
記住我

A previously well 21-year-old female patient presented to the emergency department for 6 days of fever with a highest temperature of 39 °C, associated with right hip pain, sore throat, rhinorrhea, and nausea. She visited the outpatient clinic 5 days ago for right hip pain after standing up from a seated position during a parade rehearsal. Three weeks earlier, she experienced a fall backward, landing on her buttocks due to abrupt braking of the bus she was aboard. Since then, her right hip pain has persisted, being worse in the supine position, and affecting her sleep despite analgesia. She reports no vaginal discharge or bleeding.
On arrival at the emergency department, she had a temperature of 38.4 °C, heart rate of 113 beats per minute, blood pressure of 118/73 mmHg, respiratory rate of 18 breaths per minute, and an oxygen saturation of 100% on room air. She exhibited visible lethargy and shivering, along with dry mucous membranes. Tenderness was noted over the upper and outer quadrant of her right gluteus with no visible swelling, bruising or overlying skin changes. There was no midline or paravertebral tenderness over her lumbar region. Due to the pain over the right hip, she had trouble sitting upright. Examination of her throat revealed an erythematous pharyngeal wall with an ulcer noted over the uvula and left lateral wall of the mouth. Uvula was central and tonsils were not enlarged.
Investigations and treatmentA broad infectious workup was pursued. Initially investigations showed the white blood cell (WBC) count to be 3,560 / µL which increased to 18,240 / µL (neutrophils 78%) the next day. Initial C-reactive protein (CRP) concentration was 323.6 mg/L (reference < 5 mg/L) and procalcitonin concentration of 2.5 ng/mL (reference < 2 ng/mL). Chest and soft tissue neck X-rays did not show any pneumonia, epiglottitis, or prevertebral soft tissue thickening. Urine dipstick was negative for leukocytes, blood, and nitrites. Liver function test showed mildly raised transaminases. Aspartate transaminase (AST) was 39 U/L (reference < 30 U/L), alanine transaminase (ALT) was 41 U/L (reference < 36 U/L), ALP was 178 U/L (reference < 104 U/L). Blood cultures were also obtained, and the patient was started on empirical intravenous (IV) Augmentin.
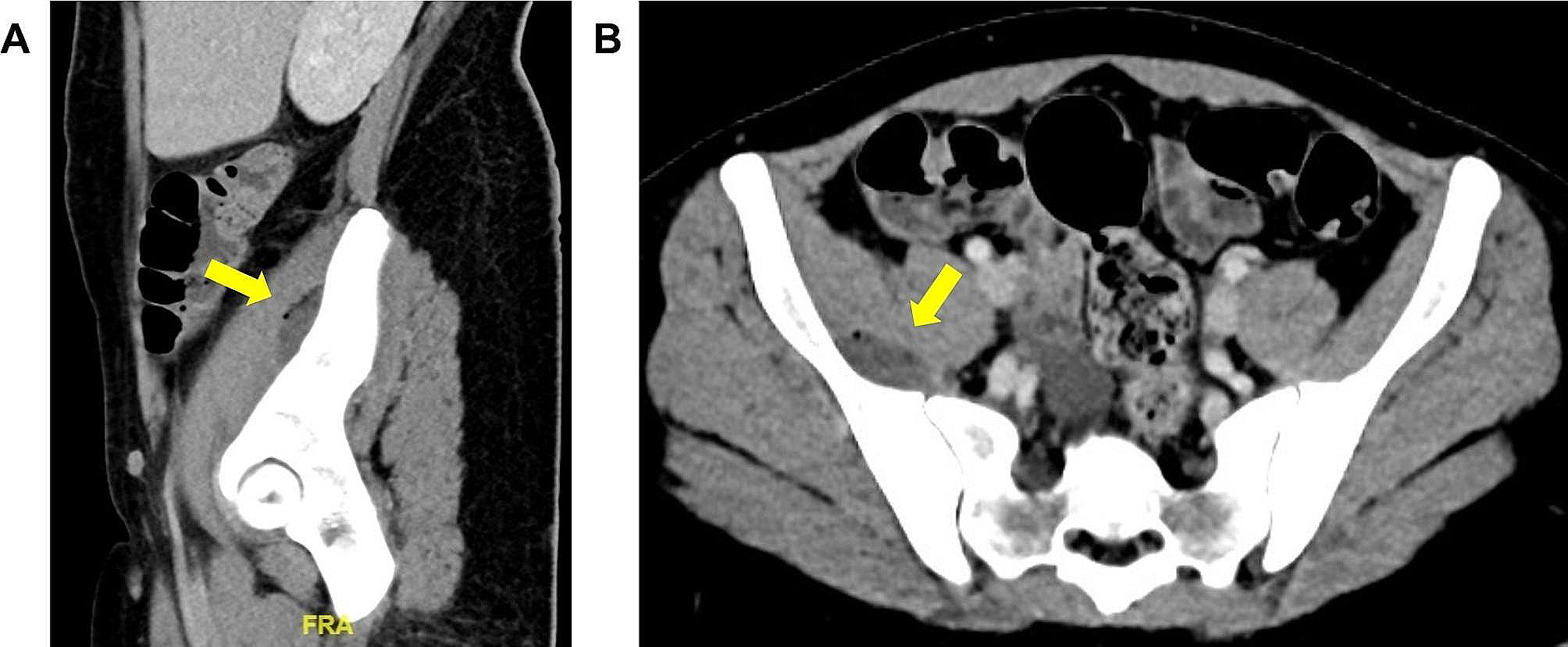
Due to the markedly raised inflammatory markers and right hip pain that seemed out of proportion, a computed tomography (CT) of the abdomen and pelvis was performed, revealing a gas-containing, faintly rim-enhancing fluid collection at the deep aspect of the right iliacus muscle overlying the right sacroiliac (SI) joint, measuring 3.4 × 1.2 × 3.9 cm (Fig. 1). A thin-walled 4.5 × 3.8 cm right adnexal cystic lesion, periportal edema in the liver, as well as patchy consolidations and ground-glass opacities were also noted in the partially imaged lower lobes of both lungs.
Fig. 1
Computed tomography imaging with contrast, (A) sagittal and (B) axial views. Arrow: a gas-containing, faintly rim-enhancing fluid collection (17 ± 8 Hounsfield unit) at the deep aspect of the right iliacus muscle overlying the right sacroiliac (SI) joint measuring 3.4 × 1.2 × 3.9 cm
The patient was referred to Orthopedics and underwent CT guided aspiration of the right iliacus collection (Fig. 2). Thirty ml of purulent fluid was aspirated which grew Klebsiella aerogenes, in line with the results of her blood culture. Acid fast bacilli (AFB) and fungal smear from the collection were negative. She was also screened for Chlamydia trachomatis, Neisseria gonorrhoea, Syphillis, Hepatitis A, B and C which were all negative. She received initial treatment with IV Augmentin, later transitioning to IV Meropenem and Ceftriaxone, and subsequently to Ciprofloxacin and Metronidazole following consultation with infectious disease specialists. Post-aspiration of the right iliacus collection, her inflammatory markers trended downwards and the pain in her hip significantly improved. She remained on oral Ciprofloxacin for a duration of 6 weeks, scheduled for a follow-up CT scan of the abdomen and pelvis 6 weeks post-discharge, along with a subsequent review by infectious disease specialists. She was also given an outpatient follow-up with Gynecology as an ultrasound of the pelvis revealed cystic lesions in the right ovary, and a non-specific vague region of heterogenous echogenicity in the anterior fundus of the uterus suspicious of a fibroid.
Fig. 2
Axial view of computed tomography guided aspiration of the right iliacus muscle abscess located approximately 8.02 cm from the skin
留言 (0)