This was a 10-year retrospective study using prehospital data from the Sapporo City Fire Bureau. This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Sapporo Medical University (approval number: 3-1-84) on April 27, 2022. The need for obtaining informed consent was waived due to the retrospective design of this study.
Study setting
Sapporo is Japan’s fourth most highly populated city, with an area of 1,121.26 km [2] and a population of 1,938,331 in 2013 and 1,973,011 in 2022. The aging rate, based on people aged ≥ 65 years, in Sapporo City was 28.1% in 2022, which was roughly the same as the national average of 28.7%.[10]
In Japan, all emergency calls to the uniform emergency number 119 are handled by the dispatch center of the municipal fire department. Japan does not use a call triage system; hence, ambulances are dispatched to all calls, and all call dispatches are made with lights and sirens. Furthermore, since Japan does not have a non-transport protocol, all patients who do not decline will be transported to emergency medical institutions by ambulance.
Outcomes
The primary outcome was the projected number of fall-related calls among older people. The secondary outcome was the proportion of falls among older people to the projected future number of emergency calls.
Data collection
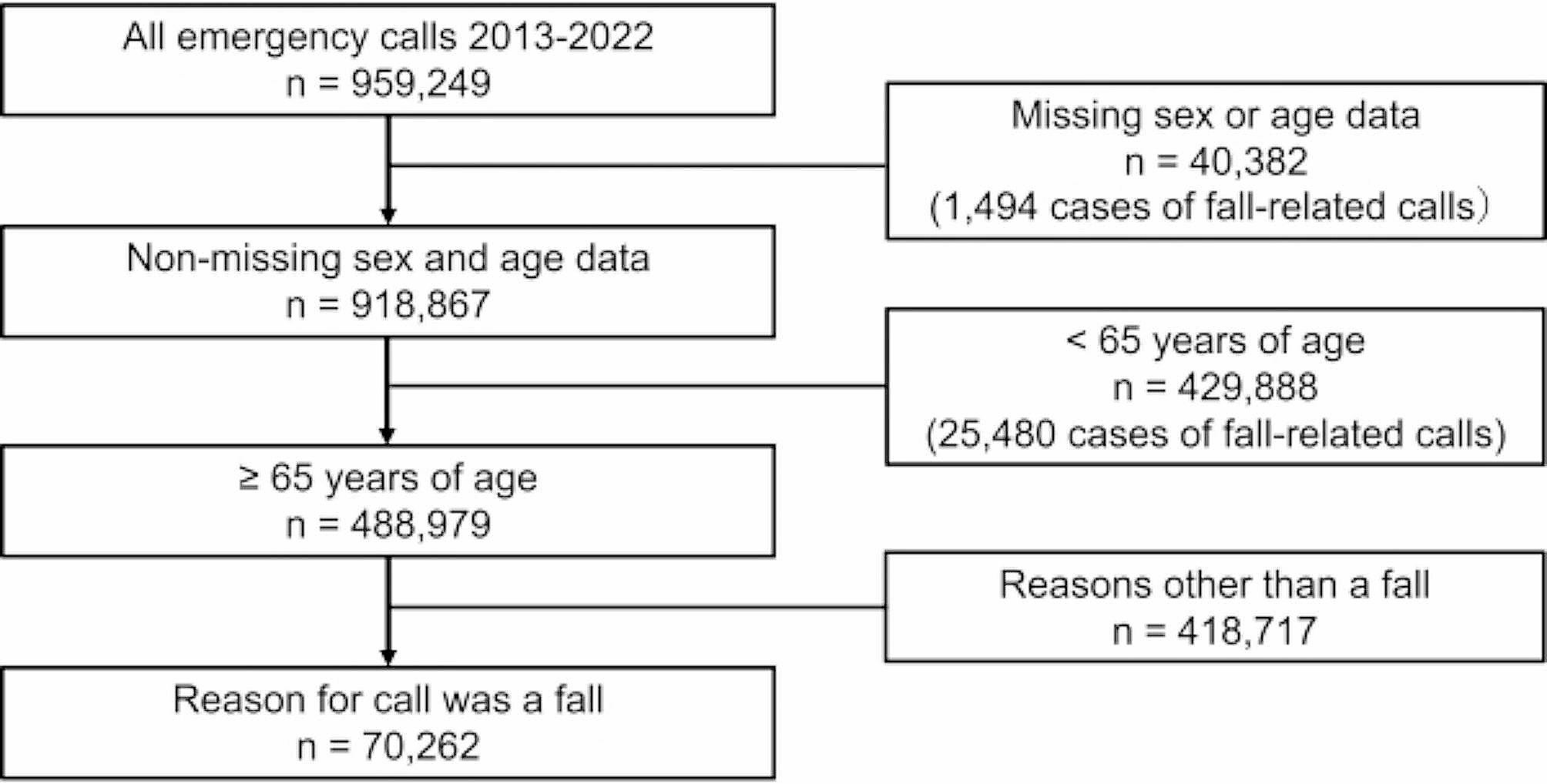
We reviewed all patient data for emergency calls in Sapporo City during the 10-year period from January 1, 2013, to December 31, 2022, using the Sapporo City Fire Department patient registry. Patients aged ≥ 65 years who were referred for ambulance transport due to a fall were eligible, except for those whose sex and age were unknown. We analyzed the number of emergency calls for each year by sex, age (in 5-year age groups), and whether the fall occurred indoors or outdoors. Indoor falls were defined as falls in roofed areas, such as the home, workplace, older adult care facility, or public facility. Outdoor falls were defined as falls outside or on the premises of a building but without a roof and were checked at the discretion of each EMT.
The sex and age (in 5-year age groups) of Sapporo City’s population are based on the figures from the Basic Resident Register of the Sapporo City Hall Database as of July 1 of each year [11]. We used future population projections of Sapporo City between 2025 and 2060, as estimated by Sapporo City Hall, to estimate the number of fall-related calls in the future [12]. (Supplementary Table 1). The cohort factor method was used with the population by sex in the 5-year age group from the Ministry of Internal Affairs and Communications Statistics Bureau “Population Census” as the reference population. The annual changes that occur with aging in the age-specific population utilized factors such as fertility rate, sex ratio at birth, survival rate, and net migration rate.
Data analysis
The annual fall-related call rate by age group (5-year age groups) in those ≥ 65 years old was calculated by sex by dividing the number of fall-related calls by the population of each age and sex subgroup. The same calculations were performed separately for indoor and outdoor occurrences. The difference in rates of fall-related calls between males and females was tested using Student’s t-test.
Age standardization was performed by the direct method using the average age distribution of 5-year-old male and female groups in Sapporo City from 2013 to 2022 as the reference population. At age ≥ 65 years, linear regression analysis was performed on the bivariate relationship between the number of fall-related calls per 100,000 population and annual trends by sex. To consider the influence of the COVID-19 pandemic, we divided the analysis into two periods, 2013–2019 and 2013–2022 [13].
Four calculation methods were used to obtain future estimates from 2025 to 2060. The first is the call rates by sex and age group in 2022, which were multiplied by the respective estimated future population and summed. The second used trends identified from 2013 to 2022 to make projections for the future. Poisson regression models, including sex, age group, and calendar year, were used [13]. Using the maximum likelihood method, the Akaike Information Criterion (AIC) was used as a measure of the predictive ability. The third method employed machine learning using the neural network model. Neural networks can model non-linear relationships in data, making them particularly useful for complex forecasting tasks. Specifically, we used the 2013–2022 data, with sex, age group, and calendar year as explanatory variables. Nested cross-validation was performed to prevent machine learning overfitting as much as possible. For cross-validation, the data were divided into four nested groups. The fourth group was used as the test set, and the remaining data were further divided into five equal groups. One subgroup of the internal folds was treated as the validation set, and the model was trained on the remaining data. In total, 4 × 5 models were fitted (K = 4, L = 5). The fourth was done the same way as the third but with a model using the years 2013–2019, which is unaffected by the COVID-19 pandemic. The number of emergency calls for each year was obtained by fitting the predictive models to the predicted population in age group, by sex, from 2025 to 2060 and summing the results. Each future estimate was calculated for falls-related calls and all emergency calls, respectively, as well as for the percentage of falls-related calls in all EMS calls. Falls-related calls were calculated separately for indoor and outdoor calls.
Analyses were performed using JMP software (JMP Pro 16 for Windows, SAS Institute, Cary, NC, USA).


留言 (0)