
記住我

The imaging quality of 99mTc-CNDG SPECT/CT in the sixty-three patients with NSCLC was preferable. Three-hour whole-body imaging showed that there was no obvious uptake of 99mTc-CNDG in the normal brain, myocardium, lung, bone and muscle. A small amount of 99mTc-CNDG was found in the liver, spleen, nasopharynx, synovium of joints and peripheral blood, and a large amount of 99mTc-CNDG was found in the kidney, bladder, gallbladder and intestine. The low background of the lung, brain, myocardium, bone and muscle made it easy to display lung lesions and metastatic lesions of the brain, bone and mediastinal lymph nodes, while the metastatic lesions of the liver, adrenal gland and abdominal lymph nodes were relatively difficult to display because of the high background of surrounding tissues. No adverse reactions were reported during the injection and imaging of 99mTc-CNDG.
Pathology and follow-upOf the sixty-three patients with NSCLC, 33 patients (52.4%) were clinically evaluated as operable and underwent radical resection of lung cancer plus lymph node dissection, and another 30 patients (47.6%) were clinically evaluated as inoperable and underwent radiochemotherapy. Among the 33 surgical patients, 30 patients underwent endoscopic radical resection of lung cancer plus lymph node dissection, and 3 patients underwent thoracotomy radical resection of lung cancer plus lymph node dissection. Among the 30 nonsurgical patients, 6 cases did not complete the scheduled radiochemotherapy, and 7 patients and 5 patients obtained histopathological N staging by lymph node biopsy and M staging by bone or pleural biopsy, respectively. The diagnoses of the remaining lesions were confirmed by at least one different image or follow-up imaging for more than 3 months.
For the 33 surgical patients with postoperative pathology, TNM staging was classified as stage IA in 19 patients, IB in 4, IIA in 1, IIB in 2, IIIA in 4, and IIIB in 3. For the 30 nonsurgical patients with biopsy pathology and clinical imaging follow-up, TNM staging was classified as stage IIIA in 2 patients, IIIB in 5, IIIC in 3, IVA in 14, and IVB in 6. The histopathological results of the 63 patients are presented in Table 1.
Table 1 Characteristics of NSCLC PatientsTNM staging accuracyT staging accuracyThe uptake of 99mTc-CNDG was abnormally increased in the primary tumor of all sixty-three patients. The mean primary tumor long axis diameter was 34.11 ± 20.58 mm (range 9–90 mm), and the mean primary tumor T/NT was 3.55 ± 1.78 (range 1.2–9.0). One patient with suspected ipsilateral lung lobe metastasis by CECT showed negative 99mTc-CNDG SPECT/CT, and no metastasis was confirmed by postoperative pathology. There were 2 patients with nodular pericardial invasion, 1 patient was positive on both CECT and 99mTc-CNDG SPECT/CT, and 1 patient with only 99mTc-CNDG SPECT/CT showed abnormally increased tumor activity. One patient suspected of pericardial invasion by CECT showed no abnormal tumor activity by 99mTc-CNDG SPECT/CT and was confirmed as having a benign lesion after 10 months of CECT follow-up after radical resection of lung cancer. Among the 13 patients with incorrect T staging on CECT, 7 patients were overestimated (11.11%), and 6 patients were underestimated (9.52%). Among the 6 patients with incorrect T staging on 99mTc-CNDG SPECT/CT, 4 patients were overestimated (6.35%), and 2 patients were underestimated (3.17%).
N staging accuracyOf the 33 patients who underwent surgery with regional lymph node pathological diagnosis conducted by surgical mediastinal lymph node dissection, 8 patients had lymph node metastasis, and 25 patients had no lymph node metastasis. In 22 metastatic lymph node stations, the mean lymph node short axis diameter was 9.23 ± 2.29 mm (range 4–14 mm),and the mean lymph node T/NT was 2.70 ± 1.76 (range 1.1–8.3). In 124 nonmetastatic lymph node stations, the mean lymph node short axis diameter was 6.78 ± 3.08 mm (range 3–18 mm),and the mean lymph node T/NT was 1.11 ± 0.29 (range 1.0–2.8). The differences in lymph node size and T/NT between the two groups were statistically significant (all P < 0.001). Of the 22 metastatic lymph node stations, 17 stations were not enlarged by CECT, of which 13 stations were found to have increased abnormal radioactive uptake by 99mTc-CNDG SPECT/CT, and 4 stations were found to have no increased abnormal radioactive uptake by 99mTc-CNDG SPECT/CT. Five stations were enlarged by CECT, all of which were found to have increased abnormal radioactive uptake by 99mTc-CNDG SPECT/CT. Of the 124 nonmetastatic lymph node stations, 109 stations were not enlarged by CECT, of which 2 stations were found to have increased abnormal radioactive uptake by 99mTc-CNDG SPECT/CT. Fifteen stations were enlarged by CECT, of which 8 stations were found to have no increased abnormal radioactive uptake by 99mTc-CNDG SPECT/CT. The pathological manifestations of those patients with abnormal radioactive uptake increase in nonmetastatic lymph nodes were inflammatory proliferation reactions. Of the 30 nonsurgery patients with regional lymph node metastasis diagnosis based on lymph node biopsy pathology and follow-up imaging, all these nonsurgery patients had lymph node metastasis. In 118 metastatic lymph node stations, the mean lymph node short axis diameter was 14.65 ± 5.91 mm(range 7–52 mm), and the mean lymph node T/NT was 2.10 ± 0.82 (range 1.2–5.8). All 118 metastatic lymph node stations were found to have increased abnormal radioactive uptake by 99mTc-CNDG SPECT/CT, of which 101 stations were enlarged by CECT. Among 25 patients with incorrect N staging on CECT, 10 patients were overestimated (15.87%), and 15 patients were underestimated (23.81%). Among 7 patients with incorrect N staging on 99mTc-CNDG SPECT/CT, 6 patients were overestimated (9.52%), and 1 patient was underestimated (1.59%).
M staging accuracyNo distant metastasis was found in the clinicopathological diagnosis of the 33 surgical patients, while 20 of the 30 nonsurgical patients were diagnosed with distant metastasis based on biopsy pathology and follow-up imaging. In 20 patients with distant metastasis, a total of 34 distant metastatic lesions with high uptake of 99mTc-CNDG were found, the mean metastatic lesions T/NT was 2.58 ± 0.86 (range 1.5–6.1).There were 6 patients with pleural metastasis, and both CECT and 99mTc CNDG SPECT/CT were positive. There were 5 patients with contralateral lung metastasis who were positive on CECT, and 4 patients who were positive on 99mTc-CNDG SPECT/CT. There were 9 patients with bone metastasis who were positive on 99mTc-CNDG SPECT/CT. Only 4 patients showed abnormal bone density by CECT. In 1 patient with osteoclastic bone metastasis in the rib detected by CT, 99mTc-CNDG SPECT/CT showed an abnormal radioactive uptake increase, while 99mTc-MDP bone imaging showed no abnormal radioactive uptake. There were 2 patients with benign bone lesions with abnormal bone density on CT that was suspected to be bone metastases, and 99mTc-CNDG SPECT/CT and 99mTc-MDP bone imaging confirmed that there were no abnormalities. There were 3 patients with adrenal metastasis, all of whom were positive on CECT, 1 patient was positive on 99mTc-CNDG SPECT/CT, and 2 patients did not show any adrenal metastasis on 99mTc-CNDG SPECT/CT due to the high radioactive distribution near the kidney. There was 1 patient with liver metastasis and 1 patient with subcutaneous metastasis, and both CECT and 99mTc CNDG SPECT/CT were positive. Among 6 patients with incorrect M staging on CECT, 1 patient was overestimated (1.59%), and 5 patients were underestimated (7.94%). Both patients with incorrect M staging on 99mTc-CNDG SPECT/CT were underestimated (3.17%).
The comparison of TNM staging accuracyFor all patients and surgical patients who underwent postoperative pathology, the accuracies of 99mTc-CNDG SPECT/CT in diagnosing T stage and N stage were higher than those of CECT, and the differences were statistically significant. For all patients, the accuracy of 99mTc-CNDG SPECT/CT in diagnosing M staging was higher than that of CECT, but the difference was not statistically significant. The comparison of the diagnostic accuracy of TNM stage between the two methods is presented in Table 2. The staging diagnoses of 99mTc-CNDG SPECT/CT and CECT in surgical patients and in nonsurgical patients are shown in Figs. 1 and 2, respectively.
Table 2 Comparison of the diagnostic accuracy of 99mTc-CNDG SPECT/CT versus CECTFig. 1
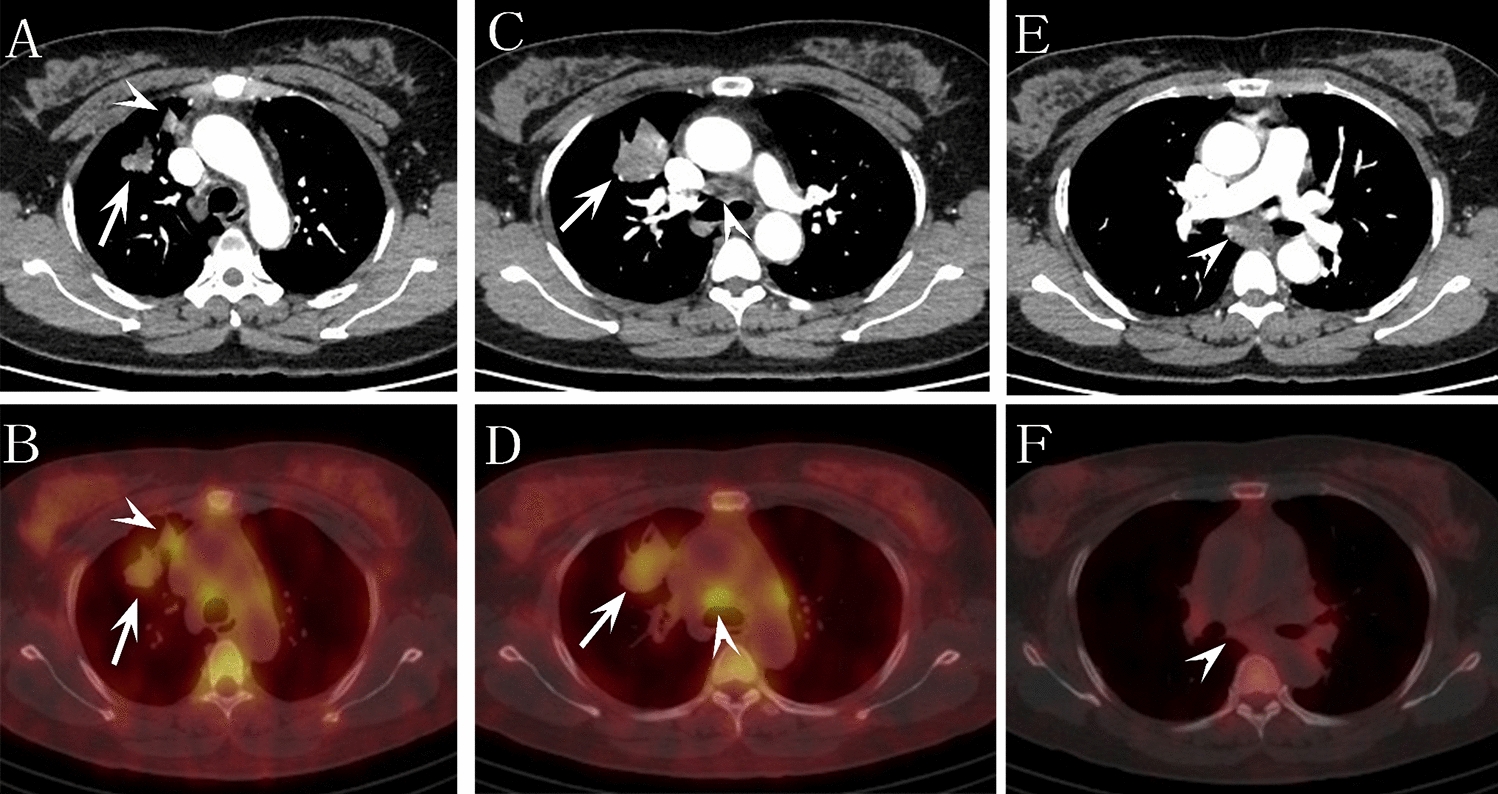
Representative case of surgery. A 50-year-old female with lung adenocarcinoma in the right upper lobe, postoperative pathological stage T3N2bM0. CECT image (A) showed that the lobulated primary tumor (arrow) and distal strip shadow (arrowhead) of the right upper lobe were abnormally enhanced, which was suspected to be right upper lung cancer complicated with obstructive pneumonia. 99mTc-CNDG fusion SPECT/CT image (B) confirmed that the primary tumor (arrow) and distal lesion (arrowhead) were highly CNDG-avid, suggesting right upper lung cancer complicated with intrapulmonary metastasis. CECT image (C) showed that the lobulated primary tumor (arrow) of the right upper lobe and slightly larger lymph node station 4R (arrowhead) were abnormally enhanced. 99mTc-CNDG fusion SPECT/CT images (D) confirmed that the primary tumor (arrow) and lymph node station 4R (arrowhead) were highly CNDG-avid, and metastatic lymph node station 4R, which was not confirmed by CECT, was definitively diagnosed by 99mTc-CNDG SPECT/CT. CECT image (E) showed abnormal enhancement of obviously enlarged lymph node station 7 (arrowhead). 99mTc-CNDG fusion SPECT/CT images (F) showed that there was no abnormal increase in CNDG in lymph node station 7 (arrowhead), and nonmetastatic lymph node station 7, which was misdiagnosed by CECT, was correctly diagnosed by 99mTc-CNDG SPECT/CT. Postoperative pathology confirmed that the lesion far from the primary tumor of the right upper lobe was an intrapulmonary metastasis, lymph node station 4R was metastasis and lymph node station 7 was nonmetastasis. Compared with CECT, 99mTc-CNDG SPECT/CT accurately diagnosed intrapulmonary metastases and differentiated mediastinal lymph node metastasis
Fig. 2
Representative case of nonsurgery. A 60-year-old male with large cell carcinoma in the left lower lobe, clinicopathological staging T4N2aM1c. CECT image (A) showed that the nodular primary tumor (arrow) of the left lower lobe and pleural nodule (arrowhead) were abnormally enhanced. 99mTc-CNDG fusion SPECT/CT image (B) showed that the primary tumor (arrow) and pleural nodule invading the left 6th anterior rib (arrowhead) were highly CNDG-avid, suggesting that the tumor had invaded the adjacent rib. A diagnostic bone window CT image (C) showed that the density of the left 6th anterior rib (arrow) near the pleural metastasis was normal. 99mTc-MDP fusion SPECT/CT bone image (D) and anterior 99mTc-MDP whole-body bone image (E) confirmed left 6th anterior rib metastasis (arrow) and left 7th anterior rib metastasis (arrowhead). Compared with CECT, 99mTc-CNDG SPECT/CT accurately diagnosed the invasion of bone by pleural metastasis of lung cancer
Potential respectabilityTo compare the accuracies of 99mTc-CNDG SPECT/CT and CECT in evaluating the potential resectability of NSCLC, the areas under the ROC curve of the two methods were calculated, as shown in Fig. 3. The accuracy of 99mTc-CNDG SPECT/CT in evaluating the potential resectability of NSCLC was significantly higher than that of CECT (P = 0.046).
Fig. 3
Graph illustrating receiver operating characteristic curves for the potential resectability of tumors with 99mTc-CNDG SPECT/CT and CECT. Potential resectability of a tumor was defined as a T stage below 4, an N stage below 3, and an M stage of 0 (99mTc-CNDG SPECT/CT: area under the curve, 0.97; 95% confidence interval, 0.89–1.00 [P = 0.023]; CECT: area under the curve, 0.87; 95% confidence interval, 0.76–0.94 [P = 0.043])
留言 (0)