
記住我

A 26-year-old male Caucasian patient was admitted to the Emergency Department in Aalst, Belgium for persistent red confluent facial and upper thoracic skin rash, sore throat, nausea, palpitations, fever and general discomfort in the last one week. Clinical examination showed fever at 38.7 °C, tachycardia (130 bpm) with cardiac systolic murmur, pain in the left hypochondrium, and multiple painful lymphadenopathies in the head and neck regions. The rash originated from the neck area, spreading to the face, and later extending to the back and breast regions. The arms, legs, and abdomen exhibited mild symptoms. The rash appeared as red in color, confluent, blanching, macular, and accompanied by itching.
His medical history revealed intermittent monoarthritic inflammation and hydrops of the right knee in the last 2 years, with a new exacerbation of synovitis, high sedimentation rate (65 mm) and C-reactive protein (CRP) value (92 mg/L) with limited rise of rheumatoid factor (RF; 14 U/ml) in blood one month prior. ANA-immunofluorescence and ANCA determinations were negative. Arthrocentesis results showed significantly elevated white blood cell count (14,118/mm3). Rheumatoid arthritis or spondyloarthropathy was suspected and treatment with sulfasalazine (500 mg 5 times per day) started. The patient stopped this treatment himself after 23 days because of the onset of fever and rash. The patient’s previous medical history was relatively unremarkable, there were no chronic diseases, recurrent infections, or allergies reported. He did not take any chronic medications but occasionally used non-steroidal anti-inflammatory drugs.
Laboratory investigations disclosed mild anemia (hemoglobin 11.6 g/dL), significant non-cholestatic hepatic pathology (AST 78 U/L, ALT 224 U/L, LDH 533 U/L, GGT 132 U/L, direct bilirubin 0.8 mg/dL, albumin 29.4 g/L, alkaline phosphatase 145 U/L), increased ferritin level (1325 µg/L), disturbed coagulation profile (INR 1.4), high CRP value (78 mg/L), mild leukocytosis (WBC 10,300/mm³) with eosinophilia 4.5%, immunity for EBV, influenza, measles, rubella, hepatitis A and B. Other possible causes of acute hepatitis, such as hepatitis C and E, HIV, and paracetamol intoxication were excluded. Group A Streptococci tests to exclude potential erysipelas were negative. Echocardiography showed no arguments for endocarditis, but some pericardial effusion was detected. Abdominal echography found no abnormalities.
A presumptive diagnosis of delayed onset sulfasalazine-induced toxicity was based on the presence of the skin rash and liver dysfunction, with differential diagnosis of Kawasaki disease (presence of large lymph nodes in the neck), oncological lymphoproliferative disorders like Hodgkin and adult Still’s disease (fever, joint pain and rash). Hypereosinophilic syndrome and other differentials, such as chlamydia, syphilis, borrelia and adenovirus were also sought and excluded.
Patient was positive on all 7 criteria of RegiSCAR scoring system, 6 out of 7 on Japanese consensus group (HHV-6 reactivation was not tested) and all three criteria on Bocquet, Bagot, and Roujeau (1996) (Table 1) [8].
Table 1 DRESS Diagnostic Scoring systems (“DRESS Syndrome Foundation: diagnosis and treatment,” [1], Bocquet, Bagot, and Roujeau, [8])Initial treatment was started with supportive saline infusion and antipyretic doses of paracetamol (acetaminophen; up to 2 g/day for fever > 38.5 °C). All non-steroidal anti-inflammatory medications, aspirin and sulfasalazine were withheld. The patient was transferred to the Gastroenterology Department because of the hepatic cytolysis pathology.
In the meantime, the skin rash increased with significant swelling of the face, pharynx and neck, dyspnea, coughing and hypoxia, requiring admittance to the intensive care unit the next day. Leukocytosis increased to 17,100/mm³ with eosinophilia 11% (1830/mm³). Hepatosplenomegaly and ascites developed, and pyrexia peaked at 39 °C. Several blood and sputum cultures gave no indication of an infectious agent.
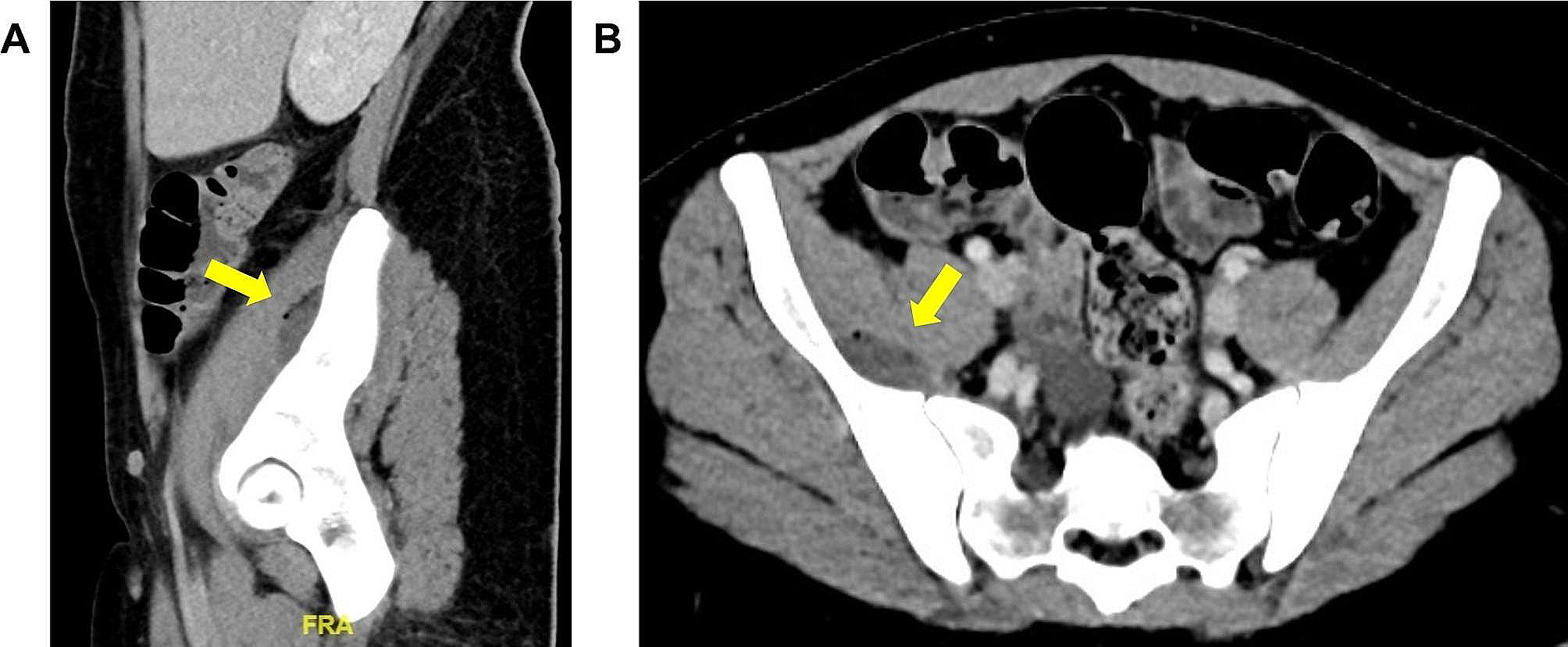
Computer Tomography (CT)-scan of thorax and abdomen showed multiple bilateral prominent lymphadenopathies in the mediastinum, the pulmonary hilum and the axillary regions. Large lymph nodes were also found along the truncus coeliacus and the right common iliac artery. Hepatosplenomegaly, right pleural effusion and massive ascites were confirmed. FDG-PET CT-scan revealed several areas of metabolically highly active metabolic areas in the head and neck and axillary regions.
The patient was further treated with corticosteroids (methylprednisolone 40 mg daily or 0.5 mg/kg/day), adequate antipyretic coverage and correction of corticosteroid–induced hyperglycemic disturbance. Following clinical improvement, the patient was transferred to the department of Oncology-Hematology two days later for further diagnosis.
Several biopsies were taken (skin, lymph node, bone marrow, Fig. 1).
Fig. 1
The pathological anatomy of the skin biopsy revealed perivascular inflammation with mainly lymphocytes infiltration (Fig. 1.1) and the focal presence of large, atypical lymphocytes CD30 positive (Fig. 1.2). No eosinophilic granulocytes were seen.
The identification of CD30 + staining, in conjunction with the findings from tomography and clinical manifestations, has significantly increased our suspicion of lymphoma as a potential candidate in the differential diagnosis. The skin biopsy staining for CD15 + was not conducted. Immunohistochemical analysis showed no pathological IgG, IgA, IgM or complement deposits.
Two lymph nodes excision biopsies showed relatively preserved lymph node structure. There is a dominance of blastoid elements on background of small mature lymphocytes and increased number of eosinophilic granulocytes. There are several blastoid cell with large eosinophilic nucleoli resembling Reed-Sternberg and Hodgkin cells (Fig. 1.3, 1.4). Interestingly, Husain et al. (2013) concluded that Reed-Sternberg cells are absent in reported cases of DRESS, while they were present in a study by Stephan et al. (2016) [9, 10]. No immunoreactivity for CD3, CD5, CD15, CD20 or CD79α was found in the large, atypical cells while the smaller cells were almost exclusively CD3 and CD5 immunoreactive T-lymphocytes (Fig. 1.5). In situ hybridization for Epstein Barr virus was negative.
Given that in situ hybridization for EBV was negative, an EBV-associated LPD, caused by iatrogenic immunodeficiency due to rheumatoid arthritis treatment, appeared to be less likely to occur. Due to the vaguely preserved lymph node structure and relatively small caliber of the CD30 it has been concluded that immunoreactive blastoid elements are more likely to be reactive immunoblasts than Hodgkin cells (Fig. 1.6).
Analysis of bone marrow biopsies demonstrated prominent eosinophilic granulocytes within the myeloid group and absence of CD30 lymphocytes. Due to the vaguely preserved lymph node structure and relatively small caliber of the CD30 it has been concluded that immunoreactive blastoid elements are more likely to be reactive immunoblasts than Hodgkin cells (Fig. 1.6). It is important to acknowledge that biopsies were obtained following administration of steroid therapy, which could have influenced the outcomes.
The patient rapidly recovered with disappearance of the skin rash, improvement of the liver function and overall decrease of the lymphocytosis. He was discharged from hospital after 10 days with supportive treatment of decreasing doses of methylprednisolone, pantoprazole, paracetamol and vitamin D substitution with calcium.
The day following his discharge, the patient consulted the Brussels University Hospital Emergency Department for relapse of acute fever (39,7° C) and thoracic and dorsal maculopapular erythema during the night. He presented with hypotension (100/52 mm Hg) and tachycardia (118 bpm). Cardiac monitoring and thoracic X-ray were normal. Abdominal echography suggested liver steatosis and splenomegaly. Laboratory data showed greatly disturbed liver tests (LDH 5508 U/L, AST 1417 U/L, ALT 2101 U/L), mild leukocytosis (10,100/mm³) with normal eosinophilic count (354/mm³, 3.5%), thrombocytopenia (52,000/mm³) and significant inflammation (CRP 53.5 mg/L). Only a few small submandibular lymph nodes were palpated. Viral serology was not tested.
The patient was admitted to the Department of Internal Medicine in Brussels, where again a dose of methylprednisolone (up to 48 mg/d or 0.6 mg/kg/day) was administered together with mometasone furoate 0.1% lipophilic cream on the skin lesions. Further investigations revealed significant hepatic cytolysis with liver steatosis, which evolved favorably under the corticosteroid treatment. The paroxysmal hyperglycemia secondary to the corticosteroid treatment was treated with insulin. Clinically neither arthritis nor synovitis was diagnosed.
The patient was discharged from hospital one week later. At home the corticosteroid dosing slowly decreased because of tremors, sleep disturbances and face swelling.
Six weeks later, liver function, leukocytosis, eosinophilic count and platelets had returned to normal values. Two months later the methylprednisolone treatment was stopped. No relapses occurred since. The patient attended two follow-up appointments, one a month later and another three months thereafter. Although further appointments were recommended, they did not occur. Laboratory analyses were conducted during these follow-ups, but imaging was not performed.
The most reasonable diagnosis was a relapse of the DRESS with reactive lymphadenopathy and hepatosplenomegaly despite treatment with high-dose methylprednisolone. The patient had a RegiSCAR score 7 out of 7 for DRESS during the relapse.
留言 (0)