Ethical clearance from the Institute Ethical Committee (IEC1-398/2023) was obtained as the first step. Second-year medical students pursuing a Bachelor of Medicine or a Bachelor of Surgery (MBBS) were the target group. The target was 100 students in total, with 50 in each group.
Setting
The study was conducted in Kasturba Medical College, Manipal. Online (via the Microsoft Teams platform) and onsite in our institute’s clinical skills lab/ Medical simulation centre.
Study design
Educational interventional study.
Subjects
Medical students (Year 2) from Kasturba Medical College, Manipal, who voluntarily enrolled for the simulation-based disaster training, were included in the study. (Convenience sampling was used, and the Phase II Bachelor of Medicine, Bachelor of Surgery (MBBS) students, those who consented to take part in the study (N = 103), were randomly divided into two groups- onsite Group I (N = 51) and online Group II (N = 52). The study’s objectives and methodology were explained to the students before obtaining consent. The sessions were conducted outside their regular clinical postings, and only students consenting to the study were included.
Inclusion criteria
MBBS Students who voluntarily enrolled for the simulation-based disaster training were included.
Exclusion criteria
All students who did not complete the pretest and posttest were excluded.
Duration of the study
Six months (including data collection and analysis).
Intervention
Online and Onsite Simulation-based disaster preparedness module. (see Supplementary File, Annexures) The topics covered in the module were disaster cycle, hazard vulnerability analysis, Incident command chain, and communication during disasters. It aligns with the competencies cited in the current CBME curriculum [17]. The online module used Microsoft Teams to deliver the session. The disaster preparedness module has been validated and published earlier [10].
Tools
Disaster preparedness module (see Supplementary File, Annexures); Questionnaires [Knowledge- MCQs; Confidence- Likert scale] (see Supplementary File, Annexures); feedback (Likert scale based), (see Supplementary File, Annexures). The questionnaire has been validated earlier.
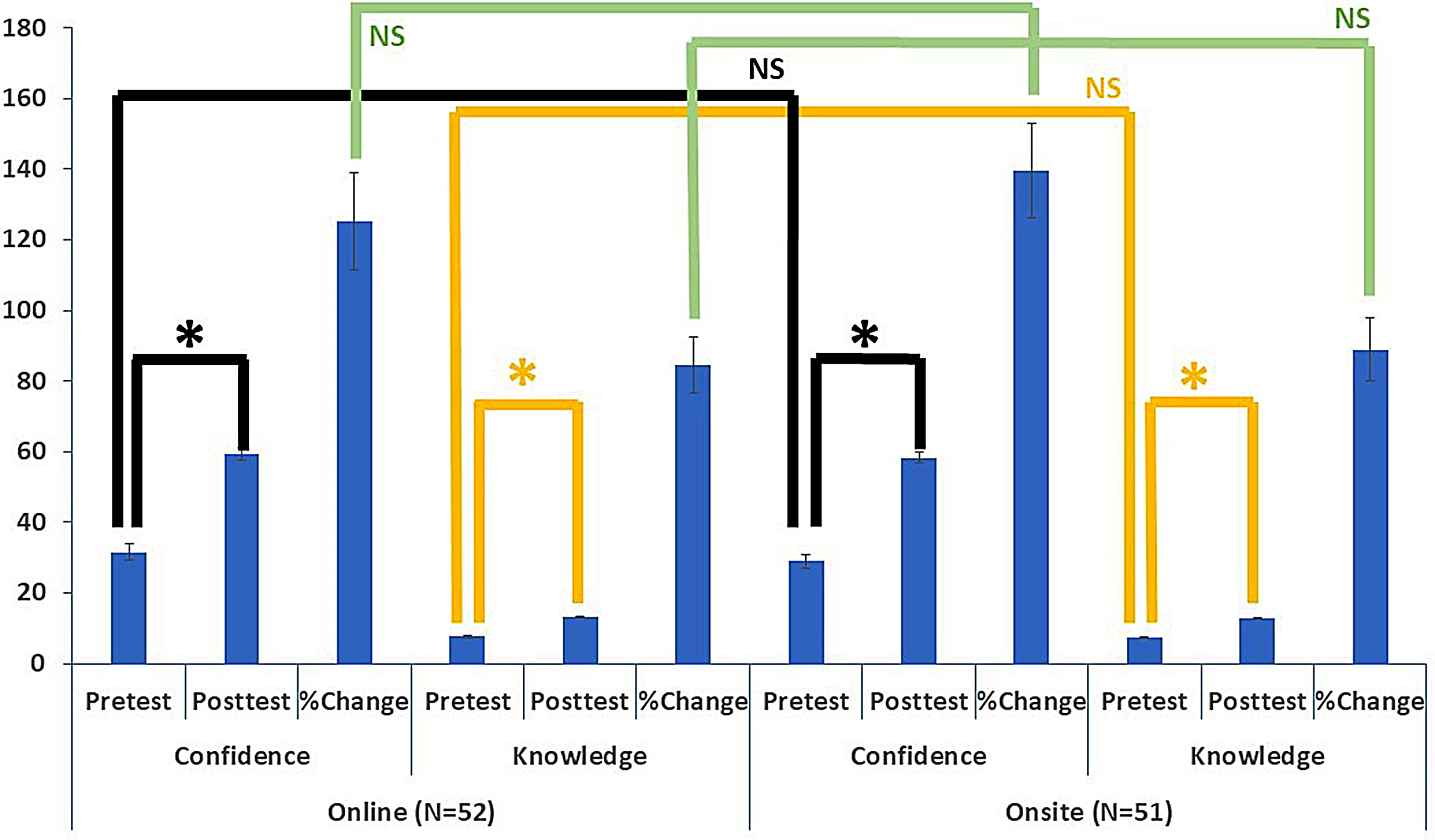
The knowledge was based on 15 single-response type multiple choice questions (MCQ), and the confidence was assessed with 15 questions based on a Likert scale of 1 to 5, where 1 = Not at All Confident, 2 = Slightly Confident, 3 = Confident, 4 = Very Confident, 5 = Extremely Confident.
Detailed description of procedure/processes
A small group of facilitators (N = 8) underwent a 2-hour onsite and online sessions training. A single person conducted this training session- the lead investigator. They were trained to facilitate small groups of five to eight learners towards completing the different sections of the tabletop exercise-based module. After training the facilitators, a tabletop exercise-based training session was announced for medical students, which was scheduled outside the regular teaching schedule. On the allotted days, outside of the routine clinical posting, the consented participants completed the pretest questionnaire via Google Forms and joined the simulation session. The participants then participated in the online tabletop exercise or the onsite workshop. The workshop lasted 3 h and was conducted via the Microsoft Teams platform (virtually) or onsite via a traditional classroom in the medical college. The same module was used for the online and the onsite session. After the workshop, the participants were subjected to a post-workshop questionnaire and feedback form via Google Forms. A single faculty (lead author) delivered the content to all the groups and received support from the trained facilitators. After the session, the participants completed the posttest questionnaire. Each simulation-based tabletop exercise lasted 60 min. All participants were exposed to three simulation-based tabletop exercises and three interactive discussion sessions as part of the module. Each group was exposed to either the online or the onsite mode of delivery as part of the study to avoid cross-contamination. All groups were, however, given the option of cross-over after participating in the study.
Statistical analysis
Statistical analysis was performed using Microsoft Excel®. The knowledge part was calculated and scored using a single response type MCQ, while the confidence and feedback were captured on a Likert scale. The mean, standard error of mean, and standard deviation were calculated for each group. Two-tailed t-tests were applied for paired analysis of within-group (online group or onsite group) and heteroscedastic analysis of between-group datasets (See Fig. 1; Tables 1, 2 and 3).


留言 (0)