
記住我
Coronavirus disease 2019 (COVID-19) is a disease that causes high mortality rates throughout the world.1,2 It has caused approximately 1.25 million deaths worldwide,3 and this number is increasing day by day. The reason for these deaths is suspected to be hyperinflammation and acute respiratory syndrome (ARDS).4 A cytokine storm (hyperinflammatory syndrome) develops because of the complex activation of excessive and uncontrolled release of cytokines. Treatments that suppress the cytokine storm are frequently tried in COVID-19. Corticosteroids, IL-6 inhibitors, cytokine adsorption devices, intravenous immunoglobulin, hydroxychloroquine, and PD-1 checkpoint inhibitors are used as cytokine storm suppressor therapies.4
In a randomized controlled trial that was conducted between 2013 and 2018 in Spain, the effect of dexamethasone on mortality in ARDS was investigated. It was concluded that early administration of dexamethasone could reduce mortality.5 The RECOVERY Collaborative Group showed that the patients who received dexamethasone had lower 28-day mortality than the patients who did not.6 We frequently use dexamethasone as an anti-inflammatory treatment in patients hospitalized in our intensive care unit (ICU) with COVID-19. In this study, we compared the length of stay in the ICU and the mortality rates of the patients who received dexamethasone and those who did not.
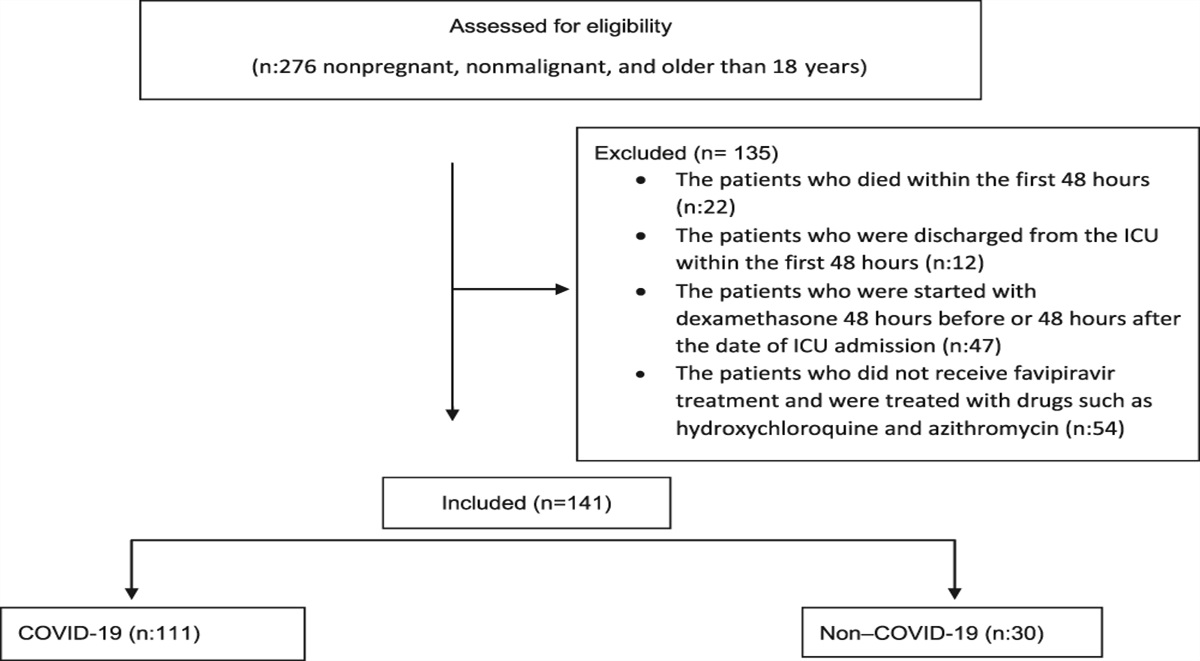
MethodsThis study was approved by the Tepecik Training and Research Hospital local Ethics Committee (No. 2020/02-69). This study was conducted in our ICU specialized in the isolation of patients with COVID-19 who needed intensive care. As this study was retrospective, the patients' consent was waived. Between March 11, 2020, and January 31, 2021, 276 nonpregnant, nonmalignant, and patients older than 18 years admitted to our ICU for COVID-19 were examined. Twenty-two patients died within the first 48 hours, and 12 patients were discharged from the ICU within the first 48 hours. Fifty-four of the 242 patients did not receive favipiravir treatment and were treated with drugs such as hydroxychloroquine and azithromycin, which were considered ineffective. A total of 47 patients were started with dexamethasone 48 hours before or 48 hours after the date of ICU admission. After these patients were excluded to reduce nonhomogeneity of the study population, 141 patients were examined. Group 1 included 111 patients who received dexamethasone (intravenous; 6 mg for 10 days), and group 2 consisted of 30 patients who did not receive dexamethasone (Figure 1). At the beginning of the pandemic, we did not routinely give dexamethasone treatment to patients. Especially after the RECOVERY trial, we often started to use dexamethasone treatment in patients who had ARDS with COVID-19. For this reason, we have fewer patients in group 2 than in group 1. According to the guideline of the Ministry of Health of Turkey on COVID-19 treatment, patients who needed oxygen support followed in the ICU.7 Dexamethasone was given to the patients who needed oxygen support with a PaO2/FiO2 lower than 200 mmHg in our ICU.
 Figure 1.:
Figure 1.: Flowchart.
Age, sex, comorbidities, the Assessment of Chronic Health and Acute Physiology II (APACHE II) score, and patient treatments were recorded. The mortality, the length of stay in ICU, the need for invasive mechanical ventilation (IMV), biochemical parameters, coagulation parameters, and arterial blood gas parameters were examined on day 0 (dexamethasone start date), 7, and 14 after the start of dexamethasone treatment. The medical records of the patients were reviewed by an infectious disease specialist, and the patients were screened for whether they had a culture-positive secondary infection.
The data were presented as the number of cases, percentage, mean (standard deviation), or median (minimum and maximum). Categorical comparisons were made using chi-square or Fischer tests. The Mann-Whitney U test was used to compare the continuous variables. The Friedman and Wilcoxon signed-rank tests were used to assess differences in the paired data. A value of p < 0.05 was considered statistically significant. A data analysis was performed with SPSS 22.0 statistical package (Statistical Package for the Social Sciences, USA).
ResultsThe mean age of the patients was 66 ± 13 years, and 85 (60%) were male. No difference was found between the two groups in age and sex (p = 0.10, p = 0.90, respectively). The most common comorbidities were hypertension (52%) and diabetes mellitus (38%). Although the APACHE II score tended to be higher in group 1, no statistical significance was observed (p = 0.06). Group 1 patients had received more convalescent immune plasma treatment than group 2 (p = 0.03). The characteristic features of the patients are presented in Table 1.
Table 1 - Characteristics of patients with acute respiratory distress syndrome associated with COVID-19 Characteristics All Patients (n=141) Dexamethasone (n=111), Group 1 Nondexamethasone (n=30), Group 2 P value Age (year) ±SD 66±13 67±13 63±11 0.10 Sex (male), n (%) 85 (60) 67 (60) 18 (60) 0.90 APACHE II score 16 (10–41) 17 (9–41) 14 (11–28) 0.06 Medical history, n (%) Hypertension 75 (53) 63 (56) 12 (41) 0.18 Cardiovascular disease 30 (21) 23 (20) 7 (24) 0.64 Diabetes mellitus 55 (39) 46 (41) 9 (31) 0.35 Chronic pulmonary disease 14 (9) 11 (9) 3 (10) 0.91 Other treatments, n (%) Convalescent plasma 69 (48) 60 (54) 9 (30) 0.04 Intravenous immunoglobulin 4 (2.8) 2 (1.8) 2 (6.7) 0.18 Tocilizumab 3 (2) 3 (2.7) 0 (0) 1.00 PaO2/FiO2 ratio, mmHg 99 [65–153] 107 [77–164] 98 [64–151] 0.45 Day 0 IMV, n (%) 34 (24) 25 (22) 9 (30) 0.33 Day 7 IMV, n (%) (n=112)* 74 (66) 65 (70) 9 (45) 0.02 Day 14 IMV, n (%) (n=62)** 48 (77) 45 (81) 3 (42) 0.04 Length of stay in hospital (d) 16 (3–98) 17 (3–73) 14.5 (3–98) 0.65 Length of stay in intensive care (d) 12 (3–74) 13 (3–74) 8 (3–50) 0.01 28-day mortality, n (%) 84 (60) 72 (64) 14 (46) 0.07 Secondary infection, n (%) 40 (28%) 36 (32%) 4 (13%) 0.04 Ventilator-associated pneumonia, n (%) 26 (19%) 26(23%) 3 (10%) 0.10 Bloodstream infection, n (%) 6 (4%) 5(4%) 1 (3%) 1.00 Urinary tract infection, n (%) 6 (4.1%) 6(4.5%) 0 (0%) 1.00*Number of the patients who were still treated in ICU on the 7th day.
**Number of the patients who were still treated in ICU on the 14th day.
Mortality at 28 day was 72 (64%) in group 1 and 14 (46%) in group 2 (p = 0.07). No difference in the length of hospital stay was noted between the two groups (p = 0.65). The length of stay in the ICU was longer in group 1 (median [minimum-maximum] 8 [3–50] versus 13 [3–74], p = 0.01).
The patients in group 1 who underwent IMV were as follows: 24 (21%) on the day of hospitalization, 63 (71%) on the 7th day, and 44 (81%) on the 14th day. No significant difference was observed in the need for IMV on the day of ICU admission between the groups (p = 0.33). However, an increase was seen in the need for IMV in group 1 on the 7th and 14th days when compared with group 2 (p = 0.03, p = 0.04, respectively) (Table 1).
The data on the development of culture-positive secondary infections were collected daily until day 28. Of the total patients, 40 had secondary infections on the 28th day (28%), including 36 (32%) in group 1 and four (13%) in group 2. The number of culture-positive secondary infections was higher in group 1 than in group 2 (p = 0.07). The most common diseases were ventilator-associated pneumonia 26 (19%), bloodstream infection 6 (4%), and urinary tract infection 6 (4%). Acinetobacter infections were present in 10 (27%) patients in group 1, whereas it was present in only one of the four patients in group 2. One patient had Candida glabrata growth, and another had Candida parapsilosis, both in group 1 (Table 1).
Hemoglobin and platelet levels decreased in group 1 on days 7 and 14 (p < 0.001 and p < 0.001 for hemoglobin and p = 0.001 and p < 0.001 for platelets, respectively) while they did not change in group 2 (p = 0.14 and p = 0.89 for hemoglobin and p = 0.18 and p = 0.60 for platelets, respectively) (Figure 2).
 Figure 2:
Figure 2: . Hemoglobin levels decreased in group 1 on days 7 and 14 (p < 0.001 and p < 0.001). Platelet levels decreased in group 1 on days 7 and 14 (p = 0.001 and p < 0.001 for platelets, respectively). Neutrophil count increased on day 7 (p = 0.001), while it did not on day 14 in group 1. In group 2, no changes were noted in the level of neutrophils on the seventh day (p = 0.17). Lymphocyte count was not differentiated on day 7 (p = 0.65). In group 1, an increase in the lymphocyte count was observed on day 14 compared with day 7 (p < 0.01). We observed a decrease in the level of lymphocytes (p <0.01). When the two groups were compared, we found that the lymphocyte count was lower on the seventh day in group 1 (p <0.001). In group 1, C-reactive protein (CRP) significantly decreased on the seventh day, but not in group 2 (p < 0.001, p = 0.90, respectively). The CRP level in group 1 was found to be significantly higher than in group 2 on the first day (p < 0.01). In group 1, the procalcitonin level increased on the seventh day and decreased on the 14th day (p < 0.001, p = 0.001, respectively), while it did not in group 2 (p = 0.15, p = 0.75, respectively). The lactate dehydrogenase (LDH) decreased at 7 and 14 days in group 1 (p < 0.01, p = 0.03, respectively). However, LDH was lower in group 2 than in group 1 on the seventh day (p = 0.01). A significant increase in D-dimer was observed in group 1 on day 7, but a similar increase was not observed in group 2 (p < 0.001, p = 0.30, respectively). *Statistically significant difference in the parameter from 0 to 7th day in the same groups. ** Statistically significant difference in the parameter from supine to 7th to 14th day in the same groups. *** Statistically significant difference in the parameter detected when compared between groups at the same time point.
In group 1, an increase in the neutrophil and white blood cell counts was observed, but no significant changes were observed in the lymphocyte count on the seventh day (p = 0.001, p = 0.001, p = 0.65, respectively). In group 1, an increase in the lymphocyte count was observed on day 14 compared with day 7 (p < 0.01), while the level of neutrophils did not change. In group 2, no changes were noted in the level of neutrophils on the seventh day (p = 0.17), but we observed a decrease in the level of lymphocytes (p <0.01). When the two groups were compared, we found that the lymphocyte count was lower on the seventh day in group 1 (p <0.001).
The C-reactive protein (CRP) significantly decreased in group 1 on the seventh day, but not in group 2 (p < 0.001, p = 0.90, respectively). The CRP level in group 1 was found to be significantly higher than in group 2 on the first day (p < 0.01). In group 1, the procalcitonin level increased on the seventh day and decreased on the 14th day (p < 0.001, p = 0.001, respectively), while it did not in group 2 (p = 0.15, p = 0.75, respectively). The lactate dehydrogenase (LDH) decreased at 7 and 14 days in group 1 (p < 0.01, p = 0.03, respectively). However, LDH was lower in group 2 than in group 1 on the seventh day (p = 0.01). A significant increase in D-dimer was observed in group 1 on day 7, but a similar increase was not observed in group 2 (p < 0.001, p = 0.30, respectively).
DiscussionIn this retrospective single-center study, we compared the mortality and length of stay in the ICU in critically ill patients with COVID-19 who received dexamethasone and those who did not. A benefit in mortality could not be demonstrated. The length of stay in the ICU and secondary infection in ICU were higher in the group receiving dexamethasone than in the usual care group.
Dexamethasone, one of the corticosteroids, can be used in many diseases and conditions (anti-inflammatory activity, antiedema activity, etc.).8 In the past, corticosteroid treatment has also been used in diseases with hyperinflammation and ARDS.9 Dexamethasone, a synthetic glucocorticoid, has been used in the treatment of COVID-19, which is a viral infection with severe ARDS and hyperinflammation.1,5,6 A total of 6,425 hospitalized patients who received dexamethasone (n = 2,104) and those who did not (n = 4321) were evaluated in a randomized controlled study by the RECOVERY study group. A significant reduction in mortality was found in the group that received dexamethasone.6 In our retrospective study, a benefit in mortality could not be demonstrated. In CoDEX study, it was found that dexamethasone did not reduce mortality and length of stay in the intensive care unit.10 The high APACHE II score of the patients who received dexamethasone (it tended to be higher although not statistically significant) and the significantly higher CRP value indicated that the severity of the disease in this group was high.
Other studies (including the RECOVERY study group) have shown that dexamethasone treatment reduces the need for mechanical ventilation in patients with COVID-19, shortens the stay in the intensive care unit, and reduces mortality.1,5,6 On the contrary, the CoDEX study showed that dexamethasone did not positively contribute to mortality, length of stay in the intensive care unit, and the need for mechanical ventilation.10 In this study, no difference was observed in the number of patients requiring IMV on day 0. On days 7 and 14 after the start of dexamethasone treatment, IMV rates were found to be significantly higher in the dexamethasone group. However, our results could be attributed to nonhomogeneity due to the higher APACHE II score and the level of CRP in the group who received dexamethasone.
One of the most common side effects of corticosteroid use is a possible increase in infection rates. Secondary infections are frequent among patients with COVID-19 requiring ICU, particularly in patients who die in the hospital.11-13 We encountered the most common secondary infections as ventilator-associated pneumonia, bloodstream infection, and urinary system infection, respectively. The most common microorganism encountered was Acinetobacter baumannii. A CoDEX trial showed that using dexamethasone did not increase secondary infection rates.10
It is well documented that CRP increases inflammatory processes.4,14,15 CRP was higher in the group that received dexamethasone. There was a decrease in CRP with dexamethasone treatment on day 7. However, on the 14th day, again, a significant increase was observed. This may be due to an intercurrent infection, or it may be the result of insufficient immunosuppression therapy for COVID-19. Therefore, when an increase in CRP in patients receiving dexamethasone treatment occurs, coinfection should be excluded. If coinfection is excluded, it would be appropriate to evaluate these patients for additional immunosuppressed therapy. In some recent studies in the literature, the use of pulse steroid and interleukin 6 antagonists as additional immunosuppressant therapy is recommended in patients with high CRP and the need for oxygen.16–18
The decrease in hemoglobin and platelet counts may have occurred due to complementary activation, thrombotic microangiopathy, and prolonged inflammation caused by COVID-19.19,20 The hemoglobin and platelet counts were significantly lower in the group receiving dexamethasone than in the patients who did not receive dexamethasone. Taking into account that the level of CRP was also high in the group that received dexamethasone, this situation may have developed as a consequence of bone marrow suppression caused by excessive cytokine release, inflammation, and thrombotic microangiopathy.15,19,20 We found that CRP levels decreased but remained high or increased during dexamethasone treatment follow-up. Studies with higher doses or longer time frames for dexamethasone administration or other immunosuppressive therapy are needed in patients with COVID-19. The significant increase in the neutrophil and leukocyte counts and the decrease in the lymphocyte count in the dexamethasone group were the expected results from using corticosteroids.21
D-dimer is a fibrin breakdown product that occurs after fibrinolysis. It is widely used in the diagnosis of conditions such as pulmonary embolism and deep vein thrombosis.22,23 It is also used as a predictor of mortality and a parameter of disease progression in COVID-19.24 If the patients have hyperinflammation, the possibility of thrombosis increases.25 It has been shown that using corticosteroids creates a procoagulant state even in healthy individuals.26 Adding steroid therapy to hyperinflammation caused by COVID-19 may also contribute to increased D-dimer.27-29 In this study, the D-dimer level tended to increase over time in the group receiving dexamethasone. As we could attribute this increase to the high severity of the disease, using dexamethasone could have also affected this situation.18,27,28
LDH is a cytoplasmic enzyme that increases because of cell destruction in many conditions, such as cancer, organ damage, hemolysis, and inflammation. In this study, LDH was significantly lower in the group that received dexamethasone compared with the group that did not receive it. This could be interpreted as a decrease in cell damage caused by inflammation or, in other words, a suppression of inflammation.28,30
This study is a single-center study with a small number of patients. As this was a retrospective study, there was a lack of standardized protocol of management between two inhomogeneous groups. Therefore, bias cannot be ruled out. The difference in the severity of illness on admission may be because of two different waves of COVID-19. Variability of therapies such as convalescent plasma and tocilizumab might affect the outcome. In addition, there was the variability of immunomodulatory drugs used in our patients, and the findings on laboratory parameters cannot be attributed to the effects of dexamethasone alone. The fact that the number of patients and the severity of the disease could not be standardized for the two groups makes it difficult to interpret the results.
ConclusionsWe could not definitively show that dexamethasone benefits mortality in our patients with COVID-19 who were admitted to the intensive care unit. The length of stay in the intensive care unit was longer in the group that used dexamethasone. In addition, a higher percentage of secondary infections were observed in the patients who used dexamethasone than in the usual care group in ICU. Homogenization was not achieved in this study, which included a limited number of patients. Our results demonstrate that further studies may be needed on glucocorticoid therapy for COVID-19.
References [1]. Li X, Ma X. Acute respiratory failure in COVID-19: is it “typical” ARDS? Crit Care. 2020;24:198. [2]. Saghazadeh A, Rezaei N. Towards treatment planning of COVID-19: Rationale and hypothesis for the use of multiple immunosuppressive agents: Anti-antibodies, immunoglobulins, and corticosteroids. Int Immunopharmacol. 2020;84:106560. [3]. World Health Organization. Coronavirus Disease (COVID-19). 2020. Geneva, Switzerland: World Health Organization. [4]. Tang Y, Liu J, Zhang D, Xu Z, Ji J, Wen C. Cytokine storm in COVID-19: the current evidence and treatment strategies. Front Immunol. 2020;11:1708. [5]. Villar J, Ferrando C, Martínez D, Ambrós A, Muñoz T, Soler JA, Aguilar G, Alba F, González-Higueras E, Conesa LA, Martín-Rodríguez C, Díaz-Domínguez FJ, Serna-Grande P, Rivas R, Ferreres J, Belda J, Capilla L, Tallet A, Añón JM, Fernández RL, González-Martín JM; dexamethasone in ARDS network. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. Lancet Respir Med. 2020;8(3):267-276. [6]. RECOVERY Collaborative Group, Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, Linsell L, Staplin N, Brightling C, Ustianowski A, Elmahi E, Prudon B, Green C, Felton T, Chadwick D, Rege K, Fegan C, Chappell LC, Faust SN, Jaki T, Jeffery K, Montgomery A, Rowan K, Juszczak E, Baillie JK, Haynes R, Landray MJ. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021 Feb 25;384(8):693-704. [7]. Sağlık T.C. Bakanlığı Bilimsel Danışma Kurulu Çalışması. SAĞLIK BAKANLIĞI COVID-19 (SARS-CoV-2 ENFEKSİYONU) ERİŞKİN HASTA TEDAVİSİ. 2020. https://www.ekmud.org.tr/files/uploads/files/covid-19rehberieriskinhastatedavisipdf.pdf. Accessed August 2, 2022. [8]. Ramamoorthy S, Cidlowski JA. Corticosteroids: mechanisms of action in health and disease. Rheum Dis Clin North Am. 2016;42:15-31. [9]. Liu K, Fang YY, Deng Y, Liu W, Wang MF, Ma JP, Xiao W, Wang YN, Zhong MH, Li CH, Li GC, Liu HG. Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province. Chin Med J (Engl). 2020;133:1025-1031. [10]. Tomazini BM, Maia IS, Cavalcanti AB, Berwanger O, Rosa RG, Veiga VC, Avezum A, Lopes RD, Bueno FR, Silva MVAO, Baldassare FP, Costa ELV, Moura RAB, Honorato MO, Costa AN, Damiani LP, Lisboa T, Kawano-Dourado L, Zampieri FG, Olivato GB, Righy C, Amendola CP, Roepke RML, Freitas DHM, Forte DN, Freitas FGR, Fernandes CCF, Melro LMG, Junior GFS, Morais DC, Zung S, Machado FR, Azevedo LCP. COALITION COVID-19 Brazil III investigators. effect of dexamethasone on days alive and ventilator-free in patients with moderate or severe acute respiratory distress syndrome and COVID-19: The CoDEX randomized clinical trial. JAMA. 2020;324:1307-1316. [11]. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Liu L, Shan H, Lei CL, Hui DSC, Du B, Li LJ, Zeng G, Yuen KY, Chen RC, Tang CL, Wang T, Chen PY, Xiang J, Li SY, Wang JL, Liang ZJ, Peng YX, Wei L, Liu Y, Hu YH, Peng P, Wang JM, Liu JY, Chen Z, Li G, Zheng ZJ, Qiu SQ, Luo J, Ye CJ, Zhu SY, Zhong NS. China Medical Treatment Expert Group for Covid-19. clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708-1720. [12]. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497-506. [13]. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, Guan L, Wei Y, Li H, Wu X, Xu J, Tu S, Zhang Y, Chen H, Cao B. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054-1062. [14]. Gustine JN, Jones D. Immunopathology of hyperinflammation in COVID-19. Am J Pathol. 2021;191:4-17. [15]. Meanwatthana J, Majam T. Interleukin-6 antagonists: lessons from cytokine release syndrome to the therapeutic application in severe COVID-19 infection. J Pharm Pract. 2021;35:752-761. [16]. Maskin LP, Olarte GL, Palizas F Jr, Velo AE, Lurbet MF, Bonelli I, Baredes ND, Rodríguez PO. High dose dexamethasone treatment for acute respiratory distress syndrome secondary to COVID-19: a structured summary of a study protocol for a randomised controlled trial. Trials. 2020;21:743. [17]. Papamanoli A, Yoo J, Grewal P, Predun W, Hotelling J, Jacob R, Mojahedi A, Skopicki HA, Mansour M, Marcos LA, Kalogeropoulos AP. High-dose methylprednisolone in nonintubated patients with severe COVID-19 pneumonia. Eur J Clin Invest. 2021;51:e13458. [18]. RECOVERY Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Lancet. 2021;397:1637-1645. [19]. Chauhan AJ, Wiffen LJ, Brown TP. COVID-19: A collision of complement, coagulation and inflammatory pathways. J Thromb Haemost. 2020;18:2110-2117. [20]. Taneri PE, Gómez-Ochoa SA, Llanaj E, Raguindin PF, Rojas LZ, Roa-Díaz ZM, Salvador D Jr, Groothof D, Minder B, Kopp-Heim D, Hautz WE, Eisenga MF, Franco OH, Glisic M, Muka T. Anemia and iron metabolism in COVID-19: a systematic review and meta-analysis. Eur J Epidemiol. 2020;35:763-773. [21]. Kudo C. Major side effects of systemic glucocorticoid. Nihon Rinsho. 2015;73:317-321. [22]. Kearon C, de Wit K, Parpia S, Schulman S, Afilalo M, Hirsch A, Spencer FA, Sharma S, D'Aragon F, Deshaies JF, Le Gal G, Lazo-Langner A, Wu C, Rudd-Scott L, Bates SM, Julian JA; PEGeD Study Investigators. Diagnosis of pulmonary embolism with d-Dimer adjusted to clinical probability. N Engl J Med. 2019;381:2125-2134. [23]. Wells PS, Anderson DR, Rodger M, Forgie M, Kearon C, Dreyer J, Kovacs G, Mitchell M, Lewandowski B, Kovacs MJ. Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. N Engl J Med. 2003;349:1227-1235. [24]. Rostami M, Mansouritorghabeh H. D-dimer level in COVID-19 infection: a systematic review. Expert Rev Hematol. 2020;13:1265-1275. [25]. Libby P, Simon DI. Inflammation and thrombosis: the clot thickens. Circulation. 2001;103:1718-1720. [26]. Majoor CJ, Sneeboer MM, de Kievit A, Meijers JC, van der Poll T, Lutter R, Bel EH, Kamphuisen PW. The influence of corticosteroids on hemostasis in healthy subjects. J Thromb Haemost. 2016;14:716-723. [27]. Huang I, Pranata R, Lim MA, Oehadian A, Alisjahbana B. C-reactive protein, procalcitonin, D-dimer, and ferritin in severe coronavirus disease-2019: a meta-analysis. Ther Adv Respir Dis. 2020;14:1753466620937175. [28]. Zheng Z, Peng F, Xu B, Zhao J, Liu H, Peng J, Li Q, Jiang C, Zhou Y, Liu S, Ye C, Zhang P, Xing Y, Guo H, Tang W. Risk factors of critical and mortal COVID-19 cases: A systematic literature review and meta-analysis. J Infect. 2020;81:e16-e25. [29]. Terpos E, Ntanasis-Stathopoulos I, Elalamy I, Kastritis E, Sergentanis TN, Politou M, Psaltopoulou T, Gerotziafas G, Dimopoulos MA. Hematological findings and complications of COVID-19. Am J Hematol. 2020;95:834-847. [30]. Henry BM, Aggarwal G, Wong J, Benoit S, Vikse J, Plebani M, Lippi G. Lactate dehydrogenase levels predict coronavirus disease 2019 (COVID-19) severity and mortality: A pooled analysis. Am J Emerg Med. 2020;38:1722-1726.
留言 (0)