Cerebellar-located glioblastoma is a rare entity, occurring only in 0.4–3.4% of all cases of glioblastoma in adults (Babu et al. 2013). The scarcity of data concerning this patient group leads to a significant deficiency in available information. This deficit hinders a comprehensive understanding of both clinical and biological characteristics inherent to this rare tumor entity. Recent published data suggest cerebellar and supratentorial glioblastoma to be characterized by significantly different frequencies of molecular subclasses (Schulte et al. 2020). Zhou et al., for example, revealed an independent role as prognostic factor of OLIG2 expression for patients with cerebellar glioblastoma (Zhou et al. 2023).
Further molecular analysis revealed that cerebellar glioblastoma themselves comprised a quite heterogeneous, methylation profile-based tumor entity with the so-called AAP subclass (anaplastic astrocytoma with piloid features) among the most frequent (Reinhardt et al. 2019). With regard to topographical, molecular and histopathological characteristics among others, cerebellar glioblastoma might imply quite different long-term outcome pattern than in case of their supratentorial counterparts.
Unfortunately, due to the rare incidence of a cerebellar glioblastoma, existing literature on survival rates of this special entity fails to present any sort of homogenous data pool. In the literature since 2000, there are currently 868 reported cases of cerebellar glioblastoma. However, studies based on cancer registries were excluded from our analysis due to concerns about the accuracy of data regarding tumor localization, the distinction between primary tumors and metastases, treatment details, and survival outcomes. This exclusion was necessary to ensure the reliability and specificity of the data we analyzed. According to our inclusion criteria, the number of cerebellar glioblastoma cases that were eligible for review is 72.
Referred to data collected from 3 up to 14 patients with cerebellar glioblastoma between 1975 and 2011, several previous retrospective studies have reported worse OS for cerebellar glioblastoma compared to supratentorial located glioblastoma (Babu et al. 2013; Gopalakrishnan et al. 2012). In contrast, analyzing a more contemporary single-center experience with 5 patients between 2002 and 2012, Milinkovic et al. in turn described a significant survival advantage of cerebellar glioblastoma patients compared to a pooled cohort of patients with supratentorial glioblastoma with an OS of 18 months (Milinkovic et al. 2014).
Such inconsistent outcome data might partly be ascribed to molecular, histopathological as well as clinical and surgical intrinsic individual features that might lead to a selection bias in a vanishingly low number of patients with cerebellar glioblastoma.
Key factors influencing glioblastoma prognosis include patient age at surgery, KPS at admission, the extent of tumor resection in terms of STR and GTR, MGMT promoter methylation status und IDH-status (Li et al. 2016; McGirt et al. 2009; Radke et al. 2019; Smrdel et al. 2016). In the present analysis, IDH-status did not significantly differ between the groups of patients with cerebellar and supratentorial glioblastoma. This is a crucial point, as the median overall survival for patients with IDH-mutated tumors is reported to be 31 months, significantly longer than the 15-month survival for those with wild-type IDH1 or IDH2 genes (Yan et al. 2009).
Furthermore, advancements in microsurgical techniques and more tailored chemotherapeutic strategies based on MGMT-promoter methylation status over the past 10 to 20 years have influenced survival outcomes. This progress, coupled with the implementation of the Stupp protocol since 2005 (Stupp et al. 2005) as the standard care, has markedly improved survival rates. Therefore, comparing current survival data with those from earlier periods (up to 30–50 years ago) may not accurately reflect the outcomes of patients treated under contemporary standards (Jeswani et al. 2013; Takahashi et al. 2014).
When discussing surgical techniques and the EOR, resection in highly eloquent regions, such as the vermis, cerebellar peduncles, and deep cerebellar nuclei, poses significant risks. These areas are crucial, for example, for motor coordination and cognitive functions, and resection can lead to severe negative outcomes. We were unable to find specific recommendations regarding the surgical management of gliomas extending to these regions, nor can we provide them ourselves.
As highlighted by Gomes et al., surgical damage to cerebellar peduncles and deep cerebellar nuclei leads to extensive white matter changes beyond the cerebellum, including disruption of connections to the cerebello-thalamo-cortical pathways, which are essential for motor control and learning (Gomes et al. 2021). The superior cerebellar peduncle, in particular, serves as the primary efferent pathway from the cerebellum, and damage to it is associated with substantial impairments in motor timing and learning tasks. Additionally, the cerebellar nuclei are critical for both motor output and cognitive processing. Therefore, resection in these regions may result in widespread and long-lasting deficits, making it a less advisable option unless absolutely necessary.
Tumor spread to the cerebellar peduncles often indicates a later stage of the disease, typically associated with brainstem invasion. Consequently, all patients in our study with brainstem infiltration, regardless of whether the tumor was supratentorial or cerebellar, were excluded. In other studies, we found no detailed information on postoperative neurological status or specific preoperative symptoms following resection in the vermis, cerebellar peduncles, or deep cerebellar nuclei.
In our patient series, one patient who underwent GTR in the vermis achieved an OS of 49 months with no unusual disability. However, it remains inconclusive whether tumor spread to the eloquent regions constitutes a contraindication for GTR. Further studies are necessary to assess the long-term outcomes of resection in these regions.
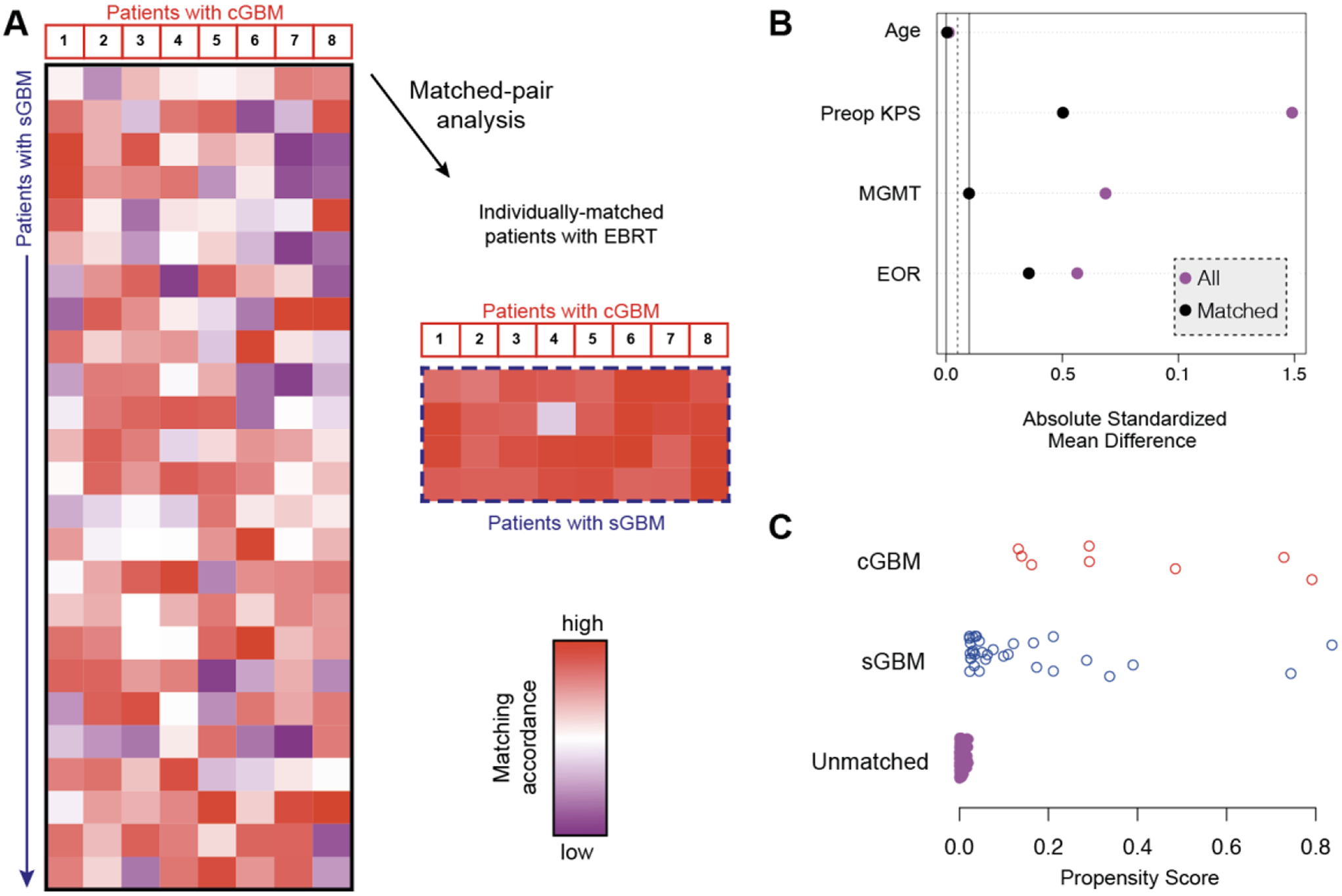
To the best of our knowledge, the present study is the first to apply propensity score matching using established prognostic factors to facilitate a more robust comparative survival analysis between cerebellar and supratentorial glioblastoma patients that had undergone surgical resection starting in 2005. Our findings suggest that survival rates for patients with cerebellar glioblastoma did not differ from those of glioblastomas located in other regions.
In particular, the OS rate of our patient cohort with cerebellar glioblastoma was comparable to the latest available data from other institutions (Milinkovic et al. 2014; Cho et al. 2019; Utsuki et al. 2012).
Further, PFS rates did not significantly differ between these entities of different glioblastoma localizations. Although there are only few publications reporting data on PFS of patient with cerebellar glioblastoma, the acknowledged data appears to be similar to our population (Hong et al. 2018; Picart et al. 2018; Milinkovic et al. 2014; Gopalakrishnan et al. 2012; Utsuki et al. 2012).
In our cohort, we observed one patient with cerebellar glioblastoma (13%) with postoperative hemorrhage resulting in early postoperative death. In the literature, there are limited reports on postoperative complications in surgery for cerebellar glioblastoma, and our systematic review did not reveal any comprehensive analysis regarding complications specifically associated with cerebellar glioblastoma surgery. Nonetheless, there is some sparse data on complications related to posterior fossa surgery, including cerebellar edema, hydrocephalus, cerebellar hematoma, and cerebellar mutism, which we address in the discussion (Dubey et al. 2009).
However, there is a lack of sufficient data from multi-center studies that allows a valid assessment of survival of cerebellar glioblastoma patients especially taking into account possible histological or histochemical heterogeneity.
Further multicenter-based studies are needed to design tailored interdisciplinary modern treatment and aftercare for patients suffering from cerebellar glioblastoma.
Limitations
The present study has several limitations. The statistical analysis and data collection were retrospective and included only a small cohort from a single institution. Given the rarity of cerebellar glioblastoma, providing Level I evidence with a Grade A recommendation is highly unlikely. Nevertheless, the use of a matched pair approach may help mitigate some confounding factors in comparisons with supratentorial glioblastoma. This approach could justify the conception and establishment of a large-scale, cross-regional database for further analysis of this rare entity. Unfortunately, due to the extended timeframe of data collection, some histological samples from the cerebellar cohort are no longer available, as certain samples have been archived since 2009. As a result, reclassification according to the 2021 WHO criteria for all eight cerebellar glioblastoma samples and further genetic analysis are not feasible within the scope of this study.


留言 (0)