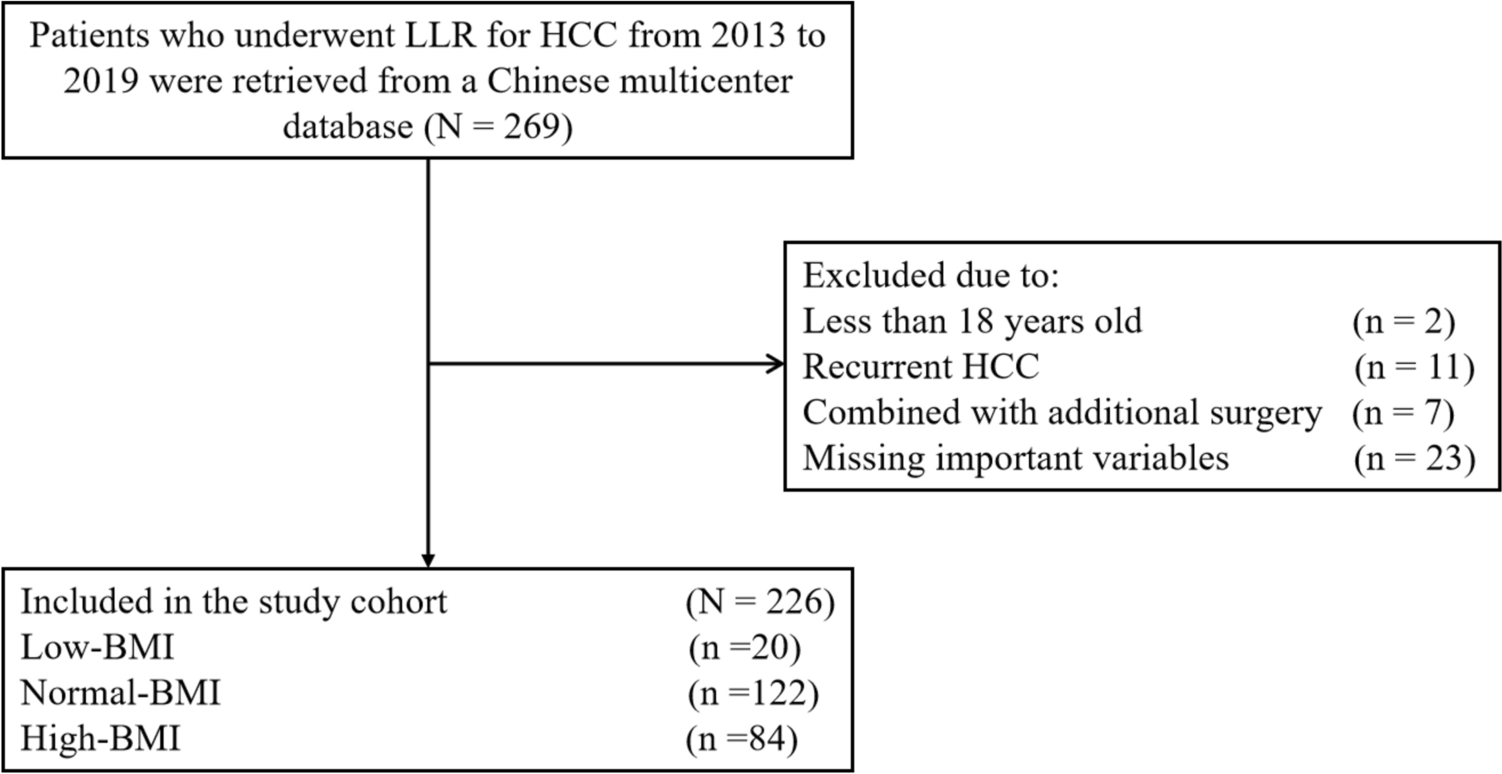
Patients who underwent curative-intent LLR for HCC between January 2013 to December 2019 at one of the four Chinese hospitals were enrolled into a database (Nantong First People’s Hospital, Nantong Second People’s Hospital, Chinese People’s Liberation Army (PLA) General Hospital, Zhongshan People’s Hospital). During the postoperative pathological examination, the diagnosis of HCC was confirmed. The exclusion criteria included: (i) age less than 18 years old, (ii) underwent open or robotic liver resection, (iii) had received liver resection with concomitant biliary reconstruction, gastrointestinal surgical procedures, splenectomy, portal-azygous disconnection, or portosystemic shunt, (iv) had a palliative liver resection, (v) within one week before LLR, patient’s BMI or liver function tests were incomplete or not available in the preoperative medical record, and (vi) an inaccurate estimate of postoperative 30-day mortality or morbidity (including the type of complications). This study was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Ethical approval was obtained from the Institutional Ethics Committee of Nantong First People’s Hospital (approval number: 2024KT260). Written informed consent was obtained from all patients for research purposes before surgery.
Baseline characteristics and operative variables
The baseline characteristics of the patients were retrospectively retrieved. In addition to age, sex, BMI, comorbidities, history of diabetes, and American society of anesthesiologists (ASA) score, other demographic characteristics were also assessed. Hypertension, cardiovascular disease, chronic obstructive pulmonary disease, and renal dysfunction were all recorded as co-morbidities. The laboratory variables, including serum hepatitis B surface antigen (HBsAg), anti-HCV, preoperative platelet count, total bilirubin, albumin, and alanine aminotransferase level (ALT), were collected. Other clinical and pathological characteristics of the patient included cirrhosis and portal hypertension, Child–Pugh grade, maximum tumor size, and number of tumors. Cirrhosis was revealed by histopathological examination. The diagnosis of portal hypertension is based on the presence of either esophageal varices or splenomegaly with a low platelet count (≤ 100 × 109 /L). Also, surgery-related factors, including intraoperative blood loss, intraoperative blood transfusion, operation time, extent of hepatectomy, and type of resection, were collected. A major hepatectomy was defined as resection of more than three Couinaud liver segments, whereas a minor hepatectomy was defined as resection of fewer than three segments. Anatomical and nonanatomical resections were defined according to the Brisbane 2000 Nomenclature of Liver Anatomy and Resections (Strasberg and Phillips 2013).
Patients’ grouping according to their preoperative BMI
According to the World Health Organization (WHO) classification (Consultation, WHO 2000), BMI was formulated by bodyweight [kg]/height2 [m2]. Based on WHO classification, three groups of patients with different preoperative BMI were classified in the current study (Consultation, WHO 2000): low-BMI was defined as BMI ≤ 18.4 kg/m2, normal-BMI as BMI 18.5–24.9 kg/m2, and high-BMI as BMI ≥ 25.0 kg/m2. Patients’ BMI was measured within one week of surgery.
Perioperative evaluation and management
Each hospital generally used the same perioperative evaluation and surgical procedures. Resection criteria were consistent over the study period (Yang et al. 2022). The technical details of the LLR have been described previously in our study (Yang et al. 2022). Generally, patients were placed in the supine or French position and the camera port was placed above or on the right side of the umbilicus under direct version. LLR was performed under CO2 pneumoperitoneum pressure at 12–14 mm Hg and 4- or 5-well method was used. Intraoperative ultrasonography (IOUS) and immunofuorence were used to detect the location of tumors and guide the resection planes, and an ultrasonic knife was utilized to predetermine the resection line. A harmonic scalpel (Ethicon, Somerville, NJ, USA) and LigaSure (ValleyLab, Inc.) were used to transect the liver parenchyma, and endoclips or Hem-o-lok clips were used to secure small hepatic vessels. The resected area was carefully checked for possible bile fistula and bleeding. The resected tumor specimens were placed in a retrieval bag and extracted through an enlarged incision site.
All patients received broad-spectrum antibiotics intravenously before surgery for 3–5 days. If the plasma albumin level was less than 30 g/L, fresh frozen plasma or albumin was given. After resection, blood tests and serologic liver function tests were performed at 1, 3, 5, and 7 days. After resection, all patients were examined by chest X-ray on the third postoperative day (POD) and by ultrasound during the first week after the surgery. Patient whose hemoglobin level was below 7 mg/dl received blood transfusions. Generally, drains are removed when no bleeding, bile leaks, or massive drainage of ascites is observed on the second or third POD.
Postoperative outcomes
Deaths within 30 days of surgery were defined as postoperative mortality, and causes of death were recorded. The definition of postoperative morbidity was any complications within 30 days after surgery based on the Clavien-Dindo grading system (Dindo et al. 2004). The severity of postoperative morbidity was categorized as minor and major morbidities. Minor morbidity was defined as Clavien-Dindo I-II and major morbidity as Clavien-Dindo III-V. The postoperative complications included acute hepatic failure, intra-abdominal hemorrhage, biliary complications, surgical site infection (SSI), pulmonary, renal, cardiovascular, and other vital organ dysfunction. On or after POD 5, postoperative hepatic failure was defined according to the “50–50 criteria” (Paugam-Burtz et al. 2009). The definition of intra-abdominal hemorrhage was a drop of hemoglobin level > 3 g/dL compared to the baseline level after liver resection, as well as any postoperative transfusion of packed red blood cells due to a decreased hemoglobin level or invasive reintervention (Rahbari et al. 2011). According to the Centers for Disease Control and Prevention’s National Nosocomial Infections Surveillance, SSI within 30 days of surgery can be classified as incisional (superficial or deep) or organ/space (A report from the NNIS System 2004). Additionally, diuretics and pleural effusions requiring paracentesis or diuretics were considered as morbidities (Ishizawa et al. 1960). An inflated level of bilirubin in the drainage was defined as a bilirubin concentration that was threefold greater than that in the serum (Koch et al. 2011). Renal dysfunction was defined as a decrease of more than 50% in glomerular filtration rate or a doubling of creatinine levels (Bellomo et al. 2004). Respiratory complications included pneumonia and pleural effusion. Other complications include postoperative acute pancreatitis, acute cholangitis, urinary infection, and cardiocerebrovascular accident, upper gastrointestinal bleeding and delayed gastric emptying. The duration of patients’ postoperative hospital stay was also documented.
Statistical analysis
SPSS version 25.0 (IBM, Armonk, New York, USA) was used for statistical analysis. Normally distributed continuous variables were expressed as mean ± standard deviation or median (range). Number (n) and percentage (%) were used to express categorical variables. For comparisons of continuous variables, Student’s t tests were used when applicable, otherwise, Mann–Whitney U tests were used. Categorical variables were compared using the Chi-square test or the Fisher’s exact test, as appropriate. Among patients with normal-BMI and low-BMI, as well as among those with normal-BMI and high-BMI, the postoperative mortality and morbidity rates, including the incidences of every complication were compared. To identify independent risk factors associated with increased postoperative morbidity following LLR, univariate and multivariate logistic regression analyses were conducted. In both univariate and multivariate analyses, odds ratios (ORs) and 95% confidence intervals (CIs) were estimated. It was considered statistically significant if P < 0.05 throughout this study.


留言 (0)