
記住我

Significant blunt bowel and mesenteric injuries (sBBMIs) include full-thickness perforations, seromuscular tears, and mesenteric lacerations and require emergent treatment. Relatively rare, this type of injury has a reported incidence of 1% of all trauma admissions and 3% for patients admitted for abdominal trauma.1–3 This low incidence may result in a challenging decision-making process and any delay in establishing a diagnosis has a negative impact on survival. Nonrecognized sBBMI is the most frequent cause for delayed laparotomies (LTs) after blunt abdominal trauma.4,5 Even a relatively short deferral of 5 to 8 hours of an intervention may lead to an increased morbidity and mortality.6,7
Clinical findings such as abdominal tenderness or the “seat-belt sign,” white blood cell (WBC) count, or the presence of vertebral or pelvic fractures have been reported to be associated with small bowel injury, but in isolation, they lack sensitivity and specificity.8–15 Plain X-rays and abdominal ultrasound are of limited value in the assessment for mesenteric and bowel injury and are no longer recommended.8 Intravenously contrast-enhanced computed tomography (CT) is considered standard of care for investigation of hemodynamically stable patients suffering from blunt abdominal trauma,16 with excellent overall sensitivity and specificity for intra-abdominal injuries.17,18 However, false-negative CT rates of up to 13% have been reported for sBBMI,19,20 especially in the setting of multiple-injury patients with concurrent solid organ or bladder injuries.21,22 Hence, missing a diagnosis of sBBMI is still an issue, leading to delayed surgical treatment and to its negative impact on survival.4,23 This is particularly true when managing blunt abdominal trauma patients with a CT showing unspecific or no signs of blunt bowel and mesenteric injury (BBMI), especially in the presence of clinical findings or in obtunded patients with an unreliable physical examination.22 For these situations and given the potential consequences of delayed diagnosis, surgical exploration is recommended. Because of its morbidity rates of 8% to 41%, nontherapeutic exploratory LT should be avoided.24–27 Diagnostic laparoscopy (LS) is a less invasive alternative with fewer associated complications.28
To optimize decision making and select patients for early surgical exploration, several tools predictive for sBBMI have been developed and published.14,29–31 These scores are based on either clinical, laboratory, or radiological variables, or a combination thereof, to predict the presence or absence of sBBMI. Because of its complex grading system for abdominal tenderness, the performance of the Z score by Zarour et al.30 could not be reliably evaluated using a retrospective study design. Moreover, it is not applicable on patients with a solid organ injury (SOI). The three scores retained for performance comparison are the Bowel Injury Prediction Score (BIPS),14 the score developed by Raharimanantsoa et al.,31 and the score by Faget et al.29 The latter two scores not having a proper term such as the BIPS, the authors of the present study have named them according to the first authors of the publication describing them: the Raharimanantsoa Score (RS) and the Faget Score (FS). The FS is built exclusively on a combination of CT findings and is easy to assess with a retrospective study design. Depending on the cutoff used, its originally reported sensitivity and specificity are, respectively, 91.1% to 100% and 85.7% to 97.6%, with a positive predictive value (PPV) of 41.4% to 82% and an negative predictive value (NPV) of 98.9% to 100%.29 Depending on the cutoff used, the reported sensitivities and specificities of the BIPS and RS are 85.7% and 76.2%, and 96% and 86.4% respectively, with respective PPVs of 70.6% and 48%, and NPVs of 88.9% and 99.4%.14,29,31 Like the FS, the BIPS and the RS are suitable for a retrospective analysis and applicable on patients with SOI.14,17,29,31 When applied to a series of patients with surgically proven sBBMI, only 56.3% had a “positive” BIPS (≥2 points—BBMI requiring surgery as defined by McNutt et al.14).32 A recent prospective multicenter study validated the BIPS as a predictor of sBBMI.33
The aim of the present study was to determine the incidence of delayed diagnosis and treatment of sBBMI in patients undergoing CT after a road traffic crash (RTC) and to evaluate the predictive performance of the FS, the BIPS, and the RS.14,29,31
PATIENTS AND METHODS Study DesignA single-center, registry-based retrospective cohort study, prepared to conform to the STrengthening the Reporting of OBservational studies in Epidemiology guidelines, was conducted.34 The study protocol was approved by the local institutional review board (2016-00928).
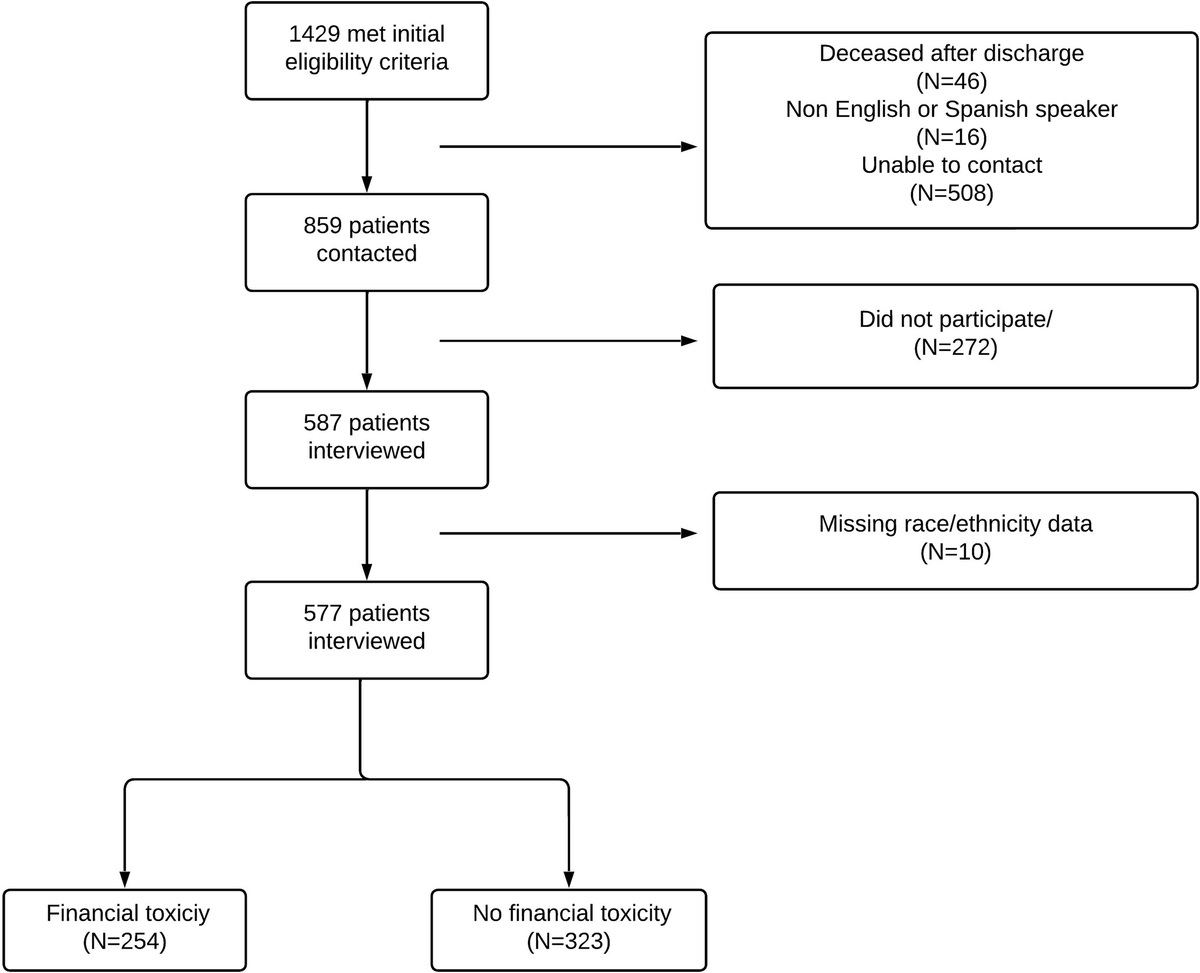
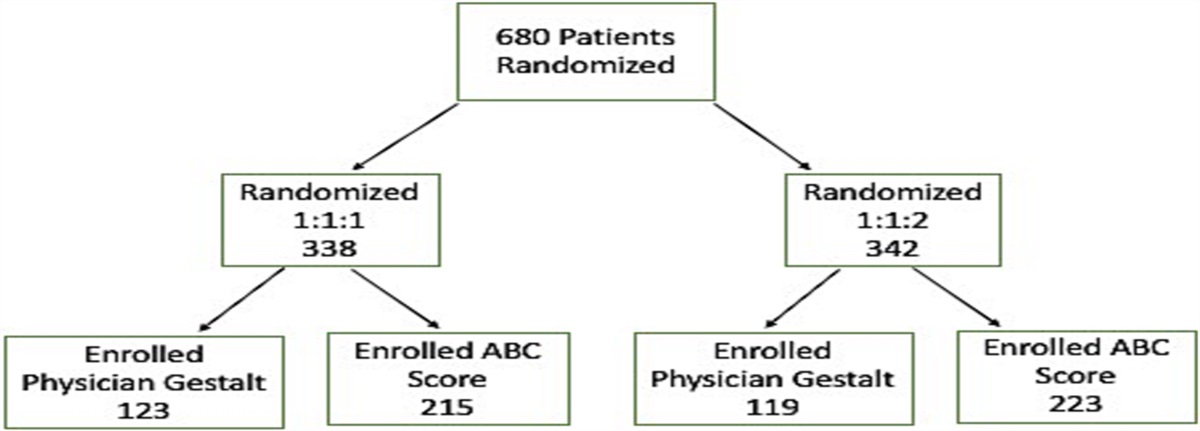
Study Setting and ParticipantsThis study was based on the prospective trauma registry of Lausanne University Hospital, a level I trauma center, including all consecutive patients older than 16 years admitted to the trauma resuscitation area of the emergency department (ED) following an RTC from January 2008 to December 2019. Patients with an initial observation period of less than 24 hours or without consecutive follow-up and patients with unavailable information about the presence or absence of sBBMI were excluded. For comparison of the scores, patients lacking items for score calculation were also excluded (Fig. 1).
 Figure 1:
Figure 1: Flowchart of RTC victims from January 2008 to December 2019.
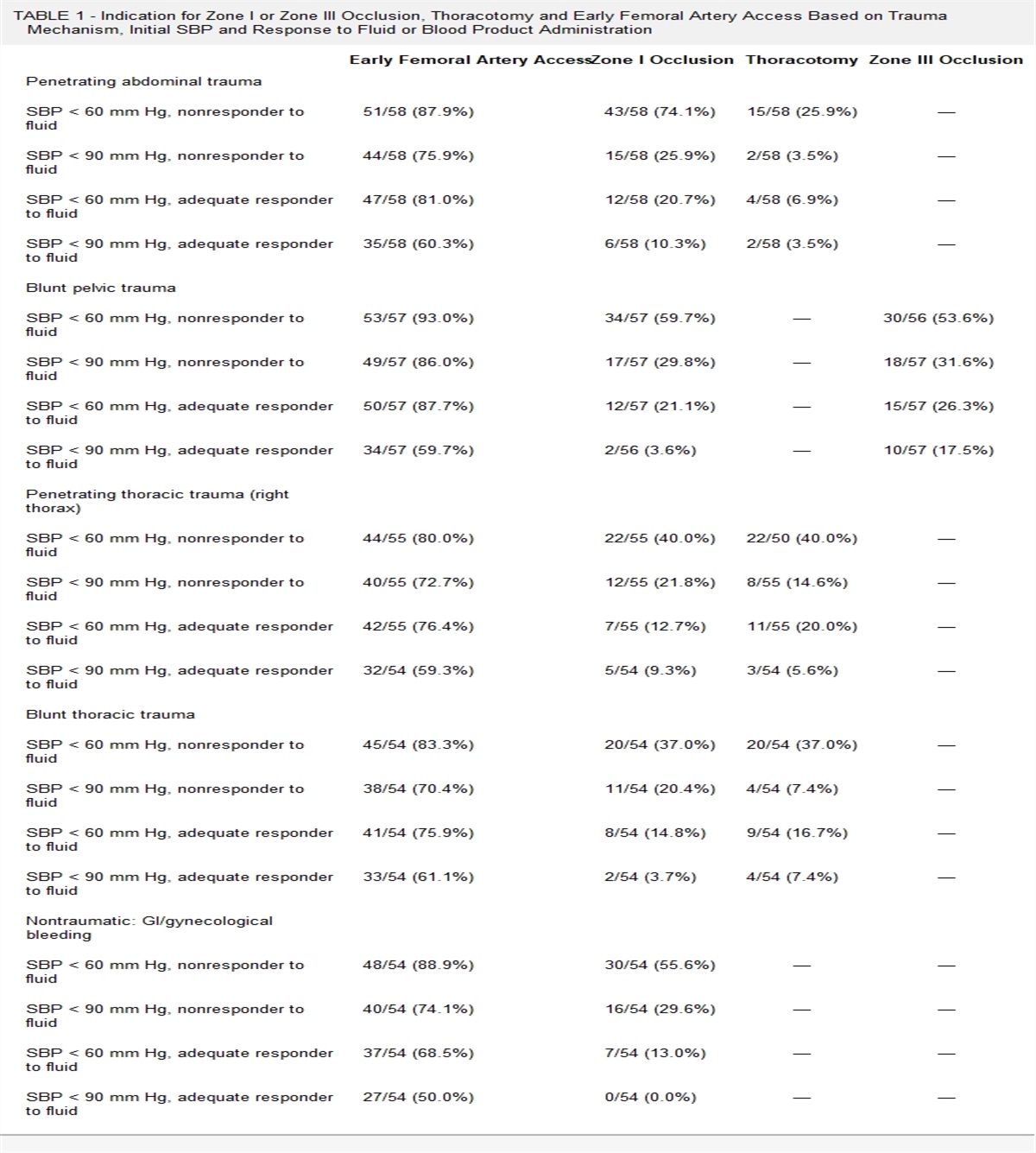
VariablesData included all items necessary to obtain each of the three tested scores (Table 1). Of note, the CT grading scale for mesenteric injury was purposefully created by McNutt et al.14 for its proposed BIPS. For the calculation of the FS (range, −1 to 24), 1 point was deducted in case of a concurrent splenic injury.
TABLE 1 - Score Points per Item for the Three Scores BIPS (Range, 0–3; Cutoff, ≥2 Pts) Pts RS (Range, 0–14; Cutoff ≥8 Pts) Pts FS (Range, −1 to 24; Cutoff ≥5 Pts) Pts WBC count ≥17 G/L 1 Free abdominal fluid 3 Hemoperitoneum ≤200 mL 1 Abdominal tenderness 1 Admission lactate level ≥1.82 mmol/L 2 Hemoperitoneum >200 mL 3 Mesenteric injury grade ≥4 1 Long bone fracture 1 Mesenteric pneumoperitoneum 5 Mesenteric Injury Grade Abdominal tenderness 2 Bowell wall thickening 2 1. Isolated mesenteric contusion* without associated bowel wall thickening or adjacent interloop fluid collection5
2
−1
Demographic data, mortality, Injury Severity Score (ISS), abdominal and extremity Abbreviated Injury Scale, diagnosis of sBBMI, and types of therapeutic intervention were obtained. The delayed treatment definition used in the present study is based on the consensus that operations performed >24 hours after admission for trauma constitute a serious delay.4 Blunt bowel and mesenteric injuries requiring either surgical or radiological treatment or obvious BBMI documented at autopsy were considered as significant. Patients who had none of the aforementioned injuries but who were alive at discharge after an observation period of more than 24 hours were considered not to have sBBMI.
Data SourceData were extracted from our prospective trauma registry and, when unavailable (abdominal pain, CT-based variables, impact against a vehicle in motion), were collected from the electronic patient records. The results of forensic autopsies were obtained with the permission of the Attorney General. All available clinical data, laboratory, and imaging results were obtained and recorded during the initial phase of care in the ED. When abdominal tenderness was not evaluable (intubated patients), 0 points were scored for this item. These patients were included in our analysis because the nonavailability of this information reflects reality and is not a limitation of the retrospective nature of the study.
The institutional multiple-injury CT protocol was performed with a 64-detector row multidetector CT system from January 2008 to August 2015 (Light Speed VCT 64 Pro; GE Healthcare, Milwaukee, WI) and a 256-row MDCT system (Revolution CT; GE Healthcare) from September 2015 to December 2019. With both machines, 1.25-mm reconstructed axial slices were acquired with increments of 1 mm during the arterial phase (25 seconds) centered on the thorax, and 2.5-mm reconstructed axial slices, with increments of 2 mm during the venous phase (80 seconds) centered on the abdomen and pelvis, after intravenous injection of iodinated contrast medium Accupaque (GE Healthcare, Milwaukee, WI) at a flow rate of 4 mL/s (120 kV; 300 mA; table speed, 55 mm per rotation [0.8 seconds]; pitch, 1.375). Automatic tube current modulation in all three axes (SmartmA) was used as well as adaptive statistical iterative reconstruction algorithm. All CT images were reviewed by one of the authors with >20 years of expertise in abdominal imaging for the presence or absence of free abdominal fluid, grade of bowel and mesenteric injury, and CT findings according to McNutt et al.14 and Faget et al.29
Statistical MethodsStatistical and graphic analyses were performed using R software version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria).35 For qualitative variables, results are expressed in frequencies and percentages. For continuous variables, a measure of dispersion was given using median, with interquartile ranges (IQRs) or with IQR (IQR = Q3–Q1). Qualitative variables were compared using Fisher's exact or χ2 test. Continuous variables were compared using Student's t test when distribution was bell shaped, and they were compared using a Kruskal-Wallis test if distribution was skewed. A significance threshold with a p value of 0.05 was adopted for all statistical analyses. Variables included in the multivariate analysis were selected based on their p value (<0.001) after univariate analysis. The variable “CT mesenteric injury grade ≥4” (BIPS) was included as a surrogate for all significant individual radiological variables to avoid overfitting. The predictive accuracy of the risk scores was compared with receiver operating characteristic (ROC) curve analysis.36,37 The areas under the ROC curve was calculated with 95% confidence interval (CI) and statistical comparisons used the DeLong method.38
RESULTS ParticipantsFrom January 2008 to December 2019, 1,258 patients were admitted to the trauma resuscitation area of our institution ED following an RTC. Patients who underwent abdominal CT without radiological evidence of injury and were discharged home or transferred to another care facility after an observation period available of less than 24 hours (n = 64) were excluded from analysis. Among all patients with a follow-up period of ≥24 hours, 18 were excluded since they died without any abdominal intervention or autopsy and therefore having an unknown sBBMI status. Finally, 12 patients were excluded because of their incomplete data sets for the calculation of any of the scores (Fig. 1). The performance comparison of the FS, the BIPS, and the RS was carried out using a common dataset where all items were available for the calculation of the three scores. In total, 247 patients were excluded because of one or more missing items for the calculation of one or more scores, resulting in a population of 917 patients on whom all 3 scores could be tested.
Descriptive Data and OutcomeThe prevalence of sBBMI in the group of patients with known sBBMI status was 3.3% (38 of 1,164). Overall (n = 1,164), 48 patients (4%) died before any intervention, and their sBBMI status was revealed by forensic autopsy findings. Significant blunt bowel and mesenteric injury was found in one of these patients. Table 2 shows the characteristics of the study population with and without sBBMI. Table 3 summarizes the characteristics of the three subtypes of sBBMI (isolated bowel/combined bowel and mesenteric/isolated mesenteric).
TABLE 2 - Characteristics of the Study Population With (+) and Without (−) sBBMI (n = 1,164) Patient Characteristics and Score Items sBBMI + n = 38 (3.3%) sBBMI − n = 1,126 (96.7%) p Age Median (IQR), y 37 (24–56) 38 (24–54) 0.97 Sex, n (%) 0.25 Male 25 (65.8) 834 (74.1) Female 13 (34.2) 292 (25.9) ISS Median (IQR), score 25 (17–34) 14 (9–24) <0.001 LOS Median (IQR), d 18 (9–39) 9 (3–19) <0.001 Mortality 30 d, n (%) 5 (13.2) 71 (6.3) 0.10 Admission to death, median (IQR), d 1.5 (0.7–8.2) 0.4 (0.1–3.4) 0.42 WBC count ≥17 G/L, n (%) 14 (36.8) 340 (30.2) 0.47 NA, n (%) 0 38 (3.4) Lactate ≥1.8 mmol/L, n (%) 26 (68.4) 612 (54.4) 0.30 NA, n (%) 0 107 (9.5) Type of collision, n (%) Collision with a moving object 22 (57.9) 521 (46.3) 0.14 NA 2 (5.3) 51 (4.5) Abdominal tenderness, n (%) Abdominal tenderness 26 (68.4) 194 (17.2) <0.001 NA (intubated) 8 (21.1) 209 (18.6) NA 0 12 (1.1) Free abdominal fluid on CT, n (%) Free abdominal fluid 28 (73.7) 178 (15.8) <0.001 NA 3 (7.9) 60 (5.3) Long bone fracture, n (%) Long bone fracture 13 (34.2) 409 (36.3) 0.79 NA 0 1 (0.1) Patient's vehicle type, n (%) Car 26 (68.4) 462 (41.0) <0.001 Motorbike 8 (21.1) 356 (31.6) 0.17 NA 0 0 CT findings, n (%) Hemoperitoneum ≤200 mL 15 (39.5) 84 (7.5) <0.001 Hemoperitoneum >200 mL 10 (26.3) 67 (6.0) <0.001 Mesenteric pneumoperitoneum 7 (18.4) 1 (0.1) <0.001 Bowel wall thickening 22 (57.9) 163 (14.5) <0.001 Arterial mesenteric vessel extravasation 11 (28.9) 3 (0.3) <0.001 Mesenteric stranding 29 (76.3) 151 (13.4) <0.001 Reduced bowel wall enhancement 4 (10.5) 3 (0.3) <0.001 Bowel wall discontinuity 2 (5.3) 0 <0.001 Splenic injury 7 (18.4) 50 (4.4) <0.001 Anterior abdominal wall injury 6 (15.8) 79 (7.0) 0.03 CT mesenteric injury grade ≥4 (BIPS) 25 (65.8) 56 (5.0) <0.001 NA 7 (18.4) 74 (6.6)Median length of stay (18 days vs. 9 days, p < 0.001), Injury Severity Score (25 vs. 14, p < 0.001), abdominal tenderness (68.5% vs. 17.2%, p < 0.001), and free abdominal fluid on CT scan (73.7% vs. 15.8%, p < 0.001) were significantly higher in patients with sBBMI. Thirty-day mortality (13.2% vs. 6.3%, p = 0.10) was not significantly higher in patients with sBBMI. Among the variables used for score calculation, presence of free abdominal fluid (p < 0.001), BIPS CT grade ≥4 (p < 0.001), traveling in a car (p = 0.001), and abdominal tenderness (p < 0.001) were all significantly associated with sBBMI in univariate analysis, whereas WBC counts ≥17 (p = 0.47), lactate levels ≥1.82 mmol/L (p = 0.30), collision with a moving vehicle (p = 0.14), presence of a long bone fracture (p = 0.79), and traveling on a motorcycle (p = 0.17) were not significantly associated with sBBMI. Results of the multivariate analysis using the statistically significant variables after univariate analysis used for the three score calculations are presented in Figure 2. Mesenteric injury grade ≥4 of the BIPS was used as a surrogate for all significant items of the FS after univariate analysis. The score item “Patient was in a car” of the RS was no longer significant after multivariate analysis.
 Figure 2:
Figure 2: Multivariate analysis of the score items significantly associated with sBBMI in univariate analysis. Variables included in the multivariate analysis were selected based on their p value (p < 0.001) from the univariate analysis. The item of CT mesenteric injury grade ≥4 (BIPS) was used to represent all individual significant CT variables.
Patient ManagementOf the 38 patients with sBBMI, 33 (86.8%) required surgical treatment and 4 (10.5%) underwent angioembolization (AE). One patient died before any treatment, and sBBMI was found at autopsy.
The most frequent sBBMIs found at exploration were active bleeding from a mesenteric vessel (n = 24) and bowel perforation (n = 26), either isolated or in association. Laparotomy was performed in 28 patients with sBBMI, of which 8 were conversions from LS. Five patients were successfully managed with LS alone. For the 33 patients with sBBMI undergoing surgical exploration of the abdomen, the median interval from ED arrival to operation was 143 minutes (IQR, 90–880 minutes). Seven patients (18%) with sBBMI underwent surgical exploration more than 24 hours after ED arrival, with a median time interval to operation of 56 hours (IQR, 33.4–100.8). Two directly underwent an LT, and five a diagnostic LS, of which four were converted to LT.
For the four patients undergoing successful AE for active mesenterical bleeding on CT, the median interval from ED arrival to embolization was 122 minutes (IQR, 105–138 minutes). One patient underwent a left colectomy for bowel necrosis 4 days after AE of the inferior mesenteric artery. Mortality was similar for patients with sBBMI who underwent early treatment (13.3%) compared with patients with delayed intervention (14.3%).
Performance of CTFor evaluation of CT performance, 81 patients were excluded from the initial population of 1,164 patients. These underwent no abdominal CT for either hemodynamic instability or absence of a clinical indication. Blunt bowel and mesenteric injury was found in 7 unstable patients without prior CT, leaving 31 patients with sBBMI in the subpopulation who underwent CT (n = 1,083).
Overall, 176 patients (16.3%) had free abdominal fluid. Among patients with sBBMI, 28 of 31 (90.3%) had free abdominal fluid on CT, in 19 cases as an isolated finding and in 9 cases with concomitant SOI (7 splenic and 2 liver injuries).
Specific CT Signs for sBBMIOf the 31 patients with sBBMI undergoing CT, 16 (51.6%) presented CT signs specific for sBBMIs, either active mesenteric bleeding (n = 9), pneumoperitoneum (n = 5), or both (n = 2). Of these 16 patients with specific sBBMI signs on CT, 15 underwent immediate treatment (surgery in 12, AE in 3). One patient had a delayed surgical treatment (27.6 hours) because of missed free air in the CT and finally required a segmental resection of perforated small bowel. None of the patients with specific signs for sBBMI died.
Unspecific CT Signs for sBBMIOf all 31 patients with sBBMI undergoing CT, 15 (48.4%) had no specific signs of significant bowel or mesenteric injury. Of these 15 patients (1 without any sign, 8 with a mesenteric contusion, 1 with free fluid without SOI, and 5 with both mesenteric contusion and free fluid), 1 died before any abdominal intervention 35 hours after his arrival because of severe traumatic brain injury, and 6 (40%) had a delay in diagnosis and treatment of more than 24 hours (Table 4). In five of six cases, LS or LT was motivated by developing peritoneal signs. Among these five patients, three underwent a second CT before surgery, which confirmed an sBBMI in two cases. In one case, specific signs of sBBMI were discovered during a CT of the pelvis obtained to assess a previous internal pelvic fixation. Diagnostic and surgical treatment delays of more than 24 hours were significantly more frequent in patients without specific sBBMI signs on CT (6 of 15) compared with patients with specific signs (1 of 16) (p = 0.04).
TABLE 4 - Patients Without Specific CT Signs and Delayed sBBMI Diagnosis and Treatment (n = 6) Patients (n = 6) Delay (h) 2nd CT Abdominal Intervention sBBMI Detailed Intervention
留言 (0)