
記住我

We present the case of a patient with a high risk of severe bleeding as bacterial meningitis is associated with a 2–3% intracranial bleeding risk overall, but as high as 25% in anticoagulated patients. [8] Anticoagulation is associated with a much greater risk of poor outcome or death, but earlier reversal is associated with greater survival. [9]. Some authors even argue for its preemptive reversal. [8, 10] The risk of a bleeding diathesis is further increased in anticoagulated patients with AKI. Due to its renal excretion, dabigatran’s half-life increases from 12–17 h in healthy individuals to 13–23 h in patients with moderate renal impairment (creatinine clearance [CrCl] 30–50 mL/min) and up to 22–35 h with severe renal insufficiency (CrCl < 30 mL/min) (Supplemental Fig. 1). [11] In individuals with a CrCl < 30 ml/min receiving a single dose of dabigatran, circulating levels remained detectable up to 96 h after drug administration, almost 4 times longer than healthy individuals. [3] In cases of massive accumulation, dabigatran levels remain above the expected levels for days (Supplemental Fig. 1), thus exposing patients to a prolonged increased bleeding risk. In such cases, the benefits of early anticoagulation reversal are expected to markedly reduce the risk of bleeding, even if not supported by current recommendations.
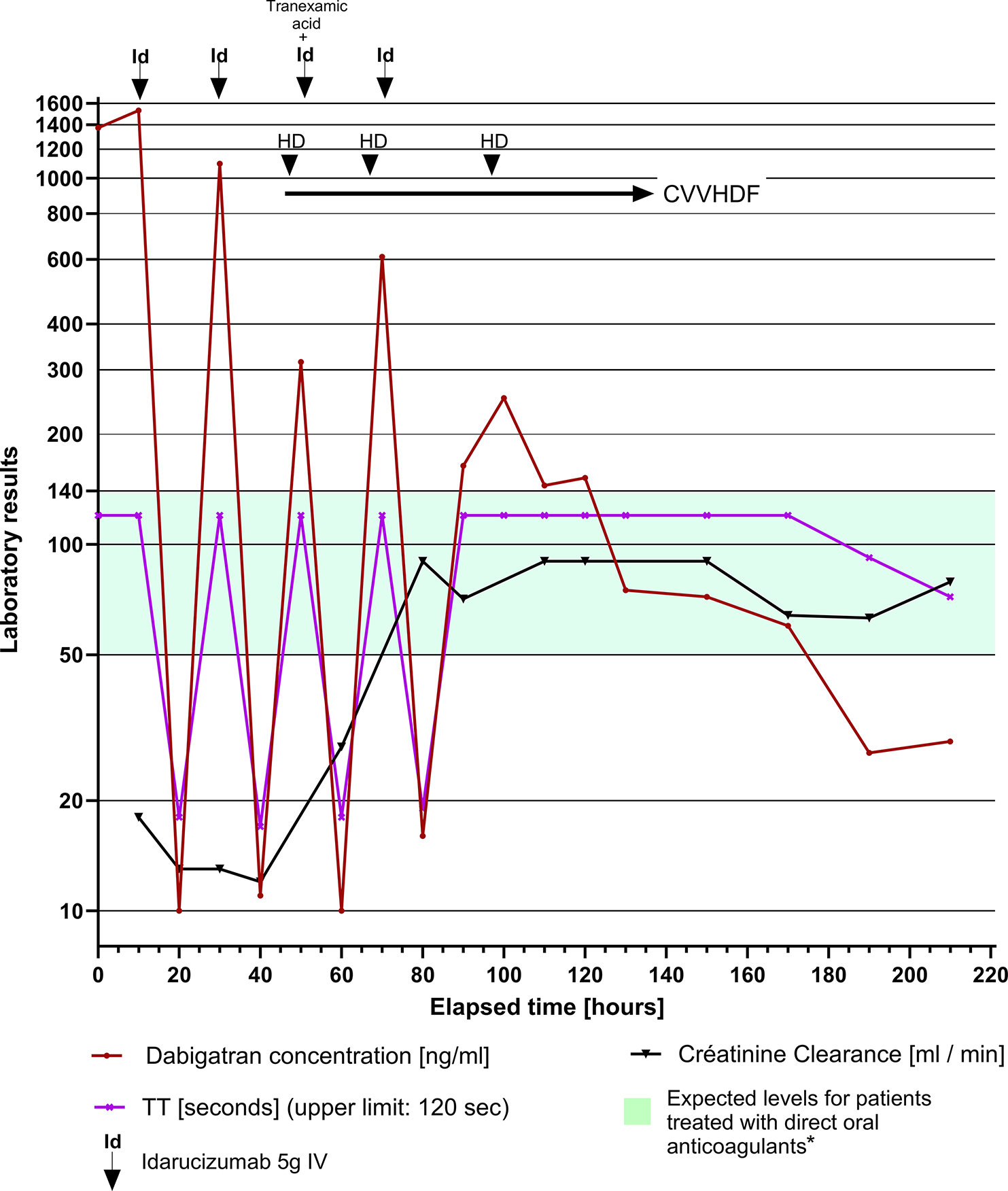
If reversal is the chosen strategy, the next question is to determine the best choice among the available options. Idarucizumab is administered as two consecutive 2.5 g intravenous boluses or perfusions over 5–10 min. However, a rebound elevation of dabigatran > 20 ng/ml, typically within the first 24 h, has been observed in up to 23% of patients. [5] This effect may be due to a free shift of dabigatran from the extravascular to the intravascular compartment, driven by a concentration gradient after elimination or saturation by idarucizumab in the intravascular compartment. Clotting parameters, in particular thrombin time, are consequently typically monitored closely during at least 24 h post-idarucizumab administration to detect this rebound. An initial concentration of dabigatran > 200 ng/ml has been recently linked to higher rates of rebound and hemostatic ineffectiveness in cases of bleeding after idarucizumab administration. [12] A modeling analysis showed that the administration of 2.5 g of idarucizumab as a 2-hour infusion markedly reduced the rebound effect compared with a bolus injection administration of 2.5 g, [13] constituting a potential new mode of administration if a sustained rather than an immediate reversal is needed. However, to our knowledge, no study has examined real-life differences between a bolus versus a 2-hour infusion of idarucizumab.
The 200 ng/ml threshold is largely exceeded in most published case reports of dabigatran accumulation and AKI. [14] In our opinion, a combination of IHD added to idarucizumab to clear dabigatran more rapidly and prevent a rebound effect and further bleeding complications should be proposed in patients with high dabigatran concentrations (Fig. 2), although evidence in the literature is sparce. A pharmacokinetic modeling analysis demonstrated that idarucizumab coupled with hemodialysis led to lower rates of dabigatran rebound. [13] Furthermore, when hemodialysis was started after a 2.5 g infusion of idarucizumab, the rebound was further reduced and anticoagulation was completely reversed. Measuring the initial concentration of dabigatran may provide clinicians with an approximate estimate of their patient’s duration of exposure concentrations above the expected levels and the associated increased hemorrhagic risk, thus guiding the reversal strategy. The choice of the type of extra-renal purification remains an open question. Some have advocated the use of sustained low-efficiency dialysis, [14] which consists in a prolonged IHD with a duration between 6 and 12 h and a reduced blood flow (100–150 ml/min), with the double advantage of being well supported in hemodynamically unstable patients, while better preventing rebounds when compared with IHD. [15]
Fig. 2
Proposed algorithm for the management of dabigatran overload, based in part on the latest publication of the French Society of Thrombosis and Haemostasis (Gendron et al., Usefulness of initial plasma dabigatran concentration to predict rebound after reversal. Haematologica. 2018 ;103(5):e226-9 and the latest French guidelines addressing DOAC reversal in emergency settings (https://sfar.org/gestion-de-lanticoagulation-dans-un-contexte-durgence/). Risk factors for dabigatran accumulation: (1) acute or acute-on-chronic renal failure; (2) interaction with glycoprotein P inhibitors (quinidine, dronedarone, ritonavir, tipranavir, nelfinavir, saquinavir, ciclosporin, tacrolimus, as well as ketoconazole or itraconazole); (3) Delirium / erroneous medication intake or administration
This case clearly underscores the need for a reevaluation of idarucizumab indications and mode of administration to avoid rebound, including the place of early hemodialysis in treating dabigatran accumulation, particularly in non-surgical patients at high risk of bleeding. To our knowledge, there are no studies assessing the potential use of idarucizumab in preventing life-threatening bleeding in such patients, particularly those with a high initial concentration of dabigatran due to AKI. This gap in knowledge warrants further investigation to enhance patient care and safety when dabigatran accumulation poses a significant bleeding risk.
留言 (0)