
記住我
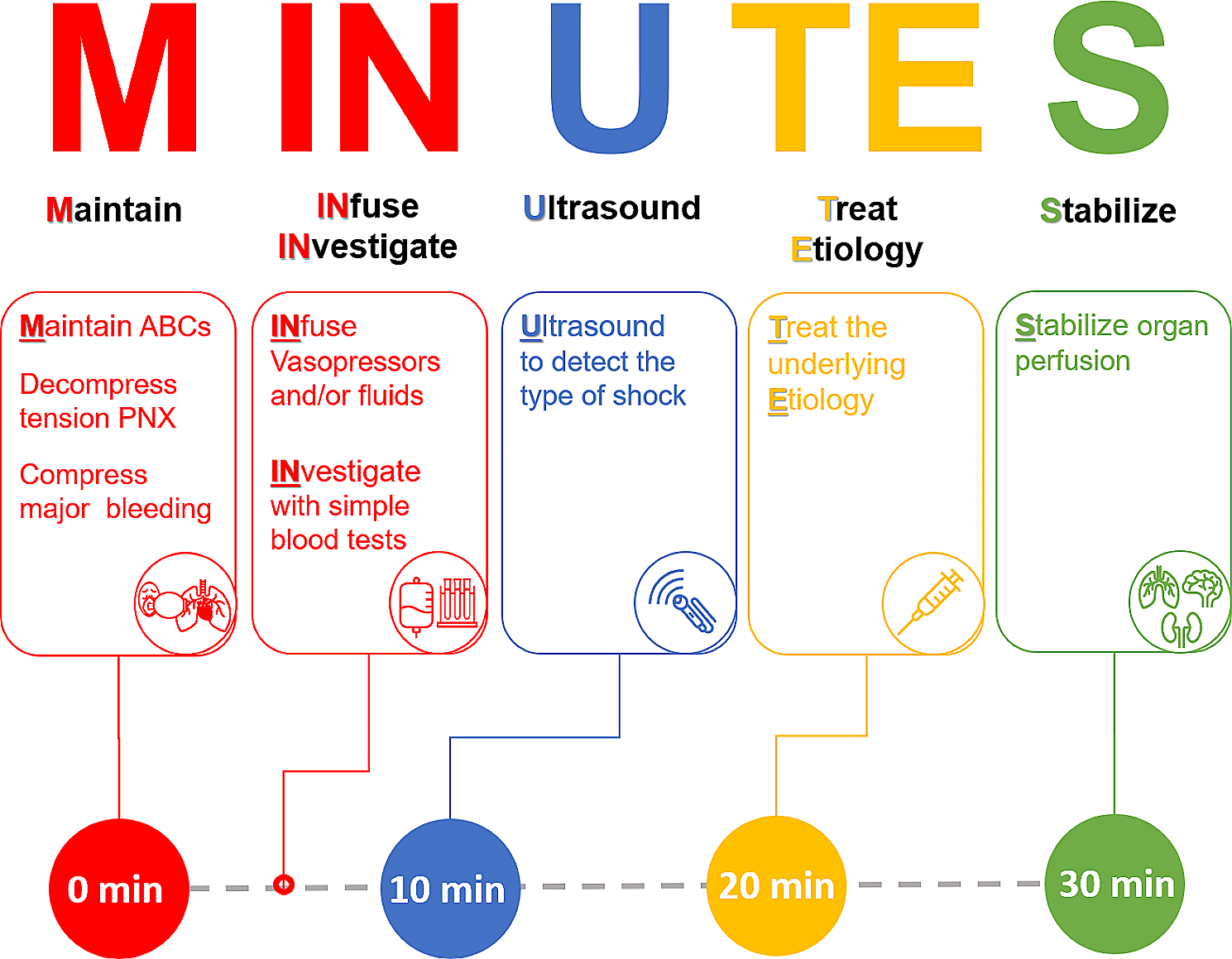

The First-MINUTES bundle includes six sequential steps: Maintain “ABCs”, INfuse vasopressors and/or fluids, INvestigate, Ultrasound, Treat Etiology, and Stabilize. The First-MINUTES bundle is summarized in Table 2, and graphically displayed in Fig. 1. In the subsequent manuscript, rationale behind each step with its associated time frame is explained.
Table 2 The MINUTES acronym to guide the initial management of undifferentiated shockFig. 1
Description of the MINUTES acronym. PNX: pneumothorax
Recognition of shockAccurate and timely detection is essential and unequivocally the most important step in managing patients in shock. Well-known bedside features of poor systemic perfusion are the three clinical windows: the brain (mental state), the kidneys (urine output), and most importantly the skin [10]. A recent systematic review of the literature has identified that reduced peripheral perfusion/temperature, prolonged capillary refill time, and a shock index (heart rate divided by systolic arterial blood pressure) ≥ 0.7–0.8 are valid clinical indicators of shock. It is important to note that the presence of arterial hypotension, although commonly present in patients with shock, must not be considered a prerequisite to define shock [8]. Compensatory vasoconstriction, particularly in young patients, may maintain arterial blood pressure within the normal range despite critical systemic hypoperfusion [11]. Although serum lactate level is a sensitive indicator of the presence of shock, hyperlactatemia can be rather unspecific [8]. Once shock is identified, the MINUTES bundle should be promptly implemented.
M - Maintain “ABCs” (minute 0)This step should be provided within the first minute of shock recognition. Providing basic and advanced life support has been well established as the initial and crucial step of resuscitation in any acutely ill patient. Therefore, ensuring airway patency, adequate ventilation, as well as presence of central pulse should be the first priorities in all patients [7, 12]. Similarly, rapidly fatal causes of shock must be identified and treated immediately (e.g., compression of external bleeding, needle-decompression of tension pneumothorax) (Table 3).
Table 3 Rapidly-fatal easily-detectable shock pathologiesIN - INfuse vasopressors – INfuse fluids (minutes 0–10)Following the ABC assessment, the mainstay of patient salvage is to restore vital organ (e.g., heart, lungs and brain) perfusion. Severe arterial hypotension can rapidly lead to myocardial hypoperfusion and death within a short period of time [1]. The term “infuse” mainly stands for infusion of vasopressors and/or fluids within a few minutes. Though fluid infusion is the first line of therapy in the initial management of shock when fluid deficit is clear, growing evidence suggests that it is safe to initiate vasopressors early in patients with septic shock in order to maintain tissue perfusion and improve venous return [13, 14]. Furthermore, excessive vasodilatation represents the most common pathophysiology of shock and requires vasopressor therapy [15]. Thus, initiation, and probably escalation, of vasopressors within the first five minutes until the etiology and type of shock have been identified is reasonable to limit the occurrence of under-perfusion and organ damage.
In case of septic shock, intravenous infusion of 30 ml/kg crystalloids has been suggested by the Surviving Sepsis Campaign within the first 3 h in patients with sepsis-induced hypoperfusion or septic shock [2]. However, fluid requirements vary substantially and such predefined volumes may result in over-resuscitation in some patients [16]. Therefore, an alternate approach has been proposed, starting with 10 mL/kg crystalloids followed by an individualized approach based on the patient response within a shorter period (one hour) than that described in the surviving sepsis campaign guidelines [17]. A similar regimen has been suggested by other authors unless clinical signs of congestion are present [13, 17]. It should be noted that fluid administration should be carefully individualized as it might be detrimental in some types of shock (e.g., cardiogenic and obstructive shock).
Whether to initiate vasopressors early or to wait for the clinical response to fluid challenge remains still debatable and likely depends on the clinical scenario and gestalt. Vasopressors may be considered early in the presence of life-threatening arterial hypotension [1], a low diastolic blood pressure < 40 mmHg, diastolic shock index > 3, or when there is a risk of fluid overload [16, 18]. It is worth mentioning that vasopressor administration could be initiated peripherally in low dilution without wasting time for central venous catheter insertion [2]. The first line vasopressor in the majority of patients with shock is norepinephrine [15].
A mean arterial blood pressure ≥ 65 mmHg appears as a suitable target during the initial salvage stage in most types of shock [2]. However, confirming adequate peripheral perfusion should not be ignored using the available indices of tissue prefusion (e.g., serum lactate, capillary refill time) [15]. In patients with hemorrhagic shock, lower targets of blood pressure values (systolic blood pressure ≈ 90 mmHg) seems more appropriate in patients without brain injury, until the source of bleeding is secured [4, 6].
IN – Investigate (minutes 0–10)After provision of life support and implementation of interventions to ensure vital organ perfusion, clinicians should swiftly proceed to basic investigations. Among these, VBG certainly seems one of the most appropriate for its ability to provide point-of-care results with information on several variables that may be useful for the management of shock and/or its underlying etiology. Indeed, results of serum lactate, hemoglobin, and glucose levels will provide ready-at-hand diagnostic and therapeutic support for clinicians. Point-of-care laboratory tests are widely available nowadays and can provide additional used data about electrolytes, cardiac markers, and kidney functions. Of course, other laboratory investigations (e.g., a complete blood count and, if appropriate, cardiac enzymes) may provide invaluable information, but their results are usually not available within the first hour. Finally, in all cases in whom acute myocardial ischemia cannot be excluded, clinicians should perform an electrocardiogram. We suggest that the timeframe to accomplish this step is within 10 min after shock has been recognized, ABCs maintained, and treatments for life-threatening arterial hypotension implemented.
U – Ultrasound (minutes 10–20)Ultrasound has several key advantages which favor its use as an initial and principal point-of-care diagnostic tool in the primary management of patients with undifferentiated shock. First, ultrasound can rapidly differentiate the pathophysiological type of shock with excellent accuracy [19], and this is particularly useful if fatal pathologies (e.g., obstructive shock) are present [10, 20, 21]. Second, ultrasound can provide useful information about fluid status (fluid responsiveness, congestion, and tolerance) whatever the type of shock is. Third, ultrasound is a cost-effective equipment which should be present in every emergency and critical care department. It is feasible in most patients without the need for expensive consumables [22]. Fourth, point-of-care ultrasound is exponentially growing [23] and has become an essential skill for all emergency and critical care physicians [24, 25]. Fifth, ultrasound has the advantage of allowing a comprehensive evaluation of several organ systems in a short time and without the need to mobilize patients, which is highly desirable under shock conditions. Accordingly, appropriate ultrasound integration in the management of patients with shock is likely to improve survival of these patients [26,27,28]. There is an increasing role for hand-held ultrasound which showed promising results in resource-limited settings [29, 30]. For all these reasons, we suggest early use of focused ultrasound examination as a crucial diagnostic step in the assessment of circulatory shock. It is clinically reasonable to perform this scan within the first 10–20 min after shock recognition, according to the availability of the device and presence of a skilled operator.
Once started, a focused ultrasound exam should answer the several questions. Does the patient have critical obstructive pathology? Does the patient have severe systolic dysfunction? Is there an obvious anatomical left-sided valvopathy (i.e., large vegetation)? Could the patient benefit from (or at least tolerate) a fluid bolus? These questions can be easily answered through a brief focused examination of the heart, lungs, and inferior vena cava [31]. Ultrasound can also rapidly detect intraabdominal collection, pneumothorax and some types of aortic dissection. Several protocols for point-of-care ultrasound examination are present for management of circulatory and/or respiratory failure (e.g., RUSH protocol) [32]. In case of inadequate views, ultrasound is still useful in evaluation of fluid tolerance (through examination of the lungs and inferior vena cava) and ruling our obstructive shock. More sophisticated examination steps could be considered at a later stage or be performed only by experienced echocardiographers. These may include precise measurement of the stroke volume using doppler echocardiography, fine evaluation of heart valves pathology and of diastolic function [24].
The timing of the ultrasound examination could vary according to both hospital facilities and practices. Some centers may have the resources to perform ultrasound even earlier [27]. This is likely to be beneficial by informing clinicians on the previously discussed use of fluids and/or vasopressors to reverse critical arterial hypotension. However, this practice might not be feasible in settings with limited resources. Therefore, maintaining perfusion should be the first priority whatever the timing of the ultrasound examination is. Nevertheless, once an ultrasound identifiable cause is on the top of differential diagnosis, point-of-care ultrasound should be a priority.
Several clinical signs can improve the diagnosis such was the presence of acute hypoxia (obstructive pathology), wide pulse pressure (distributive pathology), congested neck veins (obstructive pathology), and lower limb edema (cardiogenic pathology).
TE – Treat the underlying Etiology (minutes 20–30)Besides the pathophysiological support of circulation, treatment of the etiology of shock is the second cornerstone of shock management. Once etiology has been identified, therapeutic interventions should be directed to reverse the underlying pathology. We propose that the proper timing for this step lies after initial investigations and ultrasound, unless the primary pathology causing shock has become evident until then.
At this stage, specific management of the cause of shock should be initiated with the exception of conditions already dealt with during the early stage of the MINUTES bundle. Pulmonary embolism and cardiac tamponade are two important pathologies that should be managed appropriately in this phase. We placed these two pathologies in this phase and not earlier as their diagnosis and/or management is usually ultrasound-based [33, 34].
It should be remembered that ultrasound is not the gold standard for diagnosis of pulmonary embolism and therefore, normal cardiac ultrasound does not rule out pulmonary embolism [34]. However, according to the European guidelines, a patient with arterial hypotension and shock due to pulmonary embolism typically shows signs of right ventricular dilatation/failure. If not, other causes of shock must be considered [5]. The accuracy of point-of-care ultrasound in ruling out pulmonary embolism can be enhanced by a multiorgan approach which includes lung- and lower limb venous ultrasound examination [35].
We also highlight the importance of initiating definitive management for other causes of shock such as early antibiotic, cultures and elimination of the source in cases of sepsis [2]; hemorrhage control, transfusion and treatment of coagulopathy in patients with hemorrhagic shock [4]; as well as medical and interventional management of coronary pathologies [3].
S – Stabilize (from minute 30 on)This phase aims to stabilize systemic organ perfusion and continue vital organ support. The goal of the earlier phases of theMINUTES acronym was reversal of life-threatening disorders. Once the initial resuscitation goals have been achieved, physicians should rapidly move towards a more sophisticated and tailored correction of existing pathologies in order to optimize systemic organ perfusion and attenuate organ injury [15]. Among others, physicians will consider urine output, liver injury, electrolytes levels with re-evaluation and correction of residual acid-base and electrolyte disorders. Notably, this phase also includes the de-escalation of unnecessary hemodynamic and respiratory support, whenever possible. More detailed imaging such as computed tomography and advanced ultrasound examination can be performed. Indices of peripheral perfusion should be followed up to determine the patient response to resuscitation. Lactate clearance could be evaluated; however, the kinetics of serum lactate are usually slow and unlikely to reflect patient progression in a short period. Capillary refill time might be more appropriate for follow up in shorter periods [36].
Early management of shock usually includes infusion of fluid boluses unless clinical signs of congestion are present. Indeed, despite the increasing use of dynamic indices of fluid responsiveness to guide fluid administration, fluid overload is still a common problem in some patients due to capillary leak. Thus, searching for signs of fluid overload and considering subsequent strategies for the evacuation of fluids (e.g., diuresis) should be part of the clinical assessment, once the primary goals have been achieved [37, 38]. The wide use of focused ultrasound in critical care units over the last years has facilitated the chances to detect patients suffering from congestion with the evaluation of excess of extravascular lung water using lung ultrasound [37, 39]. Interestingly, a recent multicenter study found the coexistence of fluid overload signals in both fluid-responsive and non-responsive patients. This finding highlights the importance of performing a simple lung ultrasound examination in critically ill patients and this might direct the management plan towards a more fluid-conservative and vasopressor-based approach, if validated in larger studies [40].
留言 (0)