This is a two-year retrospective study of critically ill adult patients infected with COVID-19 that were admitted to the ICU on ventilatory support. Patients included in this study were admitted to Arrowhead Regional Medical Center (ARMC) from March 1, 2020 to February 12, 2022. ARMC is a 456-bed university-affiliated teaching public hospital that serves as a safety net hospital for the uninsured and underserved population in San Bernardino County, California. San Bernadino County is the largest geographic county in the continental United States with a diverse population of 2.2 million people in 2023. According to the 2023 Census data, the racial demographics of SBC include 56.2% Hispanic or Latino, 24.7% White, and 9.3% African American [14]. The county has a large proportion of low socioeconomic status individuals, with 13.5% of the population living below the poverty line [14].
Patients were included in the study if they tested positive for SARS-CoV-2 on a real time polymerase chain reaction test (RT-PCR) upon admission to the hospital, respiratory status either on mechanical or non-invasive mechanical ventilation for direct ICU admission. Respiratory status for the patients initially on the Medical Floor included either high flow nasal cannula or nasal cannula and later required non-invasive mechanical ventilation and mechanical ventilation. Patients with any evidence of chronic kidney disease or end stage renal disease on dialysis were excluded. This study was approved by the institutional review board at ARMC with the approval number 22 − 18. This study was also registered on clinicaltrial.gov with the ID NCT05964088. Lastly, the work has been reported in line with the STROCSS criteria [15].
Two groups were created for the analysis. The first group included patients who were directly admitted to the ICU due to their critical respiratory status from the ED (referred to as the ICU group). The second group included patients who were initially admitted to the Medical Floor with respiratory status on high flow nasal cannula or other supplemental oxygens and transferred to the ICU due to either worsening respiratory status or change in their hemodynamic conditions (referred to as the Floor group). Both Floor and ICU groups were treated with steroids according to the RECOVERY trial once the trial was published in 2021 [16]. Prior to the RECOVERY trial, the use of convalescent plasma, Remdesivir, and other monoclonal antibodies were physician dependent. Both groups had close monitoring of oxygenation with pulse oximeter and periodic arterial blood gas assessments.
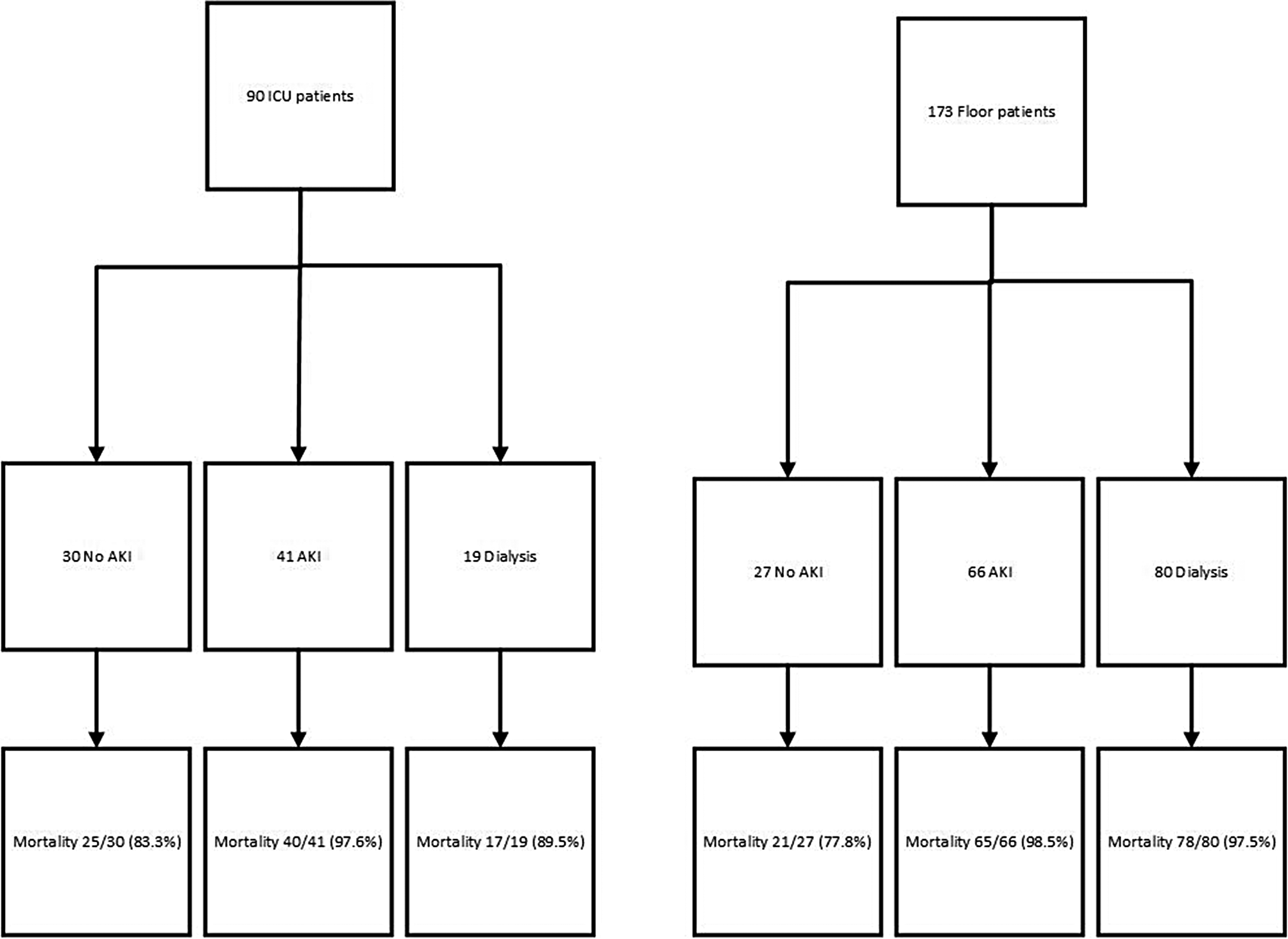
Three subgroups were created for the ICU and Floor patients separately. The ICU group was further divided into three subgroups: patients who developed AKI while admitted to the ICU (referred to as the ICU-AKI subgroup), patients who did not develop AKI during the admission and were admitted to the ICU for other Covid 19 complications (referred to as the ICU-No-AKI subgroup), and patients with previous history of dialysis dependent AKI who were admitted to the ICU resulting from other Covid 19 complications (referred to as the ICU-Dialysis subgroup). Similarly, the Floor patients were also divided into three subgroups in a similar fashion: patients who developed AKI while admitted to the Medical Floor (referred to as the Floor-AKI subgroup), patients who did not develop AKI during the course of their hospital stay admitted to the Medical Floor (referred to as the Floor-No-AKI subgroup), and patients with known history of dialysis dependent AKI who were admitted into the Medical Floor resulting from other Covid 19 complications (referred to as the Floor-Dialysis subgroup). The primary outcome of this study was mortality. The presence of comorbidities was recorded and used as a secondary endpoint. These comorbidities included obesity, T2DM, hypertension, and body mass index (BMI). All patients included in this study developed new onset AKI either directly on admission to the hospital or during the hospitalization, however for this study the AKI onset time (days) was not differentiated. The AKI was either identified on admission or throughout the hospitalization.
All statistical analyses were conducted using the SAS software for Windows version 9.4 (Cary, North Carolina, USA). Descriptive statistics were presented as means and standard deviations for continuous variables if normally distributed, or median and corresponding first and third quartile for continuous variables if not normally distributed, or frequencies and proportions for categorical variables. Independent t-test were conducted to assess the difference between floor and ICU patients for each of the three AKI subgroups separately. Analysis of Variance tests were conducted to assess the difference of continuous variables among the subgroups. Chi-square tests were conducted to assess the association between categorical variables and the subgroups. All statistical analyses were two-sided. P-value < 0.05 was statistically significant.


留言 (0)