
記住我


Gallbladder stones and main bile duct stones are common among older people and the incidence increases with age.1 Endoscopic retrograde cholangiography (ERC) is the current gold standard treatment for choledocholithiasis.2,3
To prevent recurrent biliary events patients are typically referred to laparoscopic cholecystectomy after ERC. Nevertheless, earlier studies have reported 2.1% to 19% of patients undergoing cholecystectomy may later develop main bile duct stones.4,5 Furthermore, while morbidity and mortality after laparoscopic cholecystectomy is low, complications do occur, and especially frail older patients have significantly increased risk of adverse outcome.6–9 Consequently, a wait-and-see strategy is often chosen for those at high risk based on clinicians’ decision or patient’s own will.
There is limited evidence in the elderly of whether laparoscopic cholecystectomy after successful ERC and sphincterotomy is required.8 The problem typically arises when especially frail older patients undergo ERC. Hence, here we aim to report long-term outcomes of a wait-and-see strategy after ERC among patients 75 years or older.
PATIENTS AND METHODSThis study was performed between January 2010 and December 2018 in two tertiary academic teaching university hospitals. All available information regarding each treatment episode associated with the consecutive patients 75 years or older undergoing ERC due to choledocholithiasis or biliary pancreatitis without later cholecystectomy were included. Decision to refrain from surgery was based on surgeons' decision or patients' own will. As some patients had moved to other health care districts and were operated there, we searched the national Care Register for Health Care to complete our data. These data include all operations performed in the study country. Patients with earlier cholecystectomy, no clear evidence of main bile duct stones, hepatobiliary cancers or benign strictures were excluded (Supplemental Digital Content, https://links.lww.com/TA/C814).
The primary outcome was to define the incidence of biliary morbidity among those undergoing wait-and-see strategy after ERC. The ERC-related adverse events were defined and classified according to Cotton classification.10 Secondary outcome measures were postoperative morbidity and mortality. Surgical complications were defined and classified according to Clavien-Dindo classification.11
All statistics were analyzed using SPSS Statistics version 26 for Windows (IBM Corp, Armonk, NY). Frequencies were used to calculate counts and percentages of demographic characteristics, post-ERC complications and later biliary events. To present 1-year cumulative biliary events a crossover analysis was performed. Kaplan-Meier curve was used to demonstrate cumulative biliary related recurrence. Times were calculated from ERC until the time of later biliary event, death, or end of the study period.
The study protocol was approved by Medical Directors of the study hospitals. Being a registry-based study, approval from the ethics committee was not sought.
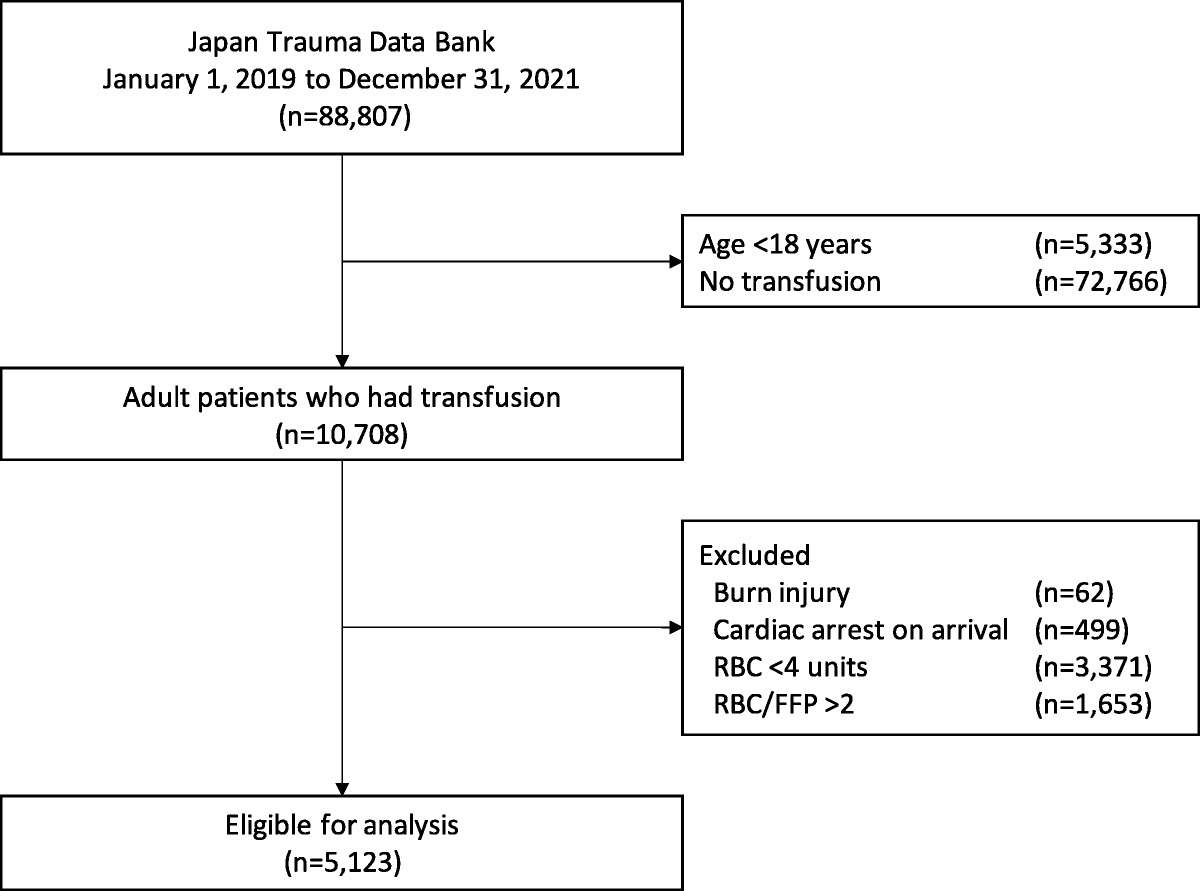
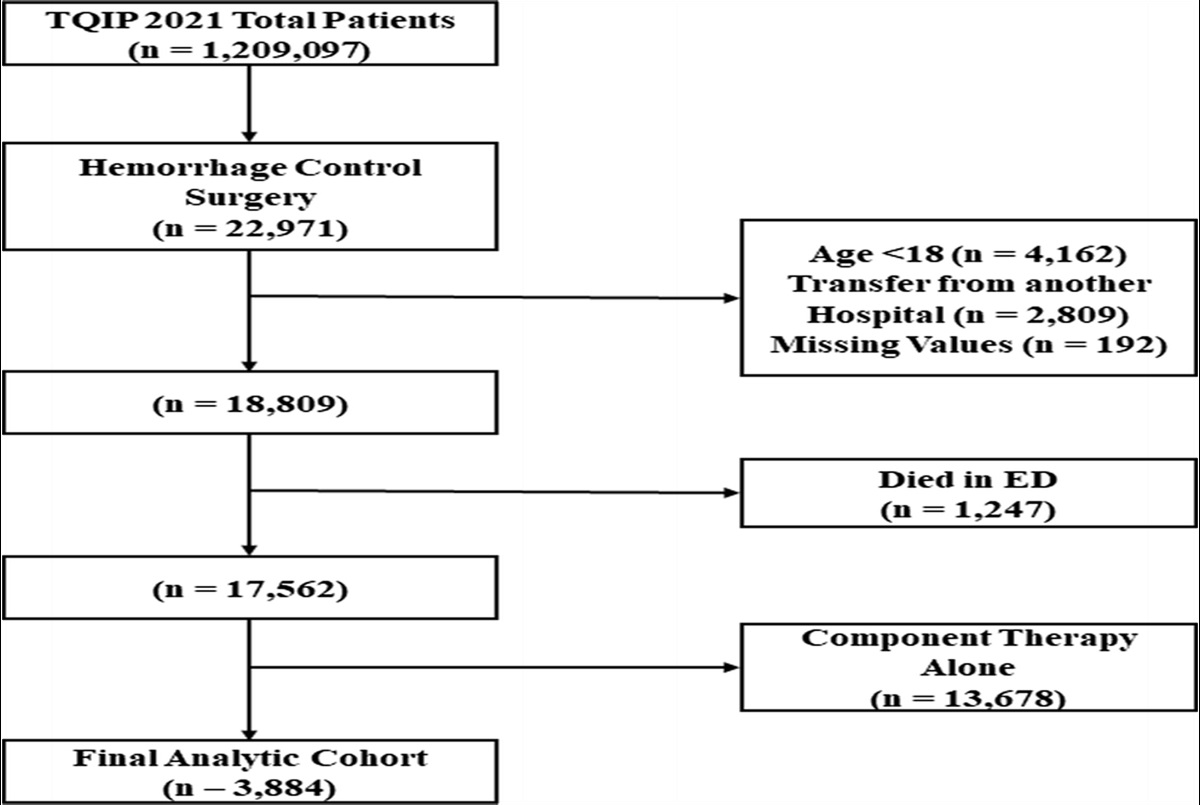
RESULTSPatient flowchart is shown in Figure 1. A total of 450 patients (median age, 85 years [75–97 years]; 61% female) were included, with a median follow-up time of 36 months (0–103 months). Patient-specific characteristics and ERC-related outcomes are presented in Table 1. The majority of patients had significant comorbidities (96%), of which the most common were cardiovascular diseases (86%), neurological diseases including dementia (33%) and diabetes (22%).
 Figure 1:
Figure 1: Patient flow diagram.
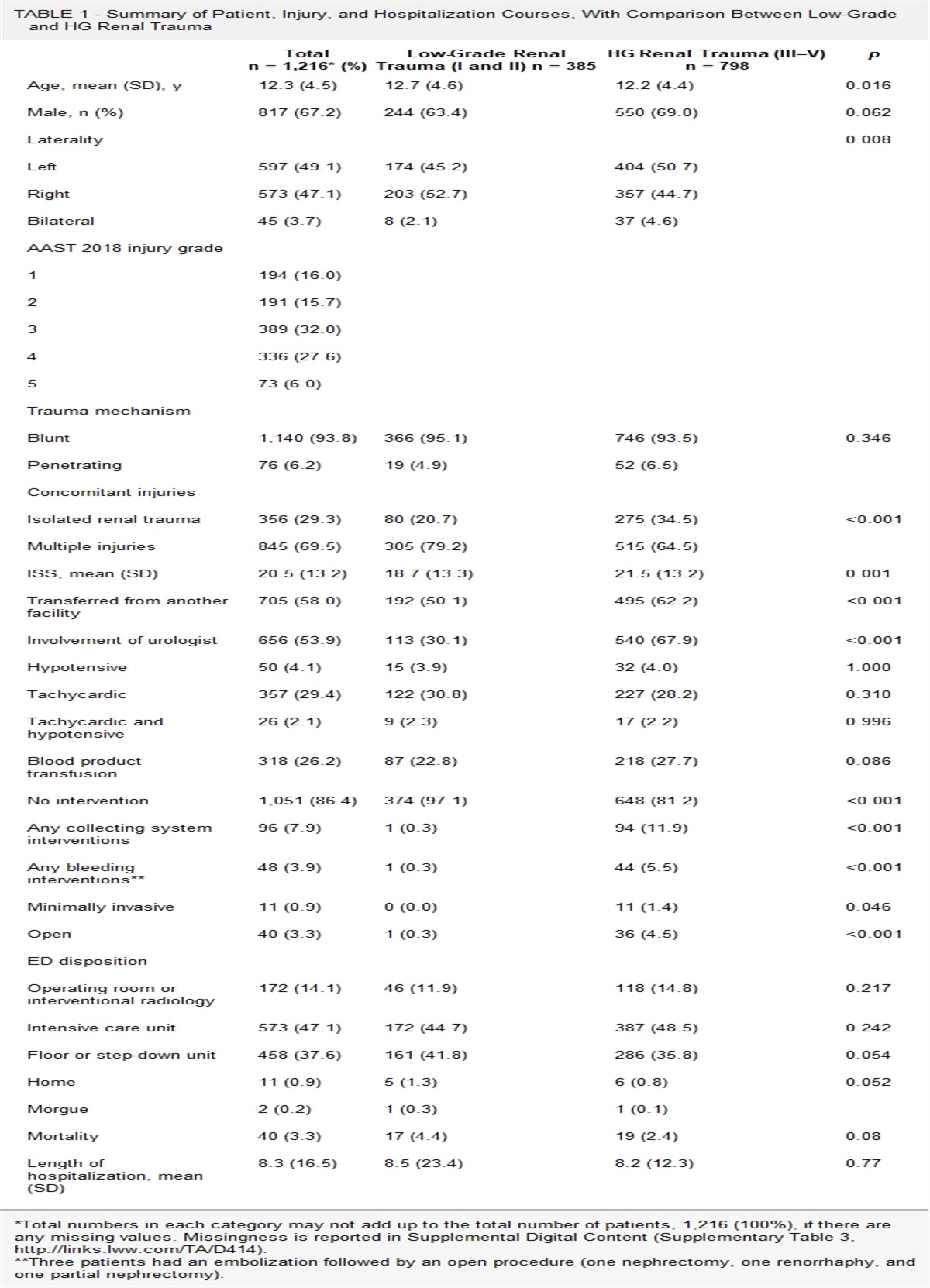
TABLE 1 - Patient and Operation-Related Characteristics (n = 442) Variables Age, median (min–max), y 85 (75–97) Sex, female (%) 274 (61%) Comorbidities 430 (96%) Cardiovascular disease 387 (86%) Neurological disease 147 (32%) Diabetes 101 (22%) Pulmonary disease 75 (17%) Psychiatric disease 19 (4.2%) Chronic alcohol abuse 2 (0.4%) Post-ERC pancreatitis 10 (2.2%) Post-ERC bleeding 8 (1.8%) Post-ERC perforation 6 (1.3%) Post-ERC infection 6 (1.3%) ERCP-associated mortality 2 (0.4%) 30-d Mortality 12 (2.7%) 90-d Mortality 23 (5.1%) 360-d Mortality 66 (15%)Later biliary-related events are shown in Table 2. Fifty-one patients (11.3%) managed with a wait-and-see strategy suffered from subsequent biliary events, of which the most common was acute cholecystitis (n = 32, 7.1%). Overall, 18 patients (4.0%) required new ERC and 16 patients (3.5%) underwent laparoscopic cholecystectomy. Only one of the laparoscopic cholecystectomies was converted open. There were no operation-associated deaths among those undergoing later surgical or endoscopic interventions. Postoperative morbidity was not increased. There were four known deaths associated with recurrent biliary events (0.9%). All of these patients had major comorbidity and were anesthetic inoperable during the initial hospital stay. One patient (0.2%) required laparoscopic cholecystectomy due to gallstone-related symptoms.
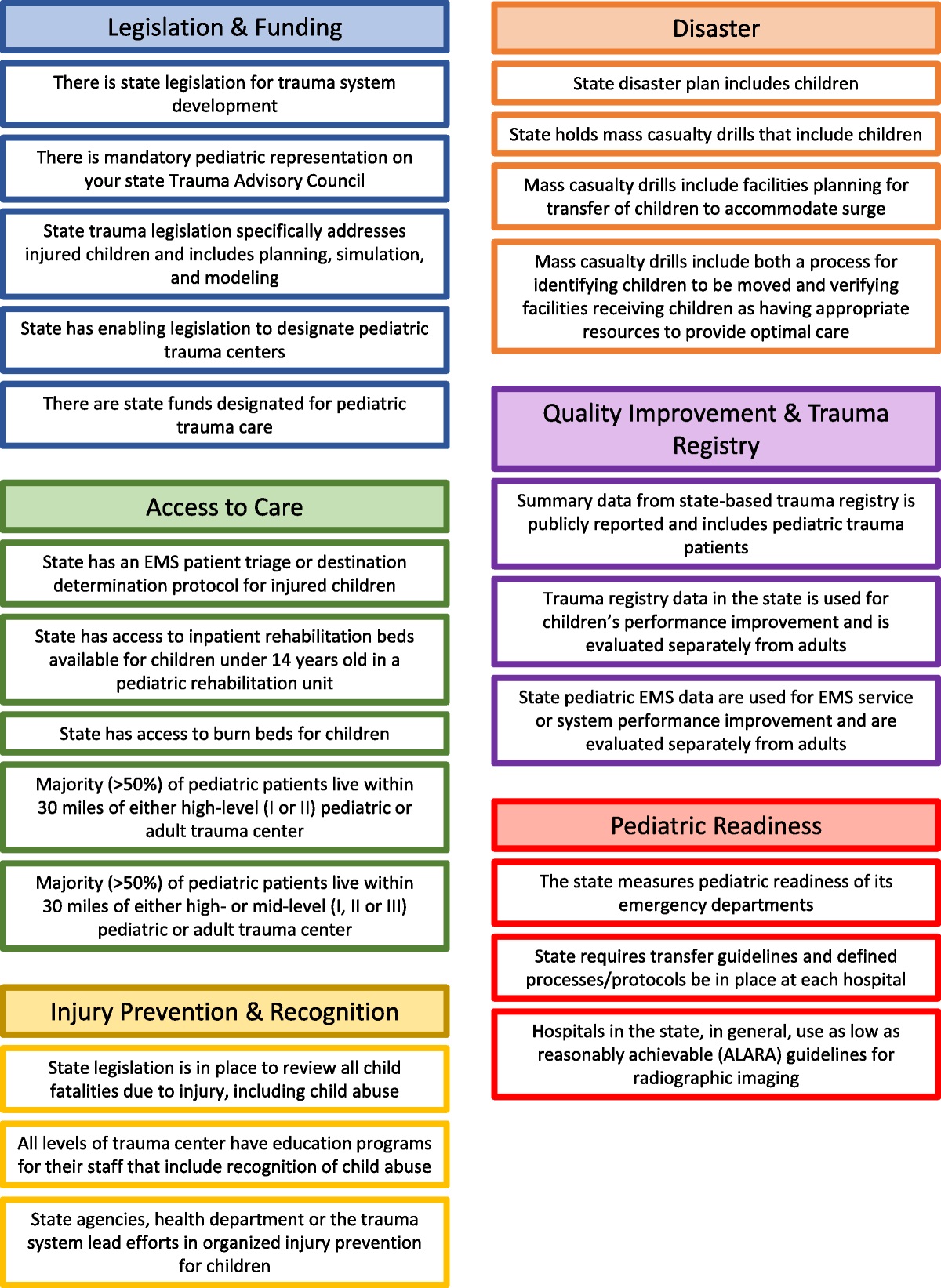
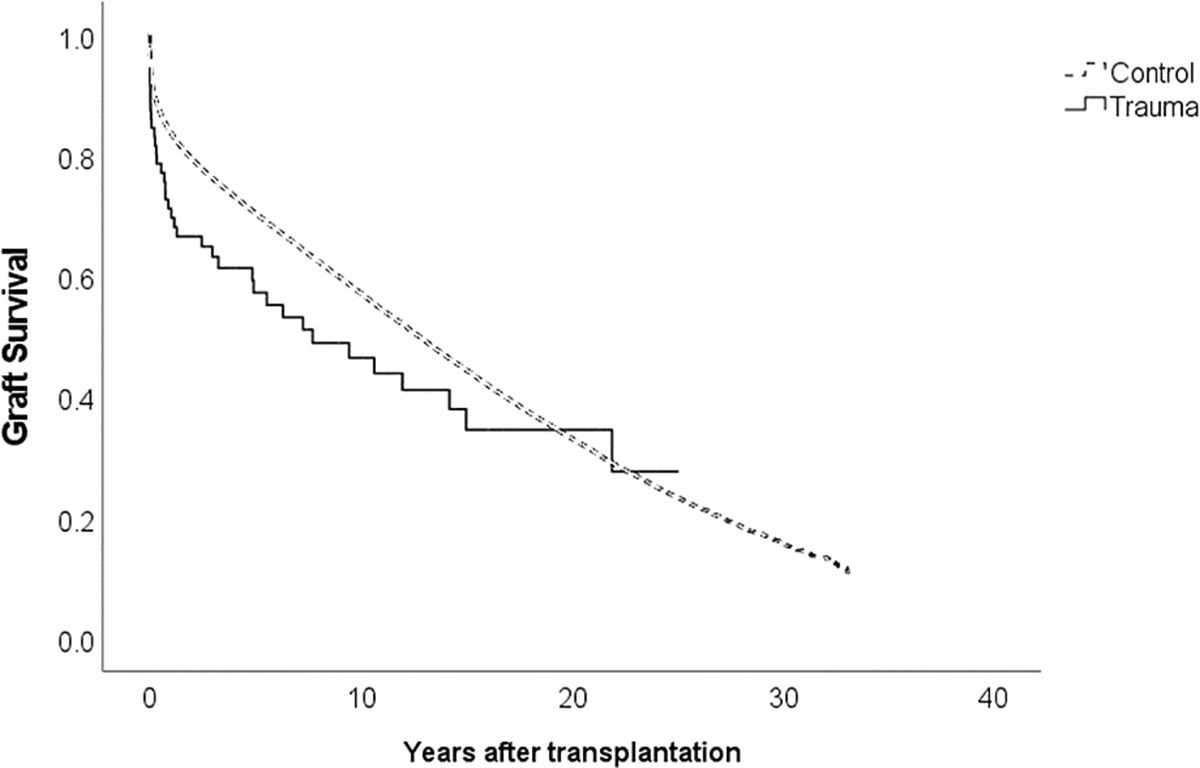
TABLE 2 - Later Biliary Recurrences and Time From Initial Admission to Recurrent Biliary Events Median Time (Min-Max) <30 Days <180 Days <365 Days <3 Years Any biliary event, d 307 (12–1993) 3 (0.7%) 17 (4.0%) 28 (7.3%) 51 (11%) Cholecystitis, d 307 (14–1799) 2 (0.5%) 12 (2.8%) 18 (4.7%) 32 (7.1%) Choledocholithiasis, d 314 (77–1993) — 5 (1.1%) 9 (2.3%) 17 (3.8%) Cholangitis, d 180 (12–1993) 2 (0.5%) 7 (1.6%) 9 (2.3%) 12 (2.7%) Pancreatitis, d 242 (208–515) — — 2 (0.5%) 2 (0.4%) Pain, d 307 — — 1 (0.3%) 2 (0.4%)Median time from ERC to second biliary event was 307 days (12–1993 days). Kaplan-Meir curve is shown in Figure 2. More than half of the events (n = 28/51, 55%) occurred during the first year after ERC.
 Figure 2:
Figure 2: Kaplan-Meier curve of cumulative later biliary events (number of events/months).
DISCUSSIONWhile laparoscopic cholecystectomy is often recommended after ERC to reduce risk of recurrent biliary events, relatively little is known about the safety of the wait-and-see strategy among older patients with choledocholithiasis. Here we have shown that patients with choledocholithiasis can be treated successfully and safely with ERC without later cholecystectomy with relatively low risk of later biliary events.
Endoscopic retrograde cholangiography is the current gold standard treatment for choledocholithiasis.2,3 Our results are in line with earlier studies on the excellent safety and efficacy of ERC in older patients.12–15 Currently, the main reason for subsequent cholecystectomy after ERC is the prevention of recurrent biliary events. Among the first studies to study whether prophylactic surgery after endoscopic stone extraction is required was performed by Boerma et al.16 This study reported a 47% risk of recurrent biliary symptoms among those undergoing a similar wait-and-see strategy. In the present study, symptoms were uncommon; only one patient suffered later from symptomatic disease and one in ten patients suffered from any subsequent biliary events. Compared with Boerma et al.10 our patients were older and had more often significant comorbidities. Similar findings that endorse subsequent cholecystectomy have been reported in other trials.8 However, at least these earlier studies have excluded patients 75 years or older.17 Furthermore, the frailest patients are often excluded from clinical trials. This might explain our better-than-expected results.
The reason why some suffer from later common bile duct stone-related problems is unknown—there are multiple possible reasons: all stones might have not been removed in the ERC, there is a risk of stricture after sphincterotomy, patients may develop new gallstones directly in the common bile duct, or small stones from the gallbladder may pass into the common bile duct. Nevertheless, choledocholithiasis can also occur after prophylactic surgery as well. Earlier studies have reported a 2.1% to 19% risk of recurrent choledocholithiasis after cholecystectomy.4,5 Here we have shown that one in ten patients suffer from later biliary events, but these can be often managed as safely and efficiently as during the initial hospital stay. Recurrent biliary events rarely lead to repeated operations or ERC or other clinically significant problems. Patients have often short history of symptoms illustrating that in overall the majority of patients with gallstones are asymptomatic. Earlier studies have estimated that gallstone disease may affect as many as 10% to 15% of the adult population, and up to 80% will never experience symptomatic or complicated disease.1 Finally, the authors of our study emphasize the economic impact of the area under study. Gallstone disease has a significant economic impact due to its prevalence, which increases with age, and as the older population increases even more efforts should thus be made to reduce the number of unnecessary operations. Further studies are planned to study the economic impact of different treatment strategies.
This study has some limitations. This was a retrospective study from two university hospitals. However, all emergency cases, ERCs and surgeries within the study hospital districts were performed in these hospitals. The data were compiled using a nationwide database search from the Finnish Care Register for Health Care to find patients moved to other regions or treated in other hospitals. Consequently, the data were comprehensive with long-term follow-up data available on all patients. No patients were lost from follow-up. However, nearly one sixth of study patients died within 1 year after ERC, thus raising suspicion of some patient selection bias. The decision whether patients underwent surgery was based on surgeons' decision and patients' own will. Previously healthy patients or those with no significant comorbidities may have been recommended to undergo surgery, and only those with significant comorbidities may have been selected for the wait-and-see strategy. These patients have high overall mortality, and in all cases, we may not be able to register later symptoms or factual cause of death. Nevertheless, our results support wait-and-see approach in selected patients, we are already planning to start multicenter randomized trial to verify our results. While here we were specifically interested in older frail patients, further prospective studies are required to find other subgroups (according to background factors, anesthesia risks, symptoms, presence of acute cholangitis or cholecystitis at index admission, medications or clinical frailty scores) who would benefit from wait-and-see-strategy.
CONCLUSIONAccording to our study a wait-and-see policy after ERC seems to be a safe option for older patients with choledocholithiasis. In the over 3-year follow-up, only less than one in ten patients suffered clinically relevant biliary morbidity after ERC when gallbladder is deliberately left in situ.
DISCLOSUREThe authors declare no funding or conflicts of interest.
All the authors contributed equally to study design, data interpretation, writing and critical revision of this article. Data were collected and analyzed by A.K., L.M., and M.U.
REFERENCES 1. Stinton LM, Myers RP, Shaffer EA. Epidemiology of gallstones. Gastroenterol Clin N Am. 2010;39(2):157–169, vii. 2. Buxbaum JL, Abbas Fehmi SM, Sultan S, Fishman DS, Qumseya BJ, et al; ASGE Standards of Practice Committee. ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis. Gastrointest Endosc. 2019;89(6):1075–1105.e15. 3. Manes G, Paspatis G, Aabakken L, Anderloni A, Arvanitakis M, Ah-Soune P, et al. Endoscopic management of common bile duct stones: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2019;51(5):472–491. 4. Yoo ES, Yoo BM, Kim JH, Hwang JC, Yang MJ, Lee KM, et al. Evaluation of risk factors for recurrent primary common bile duct stone in patients with cholecystectomy. Scand J Gastroenterol. 2018;53(4):466–470. 5. Ding G, Cai W, Qin M. Single-stage vs. Two-stage management for concomitant gallstones and common bile duct stones: a prospective randomized trial with long-term follow-up. J Gastrointest Surg. 2014;18(5):947–951. 6. Kamarajah SK, Karri S, Bundred JR, Evans RPT, Lin A, Kew T, et al. Perioperative outcomes after laparoscopic cholecystectomy in elderly patients: a systematic review and meta-analysis. Surg Endosc. 2020;34(11):4727–4740. 7. Loozen CS, van Ramshorst B, van Santvoort HC, Boerma D. Early cholecystectomy for acute cholecystitis in the elderly population: a systematic review and meta-analysis. Dig Surg. 2017;34:371–379. 8. McCarty TR, Farrelly J, Njei B, Jamidar P, Muniraj T. Role of prophylactic cholecystectomy after endoscopic sphincterotomy for biliary stone disease: a systematic review and meta-analysis. Ann Surg. 2021;273(4):667–675. 9. Fagenson AM, Powers BD, Zorbas KA, Karhadkar S, Karachristos A, Di Carlo A, et al. Frailty predicts morbidity and mortality after laparoscopic cholecystectomy for acute cholecystitis: an ACS-NSQIP cohort analysis. J Gastrointest Surg. 2021;25(4):932–940. 10. Cotton PB, Lehman G, Vennes J, Geenen JE, Russell RC, Meyers WC, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991;37:383–393. 11. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. 12. Tohda G, Ohtani M, Dochin M. Efficacy and safety of emergency endoscopic retrograde cholangiopancreatography for acute cholangitis in the elderly. World J Gastroenterol. 2016;22(37):8382–8388. 13. Galeazzi M, Mazzola P, Valcarcel B, Bellelli G, Dinelli M, Pasinetti GM, et al. Endoscopic retrograde cholangiopancreatography in the elderly: results of a retrospective study and a geriatricians’ point of view. BMC Gastroenterol. 2018;18(1):38. 14. Ukkonen M, Siiki A, Antila A, Tyrväinen T, Sand J, Laukkarinen J. Safety and efficacy of acute endoscopic retrograde cholangiopancreatography in the elderly. Dig Dis Sci. 2016;61(11):3302–3308. 15. Yun DY, Han J, Oh JS, Park KW, Shin IH, Kim HG. Is endoscopic retrograde cholangiopancreatography safe in patients 90 years of age and older?Gut Liver. 2014;8(5):552–556. 16. Boerma D, Rauws EA, Keulemans YC, Janssen IM, Bolwerk CJ, Timmer R, et al. Wait-and-see policy or laparoscopic cholecystectomy after endoscopic sphincterotomy for bile-duct stones: a randomised trial. Lancet. 2002;360:761–765. 17. da Costa DW, Bouwense SA, Schepers NJ, Besselink MG, van Santvoort HC, van Brunschot S, et al. Same-admission versus interval cholecystectomy for mild gallstone pancreatitis (PONCHO): a multicentre randomised controlled trial. Lancet. 2015;386(10000):1261–1268.
留言 (0)