
記住我

Most research on long-term COVID has been carried out for small cohorts with a short follow-up period. In one of the few publications published in the most authoritative journal Lancet, L. Huang et al. [30] report the largest 12-month longitudinal cohort study to date involving adult post-COVID-19 patients (mean age of 59 years) discharged from Jin Yin-tang Hospital in Wuhan, China. The study confirms that COVID-19 survivors still had great mobility problems one year later, complained of pain or discomfort, and also felt anxiety or depression, in contrast to the control group (comparable adults living in communities without SARS-CoV-2 infection). Fatigue or muscle weakness was the most common symptom at both 6 and 12 months. Almost half of the patients reported that they had at least one symptom after 12 months. The most common complaints were sleeping difficulty, either heart palpitations, or joint pain or chest pain. The study showed that for many patients, full recovery from COVID-19 can extend to more than 1 year. This work raises important questions for both medical services and future research [29].
The second important aspect that was announced in the editorial of the journal is the vocational rehabilitation programs for patients with long-term COVID. Only 0.4% of patients with long-term COVID-19 reportedly stated that they had participated in a vocational rehabilitation program. The reason for this low utilization of rehabilitation services is not clear. One reason may be a lack of understanding or recognition of the “long COVID” syndrome and clear management of these patients. And this is a real and widespread problem all over the world. Second, the impact of long-term COVID on mental health requires further study and long-term research [65].
The symptoms of “prolonged covid” include fatigue, cough, shortness of breath, loss of taste and smell, muscle weakness, muscle and joint pain, headache, confusion, conjunctivitis, chest pain, decreased mobility, and falls [36, 45].
Patients after a severe form of COVID-19 who have been hospitalized, as well as those observed on an outpatient basis with mild clinical forms of the disease, often report fatigue, shortness of breath, pain of various intensity and localization, cough, and other respiratory and extrapulmonary symptoms that persist for weeks and months. After discharge, less than 13% of patients feel healthy, while the majority continue to experience up to three or more symptoms of the disease, which usually do not include only fever [1]. In an Italian study assessing the persistence of COVID-19 symptoms in 143 patients discharged from hospital, only 18 (12.6%) were completely free of any symptoms associated with COVID-19 on average 60 days after the onset of the first symptoms [10]. The number of people ≥50 years old with long-term health problems increased to 47%. In addition, regardless of age, it has been found that the greater the number of pre-existing chronic conditions, the more likely it is that the resolution of symptoms will be delayed [60].
How long the disease lasts after “recovery,” including long-term physical and psychological health consequences, as well as the future of survivors of COVID-19, remains largely unclear [53].
TERMINOLOGY OF THE POST-COVID-19 PATHOLOGICAL CONDITIONThe 2019 coronavirus disease (COVID-19) pandemic has led to an increase in the population of people with a wide range of persistent symptoms after acute SARS-CoV-2 infection [59]. Because this coronavirus is a new virus, there is very little information available about the long-term effects of the disease it causes. There is not even a real consensus on what to call the long-term condition associated with COVID-19.
Several terms have been used to describe persistent symptoms after COVID-19 illness, such as “post-COVID conditions,” “long-COVID,” “post-acute consequences of SARS-CoV-2 (PASC) infection,” “post-acute COVID-19,” “chronic COVID-19” and “post-COVID syndrome.”
The term “long COVID” has been introduced by patients and has taken hold in traditional media and social media. Elisa Perego from Lombardy was the first to use the term LongCovid on Twitter to describe her long-term illness, summarizing her own symptoms. In June, the term moved from social media to print describing how Dr. Jake Suett joined a patient support group [8].
The National Institute for Health and Care Excellence (NICE) in agreement with the Scottish Intercollegiate Guidelines Network and The Royal College of General Practitioners in their recommendations from 30 October 2020 first described the following forms of COVID-19:
(1) acute COVID-19—complaints and symptoms of COVID-19 lasting up to 4 weeks;
(2) ongoing symptomatic COVID-19—complaints and symptoms of COVID-19 lasting 4–12 weeks;
(3) post-COVID-19 syndrome—complaints and symptoms that develop during or after COVID-19, last >12 weeks and are not the result of another diagnosis [13].
T. Greenhalgh et al. proposed the following division [22]:
(1) extended COVID-19—for cases where symptoms persist >3–4 weeks from the moment of infection manifestation;
(2) chronic COVID-19—if symptoms persist >12 weeks after the onset of the first symptoms.
At the end of February 2021, to separate the concepts of “long-term COVID-19” and “post-covid syndrome,” E. Fauci (United States) proposed the use of a new acronym instead of “long COVID-19”—PASC (post-acute sequelae of SARS-CoV-2 infection/COVID-19) [17].
While the WHO reports that 80% of COVID cases are “mild or asymptomatic” and most patients recover in 1–2 weeks, thousands of people now say they manage severe symptoms in 1–3 months or longer. In online support groups, these people call themselves “long-haulers.” There is still no verbatim analogue of this word in Russian-language scientific publications. However, the term “long-haulers” refers to a patient with long-term symptoms of coronavirus infection, or a patient with a long course of the disease, or patients with a long recovery from COVID-19. The term “long-haulers” has now migrated to scientific medical publications. Post-COVID syndrome, or long-covid, has already been included in the ICD-10 with the wording “Post COVID-19 condition,” and scientists from around the world are still collecting data on its manifestations and duration. At the initiative of Russian therapists, a separate code appeared in the ICD-10 to describe the post-COVID syndrome—U09.9 post COVID-19 condition.
The WHO indicates that recovery from a mild course of COVID-19 takes about 2 weeks, while a severe one can be prolonged up to 3–6 weeks. However, since COVID-19 is a new, little-studied infectious disease, it is not possible to reliably speak about the long-term consequences of the disease, i.e., more than 6 months or more. It is also not clear whether the persisting pattern of symptoms after an illness represents a new syndrome unique to COVID-19, or whether there is an overlap with recovery from similar illnesses.
LONG-TERM CONSEQUENCES FOR DIFFERENT VARIANTS OF COVID-19The long-term consequences for different strains of COVID-19 are still unknown [12]. Since the beginning of the pandemic, several variants of COVID-19 have emerged that are more transmissible and can lead to more severe acute illness. In the UK, one of the first strains of concern to emerge was the so-called “Kent variant” from lineage B.1.1.7, now called the Alpha variant. This variant is approximately 50% more transmissible [14] and likely increases the severity of acute disease [62]. As of June 30, 2021, the Alpha variant had been confirmed in over 275 000 cases in the UK and had spread to at least 136 countries worldwide [64].
In the UK, in addition to the Alpha strain, studies are underway on other identified strains of COVID-19 [65]. The US Centers for Disease Control and Prevention (CDC) and the UK government website [28] report the emergence of strains of scientific interest in both the US and the UK (Table 1).
Table 1. Variants of concern or under investigation (data up to November 24, 2021)New strains of COVID-19 such as the Eta and Delta variants will continue to emerge and spread as the pandemic evolves, with over 161 000 cases of the rapidly spreading Delta strain confirmed in the UK as of June 30, 2021. Lambda and Omicron have recently emerged which will require close monitoring. The ability of these viral strains to cause long-term complications needs to be fully explored. It can be assumed that one variant causes more devastating long-term consequences than the others, and therefore patients infected with that variant who subsequently develop long-term COVID symptoms may need additional support, as well as faster and more intensive treatment strategies to combat long-term symptoms.
According to H. Crook et al. [12], at present, the understanding of what “long-term COVID” is remains a mystery, and since the question of the impact of new variants of COVID-19 on the frequency and severity of long-term COVID is still open, it is important that research continues. It is necessary to understand what the syndrome is after suffering COVID-19. A deeper understanding of the pathogenesis, risk factors, symptoms, and treatments for long-term COVID is primarily required to reduce the burden on the healthcare system [12].
LONG-TERM CONSEQUENCES: ARE THERE ANY CORRELATIONS OF COVID-19 WITH PREVIOUS CORONAVIRUSES?Some authors, in search of answers to questions about the possible long-term effects of COVID, have turned to previous similar coronaviruses (i.e., SARS-CoV-1 and Middle-East Respiratory Syndrome Coronavirus [MERS-CoV]), in combination with the known health effects of SARS-CoV-2 infection on the prediction of potential long-term consequences of COVID-19, including pulmonary, cardiovascular, hematopoietic, renal, central nervous system (CNS), gastrointestinal, and psychosocial manifestations, in addition to well-known post-intensive care syndrome [27, 57].
Also well known is the concept of a viral disease that leads to the development of a post-viral syndrome, usually accompanied by chronic fatigue [26]. Thus, in a study in which patients were observed after one of three viral diseases [Epstein-Barr virus, Burnet’s coxiella (the causative agent of Q fever), or Ross River fever virus], 12% were found to have a specific syndrome for 6 months or more. Acute relapses of the disease were observed in the first 3 months, and chronic fluctuating symptoms included fatigue, cognitive impairment, dysphoria, anxiety, and muscle pain. This syndrome has also been called myalgic encephalomyelitis [61].
In analyzing the epidemiological data of the SARS pandemic 2002–2004, myalgia, muscle dysfunction, osteoporosis and osteonecrosis were identified as frequent consequences in patients with moderate and severe forms of this disease. Early studies have shown that some patients with COVID-19 also have significant musculoskeletal dysfunction, although long-term follow-up studies have not yet been conducted [15].
In this respect, the question remains: do the lessons of SARS apply to COVID-19? Other concerns arise: does acute COVID-19 cause diabetes [27]? Or other metabolic disorders? Will patients develop interstitial lung disease? The careful recording of symptoms and examination of the patient should allow an understanding as to how much of the consequences are common to all severe infections, which symptoms can be explained by anxiety caused by the new disease and isolation, and which symptoms are secondary to the complicated disease. If COVID-19 does cause long-term effects, then are the mechanisms underlying long-term effects immune mechanisms? Or are they caused by new or recurrent inflammation, ongoing infection, or side effects of immunomodulatory treatments? Such data may indicate candidate management strategies that will be tested during trials [66].
In general, survivors of viral pneumonia are at risk of psychological and physical complications of the disease itself, as well as treatment-related damage to the lungs and other organs. Although most survivors can return to work and normal life, a significant number of them will be found to have impaired breathing and diffusion of gases in the blood [53]. After recovery, patients remain at risk for lung disease, heart disease, weakness, and mental disorders. There may also be long-term effects of adverse events that develop during COVID-19 and its treatment [32].
SYMPTOMS OF POST-COVID SYNDROMECOVID-19 can affect virtually any organ in the body as it enters cells through angiotensin-converting enzyme (ACE) 2 receptors [5]. The possible lesions of various organs and systems of the body and associated complaints of patients are shown in Fig. 1.
Fig. 1.
Multi-organ complications of COVID-19 and long-term COVID via angiotensin-converting enzyme 2 (ACE2) receptors [12] (PTSD ia post-traumatic stress disorder).
It was shown in a retrospective cohort study by M. Taquet et al. [58] that the incidence of “any” signs or symptoms of long-term COVID varied from 46.42% in the age group 10–21 years to 61.05% over the age of 65 years, with 63.64% of patients initially hospitalized, and 73.22% of those hospitalized were placed in the intensive-care unit. In the post-COVID period, women were significantly more likely to suffer from headache, abdominal symptoms, and anxiety/depression, while men were significantly more likely to experience breathing difficulties and cognitive symptoms. A list of the main symptoms and their increasing relationships 1–180 days after the diagnosis of COVID-19 is presented in Fig. 2 [58].
Fig. 2.
Frequency, relationships, and evolution of long-term COVID symptoms: a 6-month retrospective cohort study of 273 618 COVID-19 survivors [58].
According to C. Huang et al., the most common symptoms after acute COVID-19 are fatigue and shortness of breath. The work of these authors showed that 6 months after acute infection, COVID-19 survivors mostly suffered from fatigue or muscle weakness, as well as sleep problems, anxiety, or depression. Patients who were severely ill during their hospital stay had more severe impairments in lung diffusion capacity and abnormal chest-imaging findings. These patients are the main target population for long-term recovery [29]. Other common symptoms include joint pain and chest pain [10]. In addition to these general symptoms, dysfunction of specific organs has been reported, primarily the heart, lungs, kidneys, and brain [48].
CARDIOVASCULAR SYSTEMMyocardial injury, defined by elevated troponin levels, has been described in patients with severe acute COVID-19, along with thromboembolic disease. Myocardial inflammation and myocarditis, as well as cardiac arrhythmias, have been described following SARS-CoV-2 infection. In a German study of 100 patients recently recovered from COVID-19, cardiac MRI (performed on average 71 days after COVID-19 diagnosis) revealed cardiac involvement in 78% and ongoing myocardial inflammation in 60% [50].
The presence of chronic comorbidities, duration and severity of acute COVID-19 illness, and time since initial diagnosis did not correlate with these data. However, the sample was not random and probably biased towards patients with heart disease. However, of 26 competitive college athletes who were diagnosed with COVID-19, none of whom required hospitalization and most reported no symptoms, 12 (46%) had evidence of myocarditis or prior cardiac injury. The increased incidence of heart failure as a major consequence of COVID-19 raises concerns about significant potential consequences for the elderly population with multimorbidity, as well as for younger, previously healthy patients, including athletes.
LUNGSThe long-term impact of COVID-19 on parenchyma and lung function remains unresolved. Although it is still too early to give a definitive answer to this question, limited observations demonstrate significant lung effects of the disease in some survivors.
In a study of 55 patients with COVID-19 3 months after discharge, 35 (64%) had persistent symptoms and 39 (71%) had radiological abnormalities consistent with pulmonary dysfunction, such as thickening of the interstitial tissue and signs of fibrosis [67]. 3 months after discharge, the ability to diffuse carbon monoxide decreased in 25% of patients. In another study in 57 patients, lung function test results obtained 30 days after discharge, including decreased carbon-monoxide diffusivity and decreased respiratory-muscle strength, were normal and occurred in 30 (53%) and 28 (49%), respectively. [28]. If comorbid cardiovascular disease, either pre-existing or as a result of COVID-19, is exacerbated, a persistent decline in lung function can have serious adverse effects on the cardiopulmonary system.
It is important to understand that patients with severe COVID-19 pneumonia may take 6 months or more to return to normal breathing and that this is associated with decreased mobility. An elevated level of D-dimer is a prognostic sign of lung dysfunction after 3 months [67].
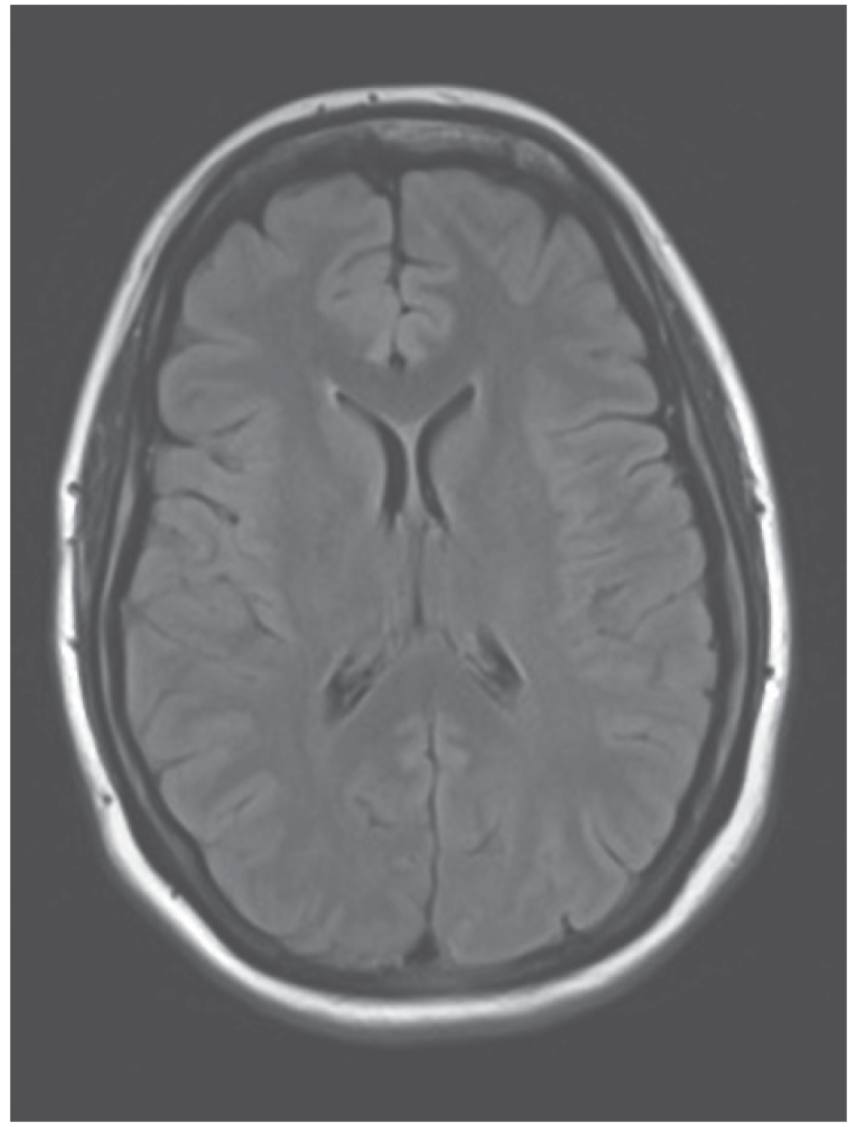
CENTRAL NERVOUS SYSTEMSARS-CoV-2 can enter brain tissue by viremia, as well as direct penetration into the olfactory nerve, resulting in anosmia. To date, the most common long-term neurological symptoms following COVID-19 are headache, dizziness, and chemosensory dysfunction (e.g., anosmia and ageusia).
Although stroke is a serious, albeit rare, consequence of acute COVID-19, encephalitis, seizures, and other conditions such as mood swings and brain fog have been reported within 2–3 months of onset [68]. However, due to the increased incidence of coagulopathy, people with long-term covid are at stroke risk [55]. These patients require neurorehabilitation to the same extent as other individuals with vascular lesions of the brain [56].
Past pandemics caused by viral pathogens (such as SARS-CoV-1, Middle East Respiratory Syndrome [MERS] coronavirus, and influenza) have had neuropsychiatric consequences that sometimes persist for months in “recovered” patients, which could seriously threaten overall cognitive health. A decrease in cognitive functions in the post-COVID period may be due to assisted ventilation of the lungs performed for patients in the acute period of severe COVID-19, as well as a high level of pro-inflammatory cytokines and acute respiratory dysfunction [25].
As suggested by O. Sinanović et al., in COVID-19 survivors in the coming years and decades, the inflammatory systemic process and/or inflammatory process in the brain can trigger long-term mechanisms that usually lead to an increase in neurological and neurodegenerative disorders [56].
Recently, more and more publications on the development of cognitive impairment against the background and in the long-term period of COVID-19 have appeared. In a review by T.M. Ostroumova et al. this problem is analyzed in detail and it is emphasized that risk factors for severe COVID-19 and cognitive impairment are largely combined and include older age, obesity and the presence of comorbid diseases such as arterial hypertension and type-2 diabetes mellitus. Such patients are potentially at high risk of developing cognitive impairment [3]. This review also mentions the work of C. Sasannejad et al. [53], which showed that cognitive impairment in some patients with acute respiratory distress syndrome (ARDS) persisted for 5 years after the illness. This study can be extrapolated to COVID-19. Moreover, the authors suggest using a battery of tests to detect cognitive impairment in this group of patients both in the acute period of the disease and in the long-term period.
The thesis about the need to use index indicators to differentiate different types and time scales of cognitive impairment should be recognized as important in the cited work. C. Sasannejad et al. [53] suggest that establishing the true cognitive impact of ARDS requires a distinction between patients with cognitive impairment before ARDS and those who develop new cognitive symptoms after ARDS. The Mini-Mental State Examination (MMSE) measures general memory impairment at that moment, but there are two limitations to its use in intensive-care units: the severity of patients and the inability to distinguish between delirium and dementia or their simultaneous presence. These limitations have led to the development of tools that are more sensitive to differentiating different types and timescales of cognitive impairment:
— a method for assessing confusion in the intensive-care unit (CAM-ICU, Confusion Assessment Method-Intensive Care Unit), which is an algorithm for diagnosing delirium; the method demonstrates high sensitivity and specificity in detecting delirium in patients with mechanical ventilation, including questions regarding the onset of changes in mental status, inattention, disorganized thinking, and changes in the patient’s level of consciousness [11];
— Modified Blessed Dementia Rating Scale (mBDRS);
— Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE);
— Mini-Mental State Examination (MMSE) for the screening of post-COVID patients.
ENDOCRINE SYSTEMThere may be long-term effects on the endocrine system in the months following COVID-19. This hypothesis was put forward based on what is known about the severe-acute-respiratory-syndrome coronavirus (SARS-CoV), which caused SARS in 2003. Patients infected with COVID-19 may be susceptible to viral damage to the pancreas, which leads to the development of diabetes. If this condition occurs, long-term follow-up is needed to understand whether the diabetes will be permanent or if SARS-CoV-2 caused a transient period of hyperglycemia that will disappear with recovery from the infection [39].
GASTROINTESTINAL TRACT AND THE HUMAN MICROBIOMEGastrointestinal involvement in COVID-19 is also associated with ACE2 receptors. The receptors are present in the glandular cells of the intestine, and viral capsid proteins have been found in the epithelium of the stomach, duodenum, and rectum, as well as in glandular enterocytes [33, 66]. Virus-induced alteration of the gut microbiome may contribute to the development of gastrointestinal symptoms [2, 34].
The incidence of complications of COVID-19 in the gastrointestinal tract ranges from 12–61% [49]. Gastrointestinal symptoms are associated only with a longer course of the disease, but not with mortality [9, 35, 47]. According to a recent meta-analysis of 29 studies (most of which were conducted in China), infection-induced gastrointestinal disturbances include anorexia (21–35%), nausea and/or vomiting (7–26%), diarrhea (9–33%), and pain in the stomach (3% or more).
Thus, the COVID-19 pandemic may affect the human microbiome in infected individuals, with significant long-term health impacts. While much remains uncertain or unknown about the virus and its consequences, the introduction of pandemic control practices could significantly impact the microbiome [18].
CONSEQUENCES OF HYPODYNAMIAElderly and senile people have been subjected to prolonged isolation due to the COVID-19 pandemic and, naturally, have significantly reduced their physical activity, which has led to the development of sarcopenia to varying degrees. As noted by T.O. Flatharta et al., unfortunately, during this period, medical professionals and public-health professionals have not been able to raise public awareness and find ways to reduce the development of sarcopenia and weakness [19].
In addition, the marked increase in inflammatory cytokines in COVID-19 leads to accelerated muscle breakdown and cachexia [41]. Loss of muscle mass can be further aggravated by immobilization during hospitalization while patients are in intensive-care units for mechanical ventilation. All people who have had COVID-19 should be tested for vitamin-D deficiency, as during prolonged isolation, lack of sunlight could significantly reduce its content [16].
In addition to muscle loss with prolonged covid, prolonged bed rest can lead to postural hypotension [11].
Moreover, vasculitis during COVID-19 can lead to damage to baroreceptors leading to autonomic dysregulation [6]. Elevated levels of cytokines can damage the autonomic nervous system. Postural orthostatic tachycardia has also been observed with prolonged COVID.
All of these factors can lead to an increase in the incidence of falls syndrome. People who fall frequently or are unstable are also likely to develop a “fear of falling” [
留言 (0)