
記住我
Coronary artery disease (CAD) is the most widespread cardiac disorder globally; even its mortality exceeds that of cancers annually. During the past 20 years, the battle to reduce the incidence of arterial thrombosis has led researchers to the discovery of various clinical markers. There are some cases with arterial thrombosis which did not have any of the traditional risk factors. Hence, the researchers focused on other predisposing factors, which may contribute to arterial thrombosis. Researchers exerted effort to find the possible positive link of soluble C-type lectin-like receptor 2 with ischemic heart disease.1
Soluble forms of platelet membrane proteins are secreted as a consequence of platelet activation, in which soluble C-type lectin-like receptor 2 (sCLEC-2) is released as a shed fragment.1
Researches' data supposed that CLEC-2 plays a pivotal role in atherothrombosis.2
Although the standard blood collection's procedure used in daily laboratory practice tests has shown to be efficient for sCLEC-2 reading, it has not yet been fully investigated.3 Endothelial dysfunction, lipid accumulation, leukocyte migration, and platelet activation are contributing factors to CAD.4
Platelet activation is mandatory for thrombotic events that follow atherosclerotic plaque rupture. Moreover, cytokines from activated platelets may activate leukocyte movement into the subendothelium, which then promotes atherosclerosis progression.5
CLEC-2 is a type II transmembrane receptor of the C-type lectin superfamily.6
CLEC-2 is a platelet activation receptor for the membrane protein podoplanin, which is expressed on some types of tumor cells and lymphatic endothelial cells.7
sCLEC-2 could be considered as a new biomarker of platelet activation. Elevated plasma levels of sCLEC-2 have been detected in thrombotic microangiopathy (TMA) and disseminated intravascular coagulation.8
We hypothesized that plasma CLEC-2 as an important regulator of atherothrombosis might reflect the extent of CAD, so we conducted this case-control study to evaluate the correlation between CLEC-2 and CAD and the relation between its level and severity of coronary heart disease “prognostic significance.”
2. Patients and methodsThis case-control study was performed in collaboration between critical care and internal medicine units at Cairo University Hospital and the National Heart Institute. This study was approved by Faculty of Medicine—Research Ethical Committee—with number (77–2022). It included 88 individuals divided into two groups.
Group I (cases group): 50 patients diagnosed with ST elevation myocardial infarction (STEMI). Group II (control group): 38 sex-matched and age-matched healthy individuals. 2.1. Inclusion criteriaInclusion criteria included adult patients older than 18 years, both sexes (male and female), and patients diagnosed with acute coronary syndrome by echocardiogram (ECG), echocardiography, and cardiac enzymes.
2.2. Exclusion criteriaExclusion criteria included younger than 18 years and patients with other cardiac diseases other than myocardial infarction (MI).
All patients who met the above mentioned criteria were subjected to full history taking, clinical examination, serum samples were withdrawn for cardiac enzymes detection (creatine kinase, creatine kinase myocardial band) by automated (COBAS INTEGRA) assessment and also lipid profile (including fasting 12–14 hours low density lipoprotein level, ECG, Echocardiography using (SIEMENS ACUSON X700) device, Diagnostic PCI was performed using (SIEMENS-MEGALIX/Cat plus 125/40/90-122GW) device, then accordingly, PCI to the affected vessels was done.
The tests of samples were stored in −20° C for the assessment of CLEC-2 immediately after admission to ICU and before catheterization using enzyme-linked immunosorbent assay (ELIZA) kit (Bioassay Technology Laboratory BT, Catalog No. E7512Hu). According to the manufacture, ELIZA reader STAT FAX was used to determine the absorbance against known standards. The results were then converted to pg/ml.
2.3. Primary outcomeThe primary outcome was to assess the association between plasma CLEC-2 and STEMI and its correlation with clinicolaboratory data.
2.4. Secondary outcomeThe secondary outcome was to assess whether plasma CLEC-2 can be used as a predictor of severity in acute coronary syndrome.
Furthermore, written informed consents were obtained from all participants demonstrating the study's purpose conforming Declaration of Helsinki (1964).
2.5. Sample sizeAccording to previous literature,1 the anticipated mean of soluble CLEC-2 in CAD cases was 144.04 pg/ml, while SD 37.92, and in controls 82.49, SD 25.38.9
The original paper had described the level in median and range, but the data were converted to mean and SD.2 Using G.Power sample size calculator at 0.01 alpha errors, with and power of 0.99, the effect size will be 1.910,11 and the minimum sample in each group is 15.
2.6. Statistical analysisAnalytical statistics using IBM Corporation's statistical package for the social sciences (SPSS) version 28, data were coded and input. For quantitative data, the mean, standard deviation, median, minimum and maximum were used to summarize the data; for categorical data, the relative frequency (%) and frequency (count) were used. Mann-Whitney and Kruskal-Wallis tests, which are nonparametric, were used to compare quantitative variables.12
An analysis of categorical data was done using the chi-square (χ2) test when the anticipated frequency is less than five, the exact test was utilized instead.13
The Spearman correlation coefficient was used to perform correlations between quantitative variables. P values regarded as statistically significant were less than 0.05.12–14
3. ResultsThis study included a total of 88 divided into two groups.
Group I (the cases group): 50 patients diagnosed with MI. Group II (control group): 38 sex-matched and age-matched control healthy individuals.Regarding group I, there were 37 (74%) men and 13 (26%) women. Age ranged from 38 to 83 years, with mean ± SD 57.9 ± 9.83 and median 60 years. Ten (20%) cases were diabetic, and 8 (16%) cases were hypertensive, whereas 11 (22%) cases were both diabetic and hypertensive. The smoking history was observed in 24 (48%) cases. CLEC-2 levels in group I were higher than in group II, P value <0.001, as presented in Table 1.
Table 1 - C lectin in two groups Cases Controls P value Median Minimum Maximum Median Minimum Maximum C-type lectin 203.50 29.00 2337.00 84.15 1.50 500.00 <0.001All patients presented with MI who were divided according to the site of infarction (by ECG) into lateral, anterior, anterolateral, inferior, and inferolateral STEMI being the anterior MI was the most common presentation. Data of echocardiography show that fair systolic function 40%–50% was found in 46% of cases, and dilated left ventricle was detected in 54%. One vessel was more detected than two or three vessels affection in 40% of cases, as presented in Table 2.
Table 2 - The different presentations and echo finding in group I Cases Count % Presentation Lateral STEMI 1 2.0 Inferolateral STEMI 2 4.0 Inferior STEMI 15 30.0 Anterolateral STEMI 2 4.0 Anterior STEMI 30 60.0 Systolic function Normal >50% 13 26.0 Fair 40–50% 23 46.0 Impaired <40% 14 28.0 Dilated LV Yes 27 54.0 No 23 46.0 Diastolic dysfunction Grade 1 25 50.0 Grade 2 15 30.0 Grade 3 8 16.0 No 1 2.0 Significant valve lesion Moderate eccentric MR 4 8.0 Moderate to severe MR 1 2.0 Severe MR 2 4.0 No 43 86.0 Number of vessels 1 20 40.0 2 17 34.0 3 13 26.0 Previous stent/graft Graft 1 2.0 Stent 2 4.0 No 47 94.0STEMI, ST elevation myocardial infarction.
CLEC-2 levels did not differ between men and women in this study and also were not affected by the history of diabetes or hypertension. Smoking history did not affect the CLEC-2 serum levels, as presented in Table 3.
Table 3 - Association between (CLEC-2) level and sex, comorbidities, and smoking history C-type lectin P value Median Minimum Maximum Sex 0.757 Male 203.50 29.00 1783.00 Female 197.40 38.20 2337.00 Comorbidities 0.612 DM 184.40 38.20 396.80 HTN 187.45 45.90 439.00 DM, HTN 197.40 42.80 2337.00 Smoking history 0.554 No 211.20 29.00 1783.00 Yes 197.40 29.00 1783.00CLEC-2, C-type lectin-like receptor 2; DM, diabetes mellitis; HTN, hypertension.
CLEC-2 serum levels were not affected by the site of MI nor the systolic function outcome. Outcome variables were normal discharge, vasopressor usage, and mortality. CLEC-2 serum levels were higher in patients with dilated left ventricle and those with diastolic dysfunction; however, these findings were not statistically significant, as presented in Table 4.
Table 4 - Association between (CLEC-2) level and different presentation, the number of occluded vessels, left ventricle, systolic function, and the degree of diastolic dysfunction C-type lectin P value Mean SD Median Minimum Maximum Presentation 0.409 Lateral STEMI 2337.00 2337.00 2337.00 2337.00 Inferolateral STEMI 137.70 84.43 137.70 78.00 197.40 Inferior STEMI 343.21 453.13 153.00 29.00 1783.00 Anterolateral STEMI 249.90 137.04 249.90 153.00 346.80 Anterior STEMI 243.95 190.51 215.00 42.80 1021.00 Systolic function 0.727 Normal 371.03 622.25 191.30 29.00 2337.00 Fair 320.72 383.75 205.10 42.80 1783.00 Impaired 241.34 144.78 215.75 52.00 520.30 Dilated LV 0.459 Yes 330.71 449.57 228.00 45.90 2337.00 No 289.11 369.23 191.30 29.00 1783.00 Diastolic dysf 0.398 Grade1 283.13 362.13 197.40 29.00 1783.00 Grade2 255.09 233.11 191.30 65.80 1021.00 Grade3 273.01 151.19 257.85 52.00 500.00 No 153.00 153.00 153.00 153.00 Significant valve lesion 0.788 Moderate eccentric MR 261.50 166.37 298.60 52.00 396.80 Moderate to severe MR 228.00 228.00 228.00 228.00 Severe MR 137.70 21.64 137.70 122.40 153.00 No 326.26 439.30 203.50 29.00 2337.00 Number of vessels 0.235 1 410.07 515.43 249.45 42.80 2337.00 2 205.02 150.86 172.90 29.00 553.10 3 299.38 454.12 197.40 52.00 1783.00 Previous stent/graft 0.637 Graft 197.40 197.40 197.40 197.40 Stent 132.35 76.86 132.35 78.00 186.70 No 321.63 421.89 205.10 29.00 2337.00 LAD 0.848 Affected 270.90 297.34 203.50 29.00 1783.00 Normal 561.41 822.02 148.40 58.10 2337.00 RCA 0.151 Affected 220.01 176.44 153.00 52.00 748.50 Normal 403.14 544.26 221.90 29.00 2337.00 LCX 0.273 Affected 382.16 645.23 153.00 38.20 2337.00 Normal 275.21 215.50 205.10 29.00 1021.00 Angiography report 0.538 RCA 293.83 226.66 182.10 58.10 748.50 OM 906.00 1240.27 906.00 29.00 1783.00 LCX, RCA 78.00 78.00 78.00 78.00 LCX 902.93 1242.37 218.80 153.00 2337.00 LAD, LCX 88.00 31.40 88.00 65.80 110.20 LAD and OM 120.85 116.88 120.85 38.20 203.50 LAD 251.24 196.63 221.90 42.80 1021.00 CABAG 393.70 393.70 393.70 393.70 AGGRESTAT 153.00 153.00 153.00 153.00 Need for other PCI 0.073 Yes 287.04 506.88 120.90 29.00 1783.00 No 318.49 387.23 211.20 38.20 2337.00 Outcome 0.640 Inotropes 213.87 155.77 127.00 120.90 393.70 Discharge 318.10 434.96 203.50 29.00 2337.00 Died 313.57 174.94 287.70 153.00 500.00 Mortality 0.387 Yes 313.57 174.94 287.70 153.00 500.00 No 311.45 422.58 203.50 29.00 2337.00CLEC-2, C-type lectin-like receptor 2; LAD, left anterior descending artery; LCX, left circumflex artery; OM, obtuse marginal branches; RCA, right circumflex artery; STEMI, ST elevation myocardial infarction.
Only three cases died due to arrhythmia; statistically, we could not discuss the predictive value of CLEC-2 regarding mortality. Follow-up was until discharge of patients, and all patients were discharged on medical treatment for follow-up in outpatient clinics apart from three mortality cases.
No statistically significant correlation (Spearman) between CLEC-2 serum level and age, low density lipoprotein level, cardiac enzymes levels and ejection fraction as shown in Table 5.
Table 5 - Spearman correlation coefficient of CLEC-2 serum level to age, LDL, cardiac enzymes level, and EF C-type lectin R P value N Age −0.026 0.859 50 LDL 0.197 0.171 50 CKMB 0.067 0.646 50 CK −0.047 0.745 50 Troponin 0.066 0.654 49 EF% −0.079 0.587 50 LAD% 0.002 0.989 43 RCA% 0.109 0.603 25 LCX% 0.250 0.334 17CLEC-2, C-type lectin-like receptor 2; CK, creatine kinase; CKMB, creatine kinase myocardial band; LAD, left anterior descending artery; LCX, left circumflex artery; LDL, low density lipoprotein; RCA, right circumflex artery.
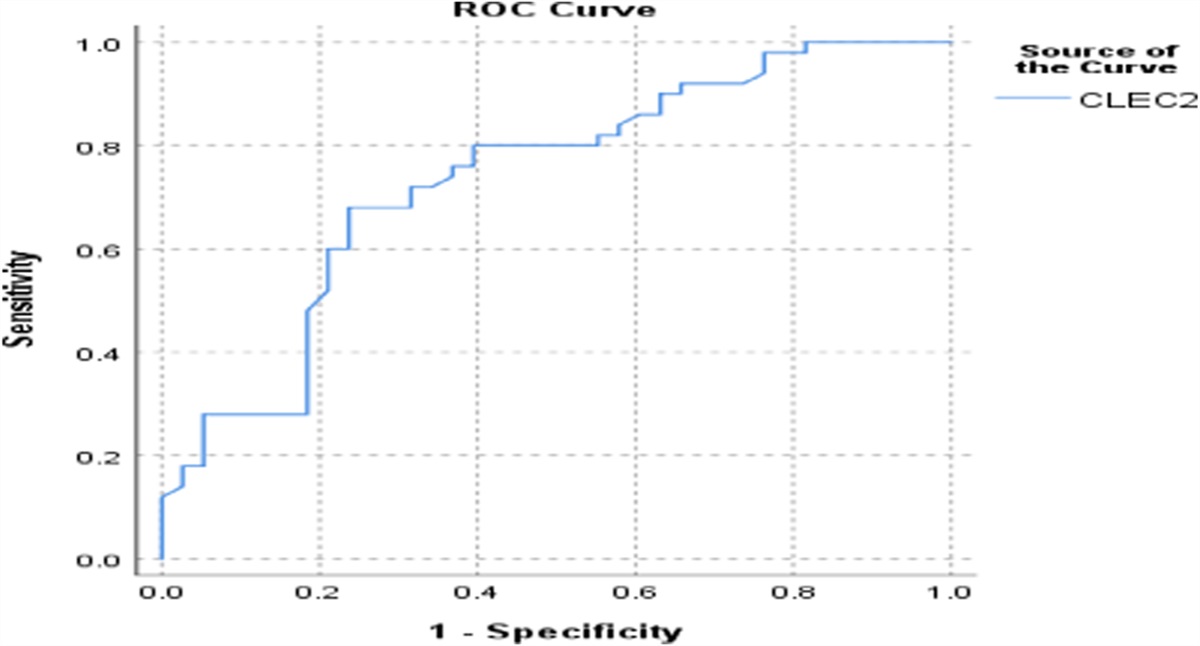
By using the ROC curve for determining the possibility of using CLEC-2 as a marker for STEMI, it showed that the best cutoff value is >121, area under the curve 0.73, sensitivity 76%, specificity 63.2% (P < 0.001), 95 CI (0.63–0.84) as shown in Figure 1.
 Figure 1.:
Figure 1.: ROC curve for the CLEC-2 as a marker for STEMI (sensitivity and specificity). CLEC-2, C-type lectin-like receptor 2; STEMI, ST elevation myocardial infarction.
4. DiscussionThis study included a total of 88 divided into 2 groups. Group I, is the cases group, includes 50 patients diagnosed with MI and group II includes 38 sex-matched and age-matched control healthy individuals. Regarding group I, there were 37 (74%) men and 13 (26%) women.
In this study, the male patients represented most cases by 74%. Male sex predominance is the result of biological and physiological differences in the cardiovascular system, which is a result of various genes expressed in sex chromosomes 15.
The CLEC-2 level in cases (MI) was higher than in controls, P value <0.001. Compared with the control group (median: 84.15 (1.5–500) pg/ml), the plasma levels of CLEC-2 were significantly high in acute coronary syndrome (median: 203.5 (29–2337) pg/mL). Min Fei et al obtained almost the same results in a study conducted on 216 Chinese patients with slight difference between levels of CLEC-2 in both groups between the two studies that may be due to ethnicity. Min Fei et al detected that CLEC-2 levels in blood were significantly increased in patients with acute coronary syndrome (134.16 [88.88–225.81] pg/mL) in comparison with the control group (65.69 (55.36–143.22) pg/mL).9
Akisato Nishigaki obtained the same results on a study conducted on 331 critical ill Japanese patients. sCLEC-2 levels were significantly higher in patients with atherosclerotic or lacunar ACI “acute cerebral infarction” or acute myocardial infarction in comparison with cardioembolic ACI or deep vein thrombosis.16
Yoshiki Yamashita et al observed that plasma CLEC-2 levels in patients with disseminated intravascular coagulation and thrombotic microangiopathy (TMA) were significantly higher (P < 0.001) than those in thrombocytopenic patients with other hematological diseases, but no significant differences in the plasma CLEC-2 levels were observed among patients with hemolytic uremic syndrome, thrombotic thrombocytopenic purpura, atypical hemolytic uremic syndrome, and other TMA in a study conducted on 58 Japanese patients with TMA.
留言 (0)