Accurate lower extremity DVT diagnosis and treatment are critical due to the risk of potentially fatal PE. While tools like the Wells score and D-dimer tests aid in assessing DVT risk [26, 27], imaging, particularly ultrasound, is crucial for confirming suspicions [28]. Despite being the preferred diagnostic method, its implementation is often delayed due to the requirement for trained specialists. Thus, the American College of Emergency Physicians (ACEP) emphasizes the importance of POCUS examinations performed directly by emergency physicians in high-risk patients and the need for ultrasound education [29, 30]. A notable research gap exists in determining the experience level emergency physicians need for specialist-level accuracy. Our study addresses this by quantifying the training EM residents require to diagnose DVT using ultrasound proficiently. We found that 13 cases were needed to achieve a diagnostic accuracy of 90%, and 18 cases had 95% accuracy in lower extremity venous POCUS examinations. These results provide foundational data for emergency physicians to effectively utilize lower extremity ultrasound in clinical settings.
The 2008 ACEP guidelines recommend residents complete at least 20 h of didactic education and 150 hands-on scans, including 25–50 scans per application [17, 30]. Our study, however, provided just one hour of lower extremity venous POCUS training, comprising a 40-minute lecture and 20-minute hands-on session, with no pre-study patient practice. This brief training, shorter than the 2–5 h in prior studies [18,19,20,21, 31, 32], aimed to accurately gauge the learning curve without prior ultrasound experience influencing it. Despite this, our study demonstrated that participants reached a 90% success rate after completing just 13 scans, indicating that minimal training might be sufficient for effectively implementing lower extremity venous POCUS in emergency care. This efficiency is notable compared to the recommended 20 and 25 cases for appendicitis and cholecystitis learning [33, 34].
In this study, EM residents required 1 to 1.5 years to complete the necessary lower extremity POCUS examinations, each making a few incorrect judgments. The main causes of these errors were chronic partial thrombosis (n = 3), severe leg edema (n = 3), pain-related examination limitations (n = 2), and knee flexion restrictions (n = 2). This mirrors previous studies that reported errors due to factors like unclear ultrasound images in obese patients, unusual venous courses, chronic thrombi, and misidentifications of conditions such as lymph nodes or superficial thrombophlebitis as DVT [20,21,22, 32]. Crucially, seven errors occurred following extended intervals of 2–5 months between ultrasound exams, suggesting that infrequent practice increases failure rates. This highlights the critical need for regular practice to sustain ultrasound proficiency [20, 35].
Ultrasound is influenced by factors such as the patient’s BMI and the skill level of the ultrasound operator [36, 37]. In obese patients, effective ultrasound penetration can be challenging, making diagnosis difficult. According to a study by Dua A et al. [38]. , it was recommended to opt for alternative imaging studies when diagnosing DVT in patients with a BMI greater than 40. Another study indicated that incorrect judgments were significantly associated with higher BMI levels (34.7 vs. 28.5 kg/m2, P < 0.001) [20]. However, our study did not find a significant BMI impact on DVT diagnosis, possibly because our average patient BMI (24.1 ± 3.61) was not high enough to affect results.
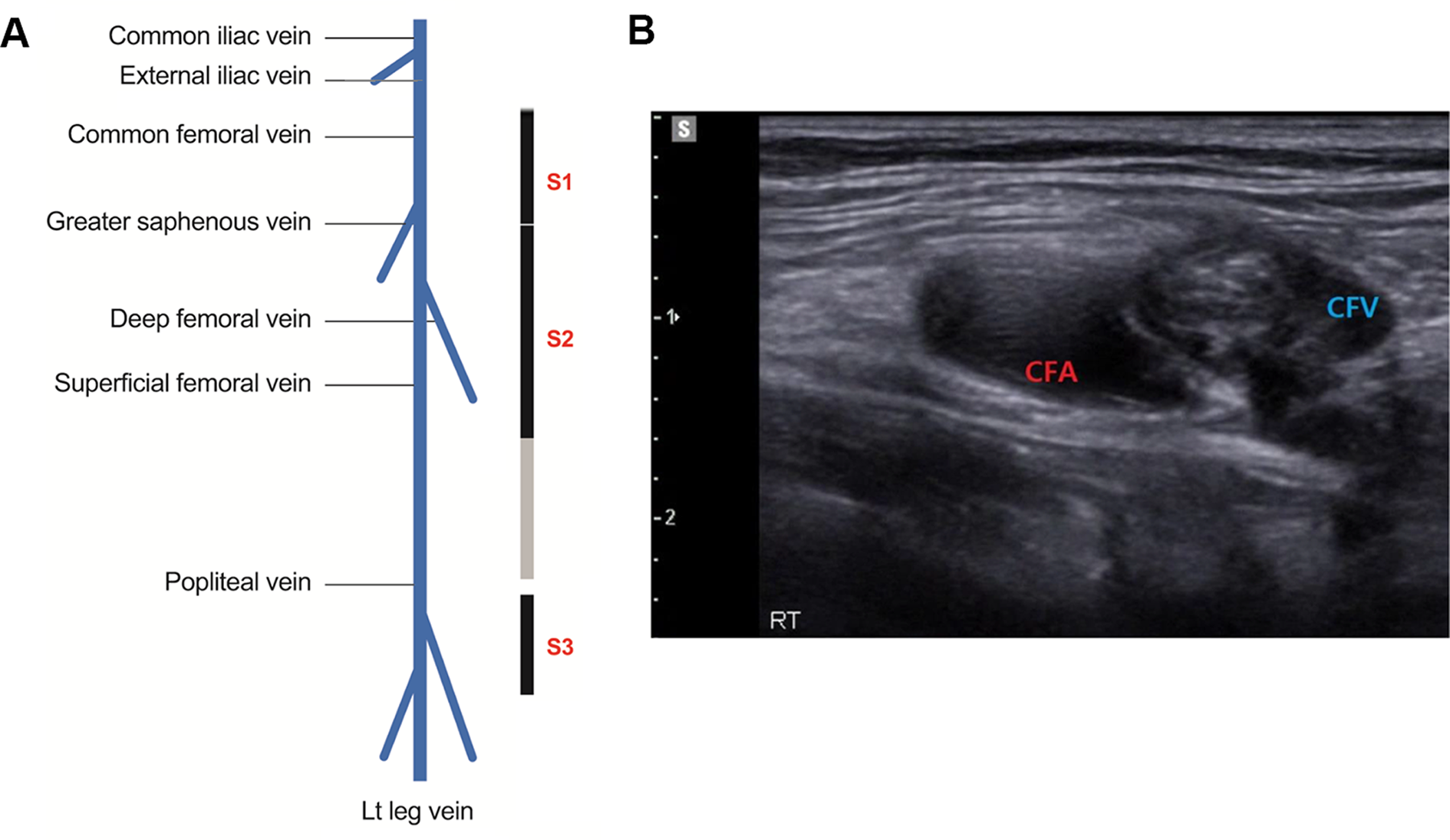
Medical institutions differ in their specialized lower extremity venous ultrasound protocols, with some focusing on specific regions and others scanning the entire leg to avoid missing isolated distal DVTs. Despite debates regarding the clinical importance of treating isolated distal DVT [39, 40], anticoagulation is recommended in high-risk cases because distal DVT can progress proximally in up to 25% of cases [41, 42]. However, ultrasound sensitivity for asymptomatic distal DVT can decrease from 74 to 50% [43], and the examinations are time-intensive. Simplified protocols covering just the common femoral and popliteal veins might miss 8% of distal DVTs but offer similar long-term outcomes [44], making them practical choices for DVT POCUS. Our study’s learning curve analysis revealed that the common femoral region (S1) was the easiest to scan, while the extensive S2 region posed challenges in acquiring high-quality vessel images. According to Caronia J.’s study, the S1 region demonstrated 100% sensitivity and 97% specificity, but the sensitivity of the S3 region decreased to 78%, likely due to the smaller size of the vein and challenges in positioning due to hip trauma, obesity, edema, and contractures [32].
The examination time, recorded from when the probe touched the patient’s skin until the scan’s end, was a median of 4 min (IQR: 3–5 min), consistent with previous studies reporting around 3 to 5 min [20, 23]. In the fast-paced ED setting, completing ultrasound examinations in under 5 min is practical for EM doctors. A reduction in examination time, while retaining accuracy, indicates growing proficiency. As shown in Fig. 4, the examination time typically decreased after 10–16 scans, aligning with the 13–18 cases needed to reach 90–95% accuracy.
The EM residents’ confidence in their diagnoses reflects the varying difficulty of cases. When doctors were 100% confident, only one error occurred in the final judgment. In cases with a confidence level of 60% or lower, all residents except EM resident 1 made errors. Table 3 indicates that each 20% increase in confidence significantly raised the odds of a correct DVT diagnosis by 2.506 times. This implies that as EM residents become more confident through experience and training, their diagnostic accuracy improves.
Our study had several limitations. First, it was conducted at a single medical institution and involved a small number of second-year EM residents with varying levels of POCUS experience. In addition, the study was conducted at a tertiary emergency center with a high proportion of malignant and severely ill patients, limiting the generalization of our results. Therefore, it is necessary to conduct research in more diverse settings. Second, to minimize the impact of prior education on learning outcomes, we did not provide comprehensive pre-training in lower extremity venous POCUS, as recommended by the ACEP. The brief one-hour preliminary training session may not have been sufficient for effective learning. Therefore, this study did not evaluate the effectiveness of POCUS education per se; however, adequate preliminary education is expected to have resulted in fewer learning cases. Lastly, it took between 1 and 1.5 years for the participants to achieve the target examination count, with breaks ranging from 2 to 5 months. These inconsistent ultrasound examinations could have negatively influenced proficiency. In addition, the accumulation of ultrasound scanning techniques and clinical experience over the years may have influenced the judgments.


留言 (0)