
記住我
Patient safety is a priority for healthcare organisations worldwide, and it is a key step in providing high-quality care. Medication errors (MEs) are major concerns in hospitals because of their consequences for patients’ morbidity and mortality.1
Various terms have been used to define and classify MEs. However, the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) approves the following definition: “Any preventable event that may cause or lead to inappropriate medication use or patient harm, while the medication is in the control of the health care professional, patient, or consumer.”2
Hospitals and healthcare professionals aim to provide the safest care possible; however, MEs can occur during any stage of the medication-use process, including prescribing, transcribing, dispensing, administration, adherence and/or monitoring.2,3 Still, MEs most commonly occur during the prescribing stage.4
The World Health Organization (WHO) defines polypharmacy as the routine use of five or more medications.5 The inappropriate prescriptions of polypharmacy lead to adverse drug events and have been associated with a higher risk of hospitalization.6
Preventable MEs place a significant burden on healthcare organisations. In the United States, they can affect more than seven million patients and cost almost $21 billion annually across all care settings.1,7
It is alarming that up to 27.4% of intensive care unit (ICU) admissions are related to adverse drug events, with 48%–86% of those admissions being preventable MEs, as reported by a systematic review, which collected data from the 1980 s through 2014.8
Adverse drug events responsible for 5%–10% of hospital-isations.9,10 Hospital stays also lengthen when admissions involve adverse drug events with a high risk of mortality.8
Special attention should be given to this problem, particularly since ICU admissions are the most severe, potentially life-threatening cases. Such unplanned ICU admissions also greatly affect the healthcare system by, for example, limiting ICU availability to other patients, doubling the incremental additional length of stay and/or overloading the ICU with significant costs.11 Therefore, the objective of this research is to evaluate the MEs which require ICU admissions and to determine the cause of these MEs, the medication category involved and the associated mortality rate via a 6-month, prospective observational study.
2 Materials and methods 2.1 Study design and settingThe present paper employed a 6-month, prospective observational study design, which involved reviewing the medical charts of all newly admitted ICU patients from March 7,2019, to September 7, 2019. This study was conducted in the Salmanyia Medical Complex, which is an acute care, tertiary teaching hospital in Bahrain, with a capacity of 970 beds. The ICU is a 20-bed, closed unit providing a range of clinical services, including general medical, surgical, trauma, gynecological, and psychiatric care.
2.2 Patient populationAll adult patients aged ≥18 years, who were admitted to the ICU during the study period, were included in the study, with the exception of elective postoperative patients, who were admitted for observation. The institution's Research Ethics Board approved the study protocol. Informed consent from the patients was waived because all data were collected in daily practice without any specific interventions.
2.3 Observations and data collectionBaseline information was collected for each patient within 48 hours from ICU admission. This information included basic demographic data, reason for ICU admission and clinical information (including the patient's baseline chronic illnesses). Further medication information was collected from the institution's electronic system. Assessments were performed without any interventions or modifications of current therapies. The clinical consequences observed for recovery outcomes within 30 days after ICU discharge, as well as the length of ICU/hospital stay, were also recorded.
2.4 Admission screeningAll collected data were screened by the critical care clinical pharmacist to determine whether the patients’ ICU admissions were related to MEs using Micromedex, UpToDate and the summaries of product characteristics (SmPCs). Agreement from the consultant intensivist was required to confirm that the MEs were the main cause of ICU admission. If such confirmation was not received, the admission was included in the other group.
The costs of ICU admission and hospital stays were calculated based on the average cost of ICU and hospital admission per day. These data were obtained from the finance department, which determines the direct cost of hospitalization.
2.5 Statistical analysisData are presented as the mean ± standard deviation (SD), unless otherwise noted. Comparisons between the quantitative variables were drawn using Student's t test. Qualitative variables were reported as counts, and comparisons between independent groups were made using Pearson's chi-squared tests. All analyses were conducted using the Minitab® statistics programme, version 19.2020.1.
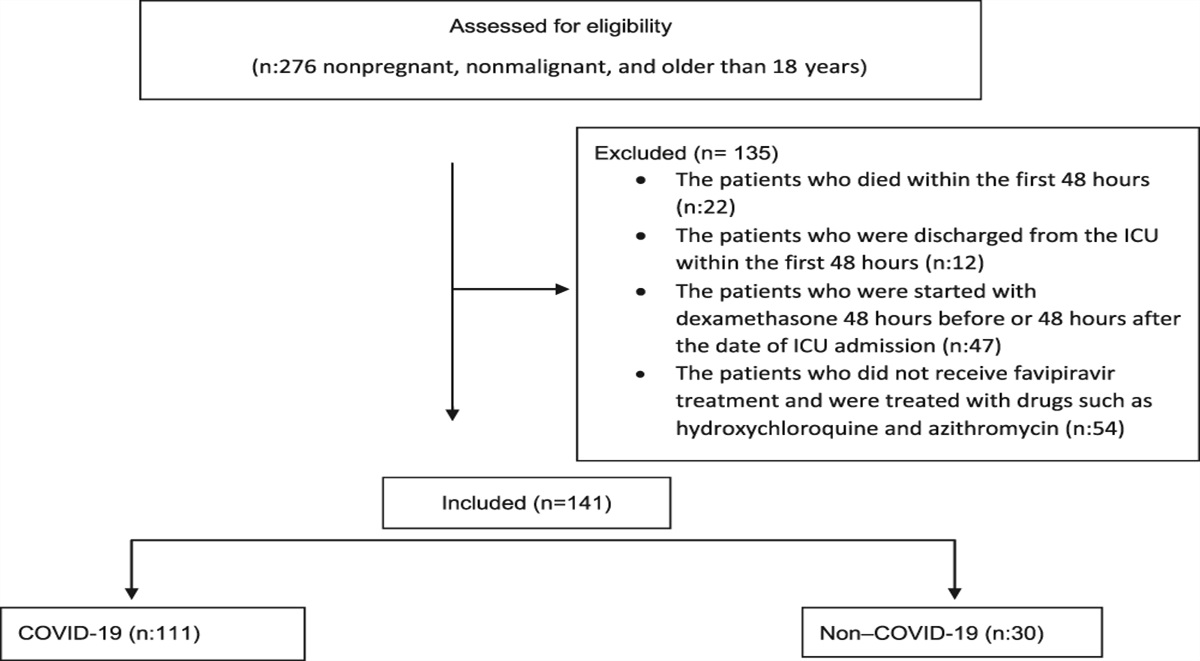
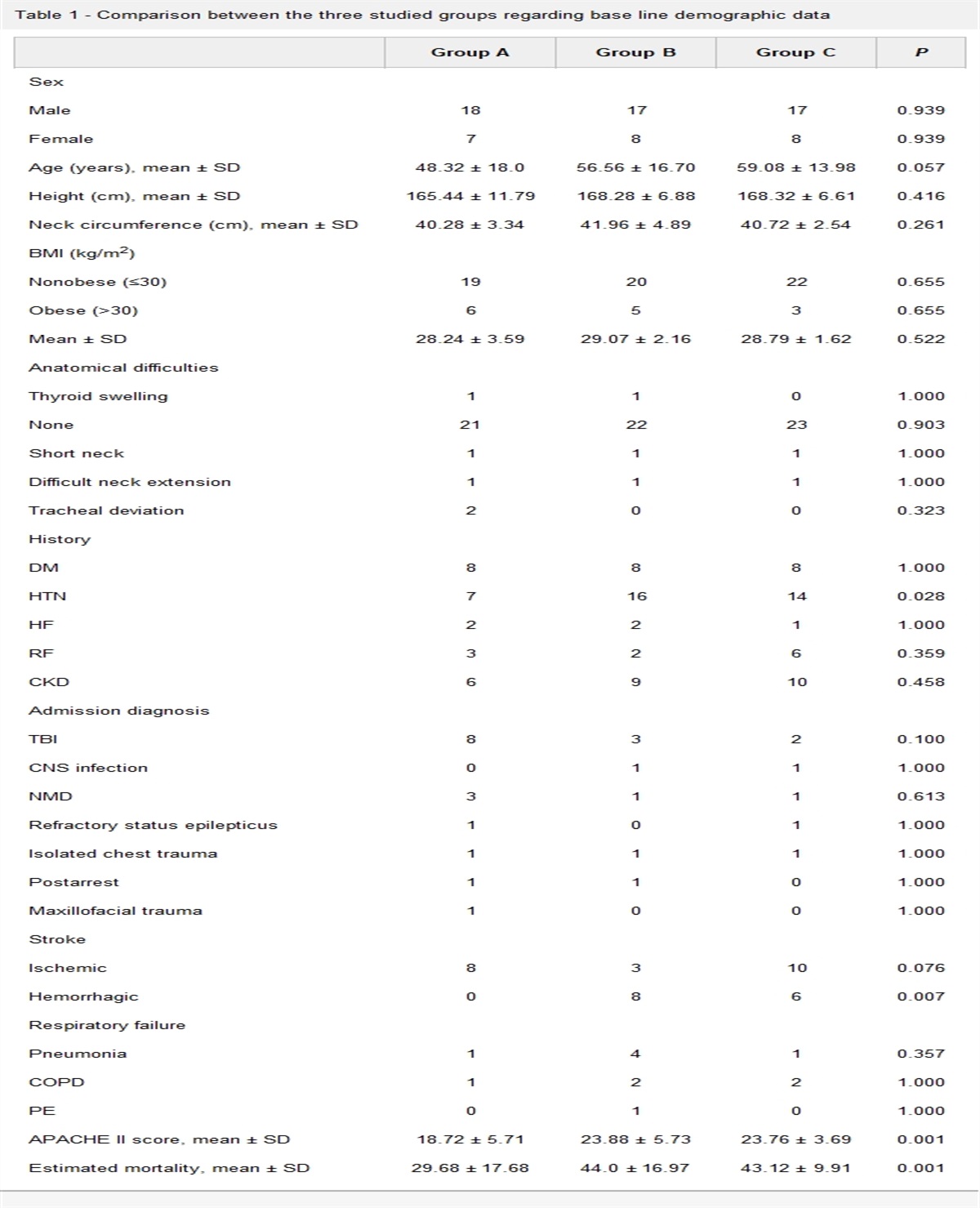
3 ResultsDuring the study period, 572 patients were admitted to the ICU, 395 were excluded from the analyses. Of these, 391 were electively admitted as postoperative patients; two were under 18 years of age; and a drug history was not clear for two patients (Fig. 1). Accordingly, 177 ICU patients were included, 26 patients were admitted to ICU due to MEs, and the remaining 155 patients admitted due to other causes. The mean age was: 50.89 ± 17.99years, Table 1 summarizes the characteristics of the population, and shows that there was no statistical difference between the two groups in regard to their age, gender nor the main presenting cause of admission. Polypharmacy (taking more than 5 medication before admission) was found to be more common among patient admitted with MEs and the result was statistically significant (P = .03).
 Figure 1:
Figure 1: Flow chart of the study.
Table 1 - Patient characteristics at admission to Intensive care unit All patients (n = 177) Admission related to MEs (n = 26) Admission unrelated to MEs (n = 151) P Age (mean ± SD) 50.887 ± 18.045 55.46 ± 16.68 50.10 ± 18.10 .16 Gender n (%) Male 91 (51.41%) 16 (61.54%) 75 (49.67%) .365 Female 86 (48.59%) 10 (38.46%) 76 (50.33%) Main cause of admission Shock 34 5 29 .99 Acute respiratory failure 47 4 43 .27 Metabolic derangement 34 5 29 .99 Cardiac disease other than shock 15 5 10 .06 Others∗ 47 7 40 .97 Polypharmacy ≥ 5 medications 65 (36.72%) 17 (65.38%) 48 (31.79%) .03 < 5medications 112 (63.28%) 9 (34.62%) 103 (68.21%)∗Hepatic failure, acute toxicity, Acute Cerebrovascular accident CVA, surgical emergency.
The MEs requiring ICU admission were categorized according to their therapeutic classification, origin of MEs and the types of errors. Anticoagulants were the most common medications involved in MEs (30.8%, almost one-third of the MEs), with a higher mortality rate (62.5%) (Table 2). The incidence of MEs occurred in outpatient clinics were higher than those occurred during hospital admission or during patient discharge, it accounts to 53.8% (Table 3). However mortality rate was higher with MEs occurred during hospital admission.
Table 2 - Frequency and Characteristics of MEs according to the ther apeutic classification Drug class % of error No. of patients 30-day mortality rate (%) Anticoagulant 30.8 8 62.5 Analgesic 7.7 2 0 Antidiabetic 11.5 3 0 Antihypertension 3.8 1 0 Antimicrobial 15.4 4 25 Antipsychotic 7.7 2 50 Other∗ 23.1 6 16.7∗Chemotherapeutic agent, antithyroid, skeletal muscle relaxant, chelating agent, Erythropoiesis-stimulating agent, electrolytes.
Type of MEs was categorized either as prescribing or dispensing error, 96% of MEs occurred during the prescription and only 4% had occurred during the dispensing process (Fig. 2). The prescribing errors were further categorized into misuse, overuse, and underuse.
 Figure 2:
Figure 2: Analysis of MEs by main cause, type.
The most frequent leading cause for prescribing errors was drug misuse (n = 15) including failure to perform biological follow-up (n = 7), serious drug interaction (n = 4), inappropriate dose prescribed (n = 2), and contraindication between drug and patient status (n = 2).
The average length of ICU stay was longer in MEs related admission in comparison to non-MEs admission 7.73 ± 4.43 days and 6.53 ± 4.003, respectively, but the difference was not statically significant. However, non-MEs related admission stayed in the hospital for longer duration in compared with MEs related admission 17.47 ± 18.01 days and 14.58 ± 9.21 days respectively, again the result was not statistically significant (Table 4). MEs related admission cost around $213,262 during their ICU admission
Table 4 - Length of stay and estimated admission cost All patients (n = 177) total Admission related to ME (n = 26) Admission unrelated to ME (n = 151) P CU length of stay (average number of days) 6.706 ± 4.078 7.73 ± 4.43 6.53 ± 4.003 .205 Hospital length of stay (average number of days) 17.05 ± 17.01 14.58 ± 9.21 17.47 ± 18.01 .218 Estimated cost of ICU admission (USD) $1,259,415 $213,262 $1,046,153 – Estimated cost of hospital admission (USD) $1,456,232 $141,644 $1,314,588 –There was no statistical difference in the mortality rate between the groups, neither ICU mortality, nor 30-day hospital mortality (Table 5).
Table 5 - Mortality rates All patients (n = 177) Admission related to MEs (n = 26) Admission unrelated to MEs (n = 151) P Likelihood ratio Mortality rate 59 (36.72%) 7 (26.92%) 52 (34.43%) .588 0.303 ICU mortality rate 42 3 39 .0008 0.0012 Hospital Mortality rate 17 4 13 .181 0.174Unplanned ICU admissions increase the burden on ICU resources. Preventable MEs, which require ICU admission, restrain ICU access for other patients, contribute to longer patient hospital stays and sometimes cause patient death.11
Therefore, we undertook a 6-month study to analyse admissions into the general ICU at our institution. Medication prescribed prior to admission were reviewed to determine if any MEs were present and, if so, whether those MEs were the main cause of admission. 14.6% of admissions to the ICU during the study period were related to MEs. Most of these serious MEs occurred during the prescription phase and were mainly due to inappropriate monitoring or follow-up and failure to prescribe medication despite the relevant indications.
The incidence of MEs related to ICU admission in this study was similar to that in previous studies, which have reported the rate of admission due to preventable adverse drug events as reaching 14%.11–17 In 2000, the Institution of Medicine (IOM) reported that more than 7000 deaths from MEs occur annually.1 During the present study, the 30-day mortality rate was 26% due to MEs. However, we observed no difference between the mortality rates among patients admitted to the ICU for MEs and those admitted for other reasons. This was comparable to previous results, which have found a 25.2% mortality rate from preventable adverse events, with no significant difference from other causes of ICU admission.12 The present study was conducted in a tertiary hospital ICU with non-elective admission of high-risk patient groups (e.g., terminal cancer patients and critical surgical cases), which could explain the high mortality rate.
MEs are common consequences of polypharmacy (the prescription of five or more medications to one patient). The WHO has reported that, with polypharmacy, the rate of prescribing errors can reach 30%.18 In this study, 17 out of 26 MEs (65%) occurred in patients who were receiving more than five medications (P = .03).
We identified certain pharmacological groups as being associated with a high risk of MEs. Anticoagulant medications —including vitamin K antagonists (VKAs), non-vitamin K antagonist oral anticoagulants (NOACs) and low-molecular-weight heparins (LMWHs)—were the most frequent cause of ME-related ICU admissions (8 patients; 30.8%). All of these MEs are related to incorrect prescriptions: insufficient doses, drug interactions, overdoses or the absence of prophylaxis except one error related to incorrect dispensing of warfarin. These data are similar to previous reports, which have demonstrated that MEs occur more often with anticoagulants than with any other medication category.19,20 It has also been noted that the 30-day mortality rate in this research was high (62%) in patients who experienced an anticoagulant MEs compared to errors with other medication types. Three deaths were attributed to bleeding and two to thromboembolism. Almost two-thirds of the anticoagulant MEs occurred during hospitalisation (at admission, while in the hospital or at the point of discharge) and were associated with the elevated 30-day mortality rate (4 out of 5). The root cause of most prescription errors was excess anticoagulant administration without appropriate monitoring/follow-up, resulting in abnormal coagulation defects and serious bleeding. The omission of anticoagulants, despite relevant indications for treatment and/or thromboembolism prevention (prophylaxis) in patients with deep vein thrombosis, pulmonary embolisms, atrial fibrillation, and/or mechanical heart valves, was the second most common error leading to failure of appropriate patient management and serious thromboembolic events. Essential laboratory tests were not performed during hospitalisation, and bleeding with high international normalized ratio (INR) levels after the administration of a VKA (warfarin) was reported, which led to intracranial haemorrhage in two cases. Though anticoagulants are classified as high-alert medications by the Institute of Safe Medication Practice (ISMP), as they can lead to a high risk of harm if used in error,21 no independent double-checking was done before warfarin was dispensed by the primary care pharmacy.
Antimicrobial drugs are also particularly important because they are widely and empirically used, generally ill-judged with a high frequency of errors.22 Antimicrobials were responsible for 15.3% of MEs ICU admissions and 14.3% of the mortalities. We noted that some of these MEs were related to drug-drug interactions between antibiotic medications (especially ciprofloxacin) and anticoagulants (warfarin). Concomitant use induced high INR and bleeding. Generally, those patients had multiple comorbidities, which further complicated the conditions.
The main causes of prescribing errors were inappropriate monitoring or follow-up, including failure to perform necessary laboratory analyses or to monitor liver and kidney function, which required therapy modifications (27%; seven patients). Another important cause was failure to prescribe a drug when its necessity was indicated (23%; six patients).
Almost all MEs occurred during the prescribing phase, which indicates that the problem is more related to physicians than to nurses or pharmacists.
We also assessed the cost of ICU admission and length of stay. No differences were observed between the admission related to MEs or other causes. While the total cost related to admissions for preventable MEs roughly accounted for $213,262 USD over the 6-month study period.
Preventing MEs is a complex process, with many limiting factors, such as available resources, policies and implications, background levels of training among hospital staff members (including pharmacists, doctors, and nurses), available competencies and an effective and self-correcting supervision system. Though many measures were taken to reduce MEs at all steps in the healthcare process, the rate of MEs remained high. We, therefore, recommend that education, awareness, better decision-making support, functional drug alerts (e.g., hard stop, explanation), medication reconciliation, involvement of a clinical pharmacist and other actions are necessary for physicians to decrease ME incidents. Quality improvement initiatives are critical to reduce anticoagulant-associated MEs.
Our study has some limitations, first, it is a single-center study; thus, it may not be possible to generalize the findings to other institutions. Second is that the cost was not accurate due to lack of cost accounting software in our hospital, accordingly, the cost presented above was only the average estimated one which does not reflect the charges for all procedures, services, laboratory tests, medications, etc. However, to our knowledge, this is the first study in the Middle East to assess general ICU admissions related to MEs.
5 ConclusionsThere is a high incidence of MEs requiring ICU admission, anticoagulant was the most common medication encountered and was associated with a high mortality rate. Close monitoring of patient on anticoagulants would provide a better safety profile and can decrease healthcare expenditures.
AcknowledgementsNone.
References [1]. Kohn LT, Corrigan J, Donaldson Molla S. Institute of Medicine Committee on Quality of Health Care in America. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000. [2]. Nebeker JR, Barach P, Samore MH. Clarifying adverse drug events: a clinician's guide to terminology, documentation, and reporting. AnnIntern Med 2004;140:795–801. [3]. US. Department of Health and Human Services. Office of Disease Prevention and Health Promotion. Washington, DC: National Plan for Adverse Drug Event Prevention; 2014 available from https://health.gov/sites/default/files/2019-09/ADE-Action-Plan-508c.pdf. [4]. Aljadhey H, Mahmoud MA, Mayet A, Alshaikh M, Ahmed Y, Murray MD, Bates DW. Incidence of adverse drug events in an academic hospital: A prospective cohort study. Int J Qual Health Care 2013;25:648–655. [5]. World Health Organization. Medication safety in polypharmacy, https://apps.who.int/iris/bitstream/handle/10665/325454/WHO-UHC-SDS-2019.11-eng.pdf?ua=1; 2019. Accessed February 5, 2020. [6]. Toshikazu Abe, Nanako Tamiya, Takako Kitahara, Yasuharu Tokuda. Polypharmacy as a risk factor for hospital admission among ambulance-transported old-old patients. Acute Med Surg 2016;3:107–113. [7]. Brianna A, da Silva, Mahesh Krishnamurthy. The alarming reality of medication error: A patient case and review of Pennsylvania and National data Internal Medicine Residency Program. J Community Hosp intern Med Perspect 2016;6(4):31758. 7. [8]. Jolivat PA, Hndlet P, Pichereau C, et al. A systematic review of adult admissions to ICUs related to adverse drug events. Crit Care 2014;18:643. [9]. Beijer HJ, de Blaey CJ. Hospitalizations caused by adverse drug reactions (ADR): A meta-analysis of observational studies. Pharm World Sci 2002;24:46–54. [10]. Kongkaew C, Noyce PR, Ashcroft DM. Hospital admissions associated with adverse drug reactions: A systematic review of prospective observational studies. Ann Pharmacother 2008;42:1017–1025. [11]. Nazer H, Eljaber R, Rimawi D, Hawari FI. Adverse drug events resulting in admission to the intensive care unit in oncology patients: Incidence, characteristics and associated cost. J Oncol Pharm Pract 2013;19(4):298–304. [12]. Marquet K, Claes N, De Troy E, et al. One fourth of unplanned transfers to a higher level of care are associated with a highly preventable adverse event: A patient record review in six Belgian hospitals. Crit Care Med 2015;43(5):1053–1061. [13]. Lama El Damn, Iman Basheti. Preventability analysis of adverse drug reactions in a Jordanian hospital: A prospective observational study. Int J Clin Pharm 2019;41(6):1599–1610. [14]. Phillips AL, Nigro O, Macolino KA, et al. Hospital admissions caused by adverse drug events: An Australian prospective study. Aust Health Rev 2014;38(1):51–57. [15]. Peyriere H, Cassan S, Floutard E, et al. Adverse drug events associated with hospital admission. Ann Pharmacother 2003;37(1):5–11. [16]. Schi⊘ler T, Lipczak H, Pedersen BL, et al. Danish Adverse Event Study: Incidence of adverse events in hospitals. A retrospective study of medical records. Ugeskr Laeger 2001;163:5370–5378. [17]. Pirmohamed M, James S, Meakin S, et al. Adverse drug reactions as cause of admission to hospital: Prospective analysis of 18 820 patients. BMJ 2004;329(7456):15–19. [18]. Medication ErrorsTechnical Series on Safer Primary Care. Geneva: World Health Organization; 2016. http://apps.who.int/iris/bitstream/handle/10665/252274/9789241511643eng.pdf?sequence=1; [Accessed 22 March 2020]. [19]. Piazza G, Nguyen T, Cios D, et al. Anticoagulation-associated adverse drug event. Am J Med 2011;124(12):1136–1142. [20]. Classen DC, Jaser L, Budnitz DS. Adverse drug events among hospitalized Medicare patients: Epidemiology and national estimates from a new approach to surveillance. Jt Comm J Qual Patient Saf 2010;36:12–21. [21]. Institute for Safe Medication Practices. ISMP list of high-alert medications in acute care settings, https://www.ismp.org/sites/default/files/attachments/2018-08/highAlert2018-Acute-Final.pdf; 2018 [accessed 20 March 2020]. [22]. Leekha S, Terrell CL, Edson RS. General principles of antimicrobial therapy. Mayo Clin Proc 2011;862:156–167.
留言 (0)