
記住我

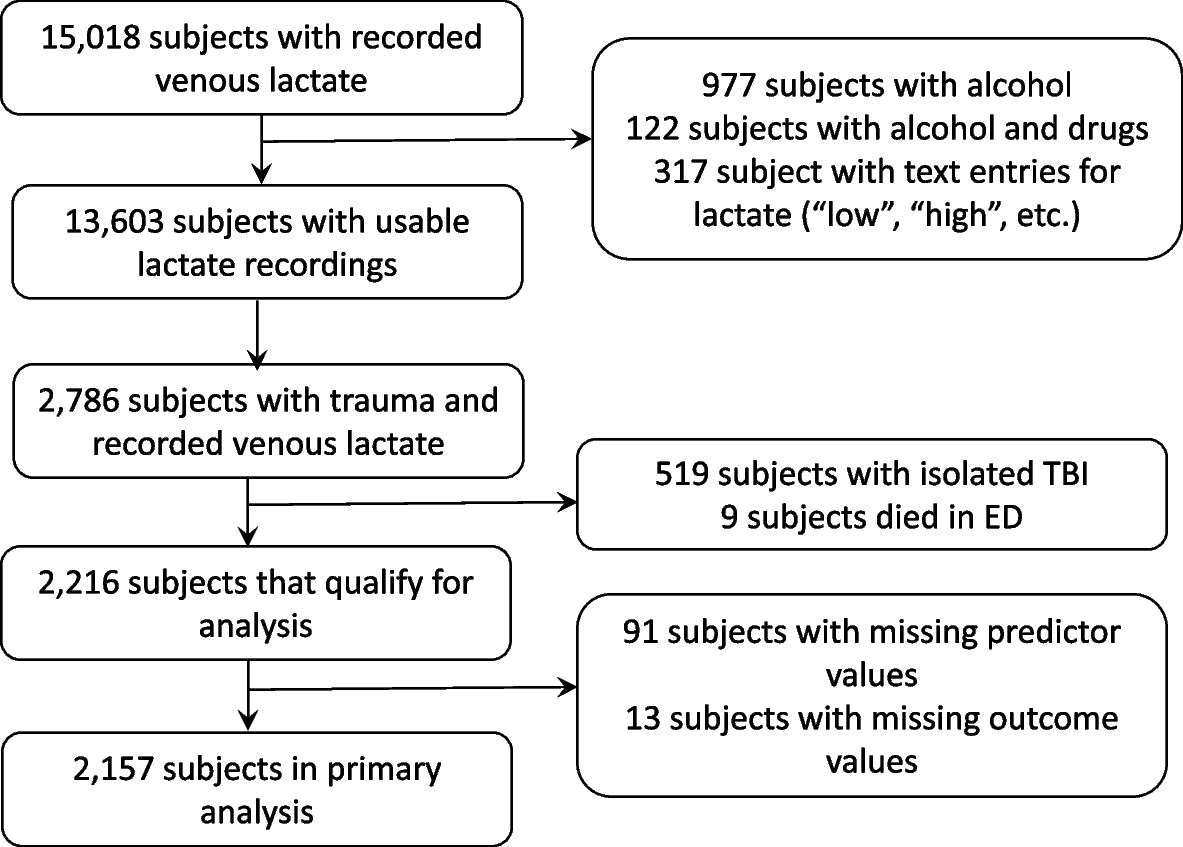
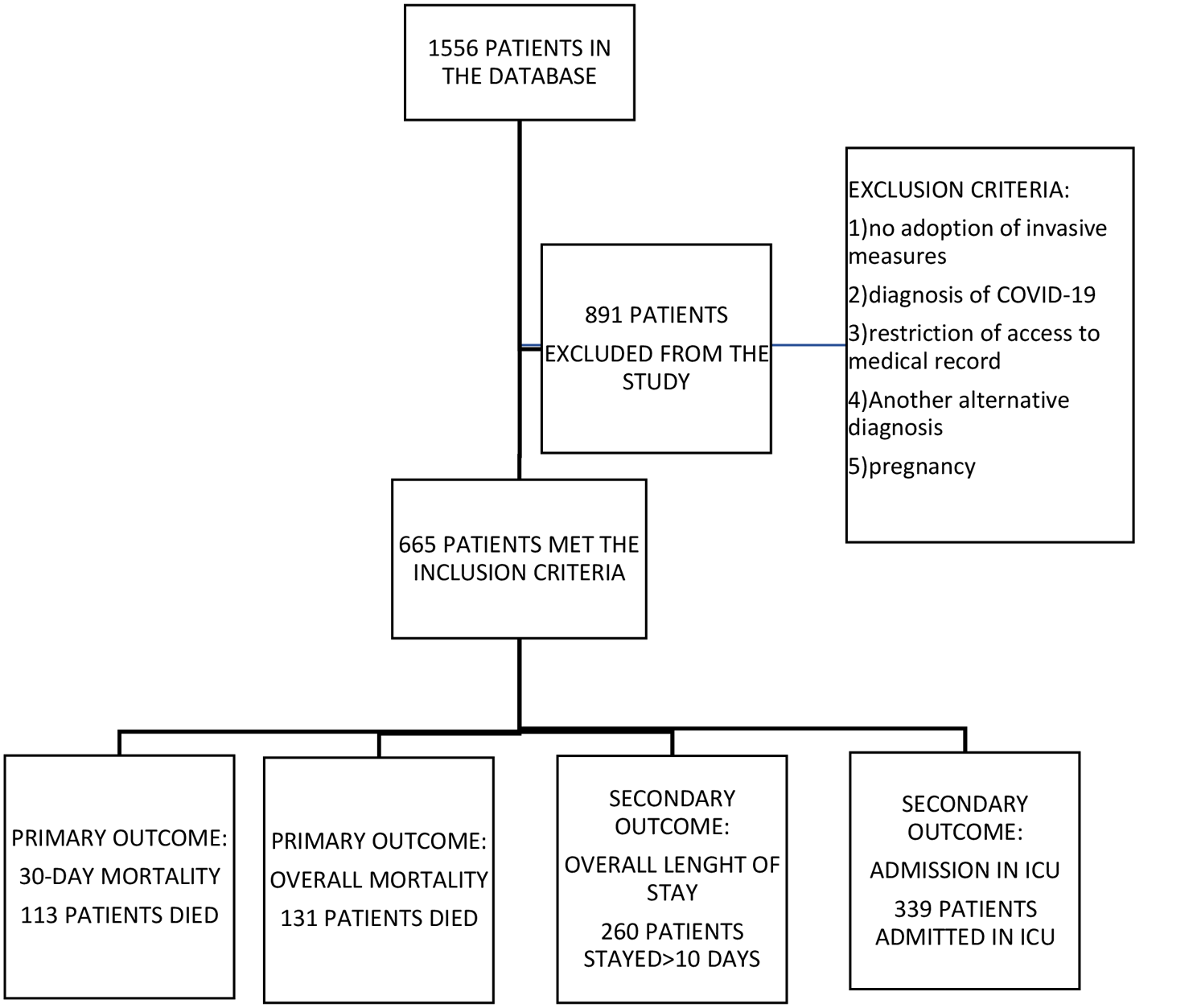
1,556 patients were admitted and assessed for infection at the ED triage. Of these, 665 patients were eligible for suspicion of sepsis during the period between January 1st, 2019, to December 31, 2020. Figure 1 shows the flowchart of the study with the number of patients included along with the results of the main outcomes found.
Fig. 1
Flowchart of the study with the main outcomes
The demographic, clinical, laboratory, and main outcomes of the population in the study are described in Table 1. The average age in the sample was 73.36 years old and 75% of the patients were elderly (≥ 65 years). The ratio of men to women was similar. The predominant site of infection found in the study was respiratory (49.77%) such as bronchopneumonia; followed by urinary tract infections (23.01%) such as cystitis and pyelonephritis; abdominal infections (12.33%) such as intra-abdominal abscesses; colitis, diverticulitis and peritonitis; and skin infections (3,01%), such as erysipelas, cellulitis and abscesses.
Table 1 Characteristics of the patients with suspicion of sepsisMost patients presented qSOFA ≥ 2 at admission, representing a group of patients with high scores and with a tendency towards higher mortality, which suggests that patients were in a severe condition at admission. In addition, 411 patients scored at least one point on the severity criteria, with most scoring only one point when they arrived at the emergency triage (53.61%).
When the patients were recognized by the protocol as potentially septic, the mean time of ATB start was 37.43 min. Patients who received the ATB were divided into three groups according to the time of administration. Approximately 34% of the patients received antimicrobial therapy within 30 min, 58.52% started between 30 and 60 min, and only 7% received it above one hour. About 17% of the patients included in the study died within 30 days, with almost half being admitted in the ICU, having around a 10-days length of stay in hospital.
Among the 665 patients included in the study, 98 patients exhibited positive blood cultures (14.74%), 505 exhibited negative blood cultures (75.94%), and 60 presented blood cultures that were considered contaminants (9.02%). Table 2 displays the bacteria detected by blood cultures in the entire cohort of patients. Among the 98 positive blood cultures, 56 were gram-negative bacteria (57.14%), 26 were gram-positive bacteria (26.53%). The most common gram-negative isolated in blood cultures was 39 Escherichia coli (39.80%), nine Klebsiella pneumoniae (9.18%), four Pseudomonas aeruginosa (4.08%), three Proteus Mirabilis (3.06%), with only one case of Neisseria meningitidis (1.02%) being detected. The most common gram-positive bacteria isolated were eight Staphylococcus aureus (8.16%), four Enterococcus faecalis (4.08%), three Streptococcus pneumoniae (3.06%), two Staphylococcus epidermidis (2.04%) that were not considered as contaminants, and nine (9.18%) other Streptococcus species, except for Streptococcus pneumoniae. Eight of the positive blood cultures were considered as other bacteria (8.16%), and eight as polymicrobial flora (8.16%).
Table 2 Bacteria isolated in positive blood culturesaTable 3 shows predictors of 30-day and overall mortality in patients with suspicion of sepsis. The reported number of deaths in 30 days was 113 (17%), while overall deaths were 131(19.7%). The univariate analysis has shown that age ≥ 65 years, three points on qSOFA, shorter times before ATB administration, and higher values of lactate were risk factors associated with higher mortality in 30 days. The same applies to other variables such as three points on qSOFA and lactate values. Positive blood cultures (RR, 1.63;95% CI, 1.10 to 2.41) and administration of vasopressors in the ED (RR, 2.14;95% CI, 1.44 to 3.17) featured as independent factors of 30-day mortality in the multivariate analysis.
When the outcome analyzed was overall mortality, age ≥ 65 years, three points on qSOFA at the triage, shorter times before the administration of ATBs (p = 0.02), higher values of lactate (p = 0.04), and positive blood cultures(p = 0.002) were only statistically significant in the univariate analysis. Administration of vasopressors at the ED (RR, 2.25; CI 95%, 1.58 to 3.21) was the only variable that was considered an independent risk factor in the non-survival group in the multivariate analysis.
Table 3 Predictors of 30-day mortality and overall mortality in patients with suspicion of sepsis according to regression analysisTable 4: shows the association among the variables studied and the secondary outcomes: overall length of stay and ICU admission in patients with suspicion of sepsis admitted in the ED. The univariate analysis showed that patients with two points on qSOFA at presentation had longer periods (> 10 days) of length of stay in hospital and patients with one point on the severity score at presentation were associated with shorter periods (≤ 10 days). The feature age ≥ 65 years (p < 0.001; RR, 1.52;95% CI, 1.19–1.93) was significantly associated with longer periods of stay in hospital along with administration of vasopressors in the ED (RR, 1.31;95% CI, 1.10 to 1.56) in the multivariate analysis. Lower values of platelets (RR, 1.01; CI 95%, 1.01 to 1.02) at presentation were also significantly associated with shorter periods of stay, but in both groups the median values were in the normal range.
Table 4 Predictors of overall lenght of stay and ICU admission in patients with suspicion of sepsis according to regression analysisConsidering the admission to the ICU, association was observed with three points on the severity criteria and higher values of creatinine in the univariate analysis. Scoring any point on qSOFA was considered as an independent factor for ICU admission (qSOFA = 1 point, p = 0.02; qSOFA = 2 points, p = 0.03, and qSOFA = 3 points, p = 0.04) in the multivariate analysis. Positive blood cultures (RR, 1.17; CI 95%, 1.01 to 1.36) and administration of vasopressors in the ED (RR, 2.50; CI 95%, 2.20 to 2.84) were also considered as risk factors when included in the model.
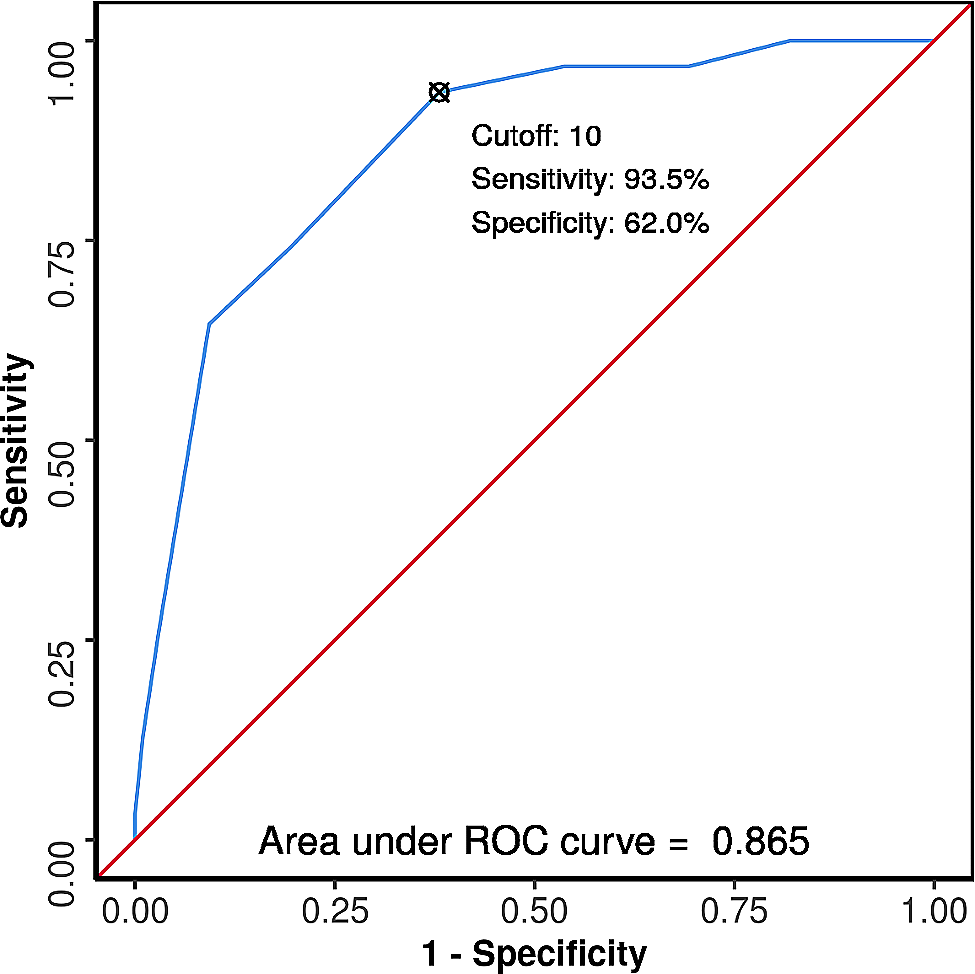
When evaluating the three different antibiotic administration intervals (less than 30 min, 30–60 min, and more than 60 min) in relation to mortality, no statistical significance was found concerning survival rates (p = 0.21). Figure 2 presents two AUROC curves estimating the accuracy of various cutoff points for the main scores analyzed, along with predictions for 30-day mortality. The highest AUROC was found for qSOFA (AUC = 0.58), and the lowest AUROC was found for the severity criteria (AUC = 0.52). A qSOFA score of two or more points was used as the reference baseline, while one or more points were used as the reference baseline for the severity criteria curve. The sensitivity for the qSOFA curve was 20% (95% CI 16%-24%), with a specificity of 87% (95% CI 82%-91%). The sensitivity for the severity criteria curve was 18% (95% CI 15%-22%), with a specificity of 85% (95% CI 80%-89%).
Fig. 2
Receiver operating characteristic curves for in-hospital mortality
留言 (0)