
記住我
Myocardial dysfunction is a serious complication in critically ill patients with sepsis and septic shock. It is considered one of the most complex organ dysfunctions in these patients because of its dynamic evolution due to the adaptation of the cardiovascular system to the disease process and resuscitation treatment.1 The incidence of diastolic dysfunction in patients with sepsis or septic shock is around 20%–56%.2,3 Studies showed strong correlation between diastolic dysfunction and mortality in these patients.4,5
However, there is a wide range of discrepancy involving which echocardiographic parameters are most predictive for poor outcome in these patients in addition to their cutoff values. The nature and complexity of critical illness along with preexisting comorbidities increases the number of confounding factors that (in part) explain the range of disparate findings across sepsis studies.
The primary aim of this study was to determine the impact of diastolic dysfunction on hospital mortality in patients admitted with sepsis. The secondary aim was to determine which echocardiographic diastolic parameters were most predictive of poor prognosis.
2. MethodsThis prospective study was conducted on 70 patients with clear evidence of sepsis and septic shock between March 1, 2019 and September 1, 2019. Data were collected from the critical care medicine departments of 2 academic medical centers after approval by each of the respective institutional ethical committees.
2.1 Inclusion CriteriaAll patients who had clear evidence of sepsis or septic shock were included. Sepsis was promptly identified at the bedside with qSOFA, that is, 2 or more of hypotension: SBP less than or equal to 100 mmHg; altered mental status (any GCS less than 15); and tachypnea: RR greater than or equal to 22 b/min. Septic shock was defined as a subset of sepsis in which, despite adequate volume resuscitation, both of persistent hypotension requiring vasopressors to maintain MAP greater than or equal to 65 mm Hg and lactate greater than or equal to 2 mmol/L were present.6
2.2. Exclusion CriteriaAny patient with any of the following were excluded: pregnant women, age 18 years and younger, significant mitral or aortic valve lesions, presence of regional wall motion abnormality or history of previous MI, and patients with poor echocardiographic window or poor image quality.
2.3. MethodologyOn admission, all patients had routine laboratory tests, including complete blood picture, kidney and liver functions tests, coagulation profile, C-reactive protein, arterial blood gases, and serum lactate. Lactate clearance was calculated 24 hours after admission. Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment scores were documented for all patients on admission. Blood cultures were withdrawn on admission before antibiotic therapy, and all patients were treated according to the fourth edition of Surviving Sepsis Campaign guidelines (2016), which were the latest at the time of the study. For all patients, vital signs were obtained at least hourly and both telemetry and peripheral capillary oxygen saturation were monitored continuously. Central venous pressure was measured on admission and hourly during the whole ICU stay.
2.4. Transthorathic EchocardiographyEither the echocardiography probe S4-2 of Philips HD7XE or the Siemens Acuson X300 PE ultrasound machine cardiac probe was used to collect the data. Parasternal long-axis standard 2D echocardiography, along with M-mode, was used to obtain standard heart chambers quantification and estimation of ejection fraction (EF) by the Teichholz formula.7 In an apical 4-chamber view, color Doppler was used on the mitral valve with M-mode to obtain the velocity of propagation. Pulsed wave Doppler was used to obtain mitral inflow patterns. Both E and A were recorded along with E/A ratio and E deceleration time, followed by IVRT after optimization of the signal. Tissue Doppler was used to obtain both septal and lateral E′, A′, and E/E′ ratio. Right ventricular function was assessed using TAPSE and maximum tricuspid regurgitation velocity.
Patients were stratified into 4 groups. Group 1 had only systolic dysfunction and normal diastolic function and EF ≤50%. Group 2 had only diastolic dysfunction and E′ ≤ 8 cm/sec. Group 3 included patients who had combined systolic and diastolic dysfunction, EF ≤50%, and E′ ≤ 8 cm/sec. Group 4 patients served as control because they had normal systolic and diastolic function, EF > 50%, and E′ > 8 cm/sec.
All clinical data during the hospital stay were recorded, including the use of vasopressors or inotropes, the need for renal replacement therapy (RRT), length of hospital stay, and in-hospital all-cause mortality.
2.5. Statistical AnalysisData were coded and entered using the Statistical Package for the Social Sciences (SPSS) version 25 (IBM Corp., Armonk, NY). Data were summarized using mean, standard deviation, median, minimum and maximum in quantitative data and using frequency (count) and relative frequency (percentage) for categorical data. Quantitative variables were compared using the nonparametric Kruskal-Wallis and Mann-Whitney tests. For comparing categorical data, the chi-square test was performed. The exact test was used instead when the expected frequency was less than 5. Correlations between quantitative variables were ascertained using the Spearman correlation coefficient. The ROC curve was constructed, with area under the curve analysis performed to detect the best cutoff value of significant parameters for detection of mortality. Logistic regression was used to detect independent predictors of mortality. P values less than 0.05 were considered as statistically significant.
3. ResultsThis study had 70 eligible patients, with all 70 included and none excluded. The mean ages of the studied patients were 63.93 ± 11.42, 59.33 ± 13.98, 63.42 ± 15.56, and 57.05 ± 16.81 years in the 4 groups, respectively, with no statistical significant difference. The general characteristics and the first 24 hours’ hemodynamic data of the studied patients are summarized in Tables 1 and 2, respectively.
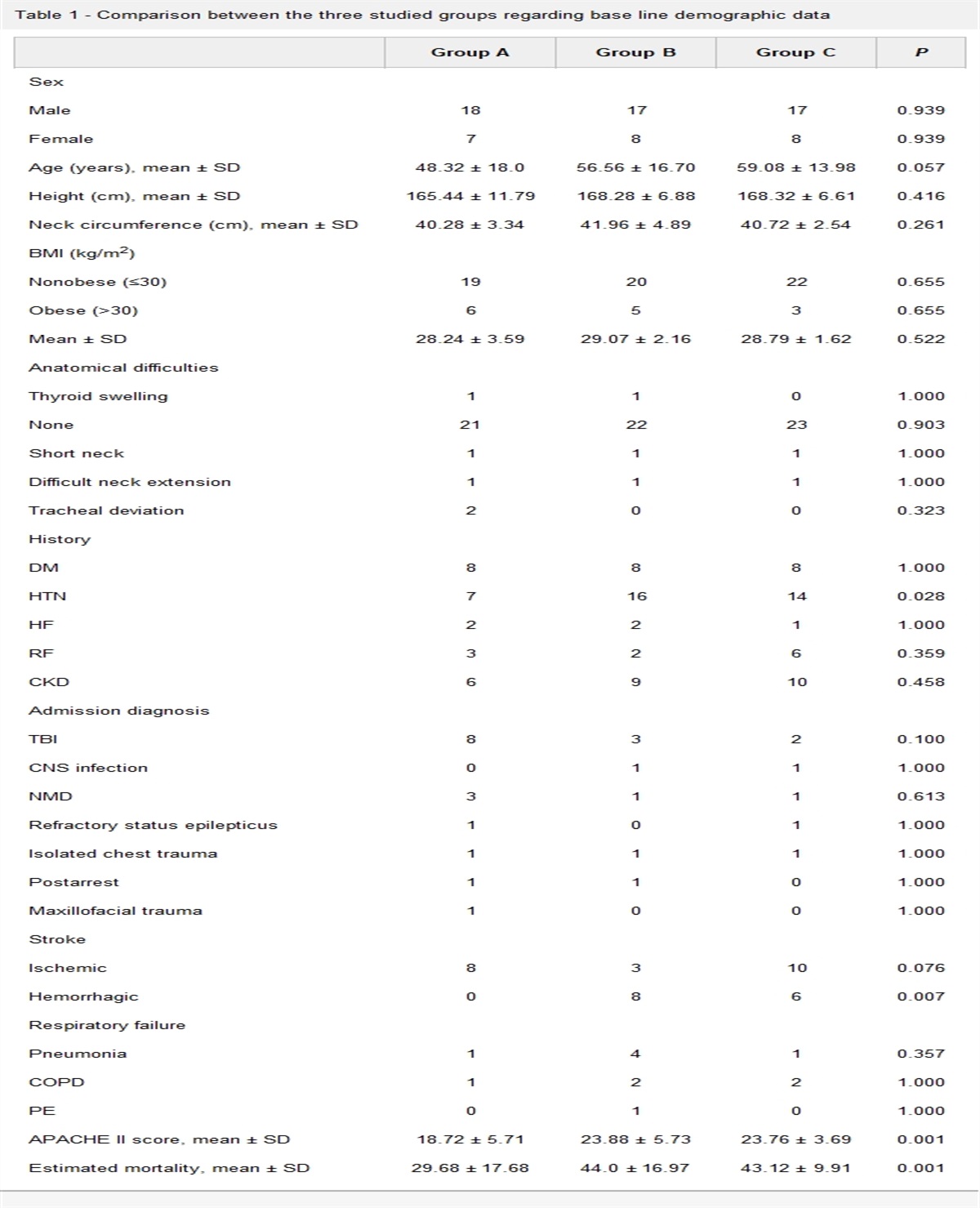
Table 1 - General characteristics of the studied patients Group G1 (n = 14) G2 (n = 18) G3 (n = 19) G4 (n = 19) P value Age 63.93 ± 11.42 59.33 ± 13.98 63.42 ± 15.56 57.05 ± 16.81 0.451 Sex Male 7 (50.0%) 10 (55.6%) 13 (68.4%) 3 (15.8%) 0.009 Female 7 (50.0%) 8 (44.4%) 6 (31.6%) 16 (84.2%) HTN 8 (57.1%) 12 (66.7%) 11 (57.9%) 7 (36.8%) 0.310 DM 8 (57.1%) 11 (61.1%) 15 (78.9%) 10 (52.6%) 0.365 IHD 6 (42.9%) 6 (33.3%) 17 (89.5%) 6 (31.6%) 0.001 +ve Blood culture 5 (35.7%) 9 (50.0%) 10 (52.6%) 12 (63.2%) 0.483 Lactate 5.18 ± 1.21 5.35 ± 1.15 5.71 ± 0.90 5.32 ± 1.27 0.681 CRP 187.07 ± 119.05 153.56 ± 108.76 165.91 ± 132.10 170.26 ± 98.92 0.810 APACHE II 20.79 ± 8.53 18.06 ± 9.77 23.05 ± 11.28 18.0 ± 7.82 0.456 SOFA 6.86 ± 3.39 7.0 ± 4.61 9.0 ± 5.72 5.84 ± 2.63 0.362 Shock 6 (42.9%) 5 (27.8%) 9 (47.4%) 4 (21.1%) 0.305Data are presented as mean ± SD or number (percentage %).
DM, diabetes mellitus; HTN, hypertension; IHD, ischemic heart disease; CRP, C-reactive protein; APACHE II, Acute Physiology and Chronic Health Evaluation; SOFA, Sequential Organ Failure Assessment.
Data are presented as mean ± SD.
CVP, central venous pressure; HR, heart rate; MAP, mean arterial blood pressure; SVR, systemic vascular resistance; SPO2, arterial saturation by pulse oximetry (SpO2).
As expected, statistical significant difference was found in the different studied groups regarding many of the diastolic function parameters, namely E, A, E/e′, septal e′, and lateral e′ (Table 3).
Table 3 - Different diastolic parameters in the studied groups G1 (n = 14) G2 (n = 18) G3 (n = 19) G4 (n = 19) P value Vel. of prop., (cm/s) 57 ± 26 51.7 ± 29 50 ± 22 68.5 ± 24 0.124 TR max velocity 233 ± 47 308.8 ± 62 339.8 ± 50 242.7 ± 65 0.001 E, (cm/s) 97.7 ± 20 73.2 ± 17 80 ± 17 97.7 ± 17 0.001 A, (cm/s) 73.4 ± 34 55.4 ± 35 48 ± 33 70 ± 39 0.029 E/A 1.6 ± 0.8 2 ± 1 2.3 ± 1.2 1.6 ± 0.6 0.301 E/e′ 8.6 ± 2.5 12 ± 3 13.2 ± 3 13.2 ± 3 0.001 E dt., (ms) 339.8 ± 63 148.9 ± 43.6 154 ± 51 152 ± 36 0.451 Sept. e′, (cm/s) 11.9 ± 2.8 6.3 ± 1.4 6.3 ± 1 10.4 ± 2 0.001 Sept. a′, (cm/s) 7.7 ± 2.6 8.5 ± 2 8.7 ± 3.1 8 ± 2 0.712 Lat. e′, (cm/s) 13.8 ± 3.7 8.5 ± 2 7.9 ± 2 12 ± 2.4 0.001 Lat. a′, (cm/s) 8.5 ± 3 9.3 ± 2 9.6 ± 3 9.8 ± 3 0.669Data are presented as mean ± SD.
Vel. of prop., velocity of propagation in cm per second; IVRT, isovolumetric relaxation time in milliseconds; E, E wave velocity in cm per second; A, A wave velocity in cm per second; E/A, E wave-to-A wave ratio; E/e′, E wave-to-E prime ratio; E dt, E wave deceleration time in milliseconds; Sept. e′, mitral annulus septal e′ velocity (septal e′) in cm per second; Sept. a′, mitral annulus septal a′ velocity in cm per second; Lat. e′, mitral annulus lateral e′ velocity in cm per second; Lat. a′, mitral annulus lateral a′ velocity in cm per second.
Regarding patients outcome, patients in group 3 were the worst. The mortality rate was 68.4% in group 3 while it was 7.1%, 61.1%, and 15.8% in group 1, 2, and 4, respectively (p<0.001). In addition, they had a higher incidence of developing acute kidney injury (AKI) with a subsequent need for RRT (p=0.008). Despite having a higher incidence of use of vasoactive agents, this finding was statistically insignificant. Length of ICU stay did not differ among the studied groups compared with the control group (10.71 ± 8.11, 6.72 ± 5.72, and 8.21 ± 4.6 versus 8.39 ± 6.4, respectively; P=0.24; Table 4).
Table 4 - Comparison between different studied groups regarding different outcome parameters G1 (n = 14) G2 (n = 18) G3 (n = 19) G4 (n=19) P value VA agents 6 (42.9%) 8 (44.4%) 10 (52.6%) 6 (31.6%) 0.623 RRT 4 (28.6%) 2 (11.1%) 7 (36.8%) 0 (0.0%) 0.008 LOS 10.7 ± 8.1 6.7 ± 5.7 8.2 ± 4.6 8.4 ± 6.4 0.248 Mortality 1 (7.1%) 11 (61.1%) 13 (68.4%) 3 (15.8%) <0.001Data are presented as mean ± SD or number (percentage %).
VA agents, vasoactive agents; RRT, renal replacement therapy; LOS, length of ICU stay.
Many of the diastolic dysfunction parameters were significantly different between survivors and nonsurvivors. However, using a multivariate regression analysis model that was applied among diastolic dysfunction parameters, only E/A ratio and septal e′ were independent risk factors of mortality, with odds ratios (ORs) 4.358 (P = 0.026) and 0.169 (P = 0.001), respectively (Tables 5 and 6).
Table 5 - Comparison between survivors and nonsurvivors regarding different diastolic parameters Died (n = 28) Survived (n = 42) P value Vel. of propagation 48.71 ± 20.76 62.43 ± 27.59 0.083 E/A 2.57 ± 1.23 1.52 ± 0.81 <0.001 E/e′ 13.10 ± 3.51 9.58 ± 2.21 <0.001 E deceleration time 149.18 ± 45.64 216.10 ± 371.66 0.250 TR max. vel. 310.39 ± 60.89 266.79 ± 73.69 0.008 Septal e′ 6.10 ± 1.46 10.15 ± 2.76 <0.001 Septal a′ 7.83 ± 2.74 8.52 ± 2.68 0.372 Lateral e′ 7.84 ± 1.94 12.23 ± 3.21 <0.001 Lateral a′ 8.67 ± 2.61 9.78 ± 3.05 0.134Data are presented as mean ± SD.
Vel. of prop., velocity of propagation in cm per second; E, E wave velocity in cm per second; A, A wave velocity in cm per second; E/A, E wave-to-A wave ratio; E/e′, E wave-to-E prime ratio; E dt, E wave deceleration time in milliseconds; TR max. vel., tricuspid regurge maximum velocity in cm per second; Sept. e′, mitral annulus septal e′ velocity (septal e') in cm per second; Sept. a′, mitral annulus septal a' velocity in cm per second; Lat. e′, mitral annulus lateral e′ velocity in cm per second; Lat. a′, mitral annulus lateral a′ velocity in cm per second.
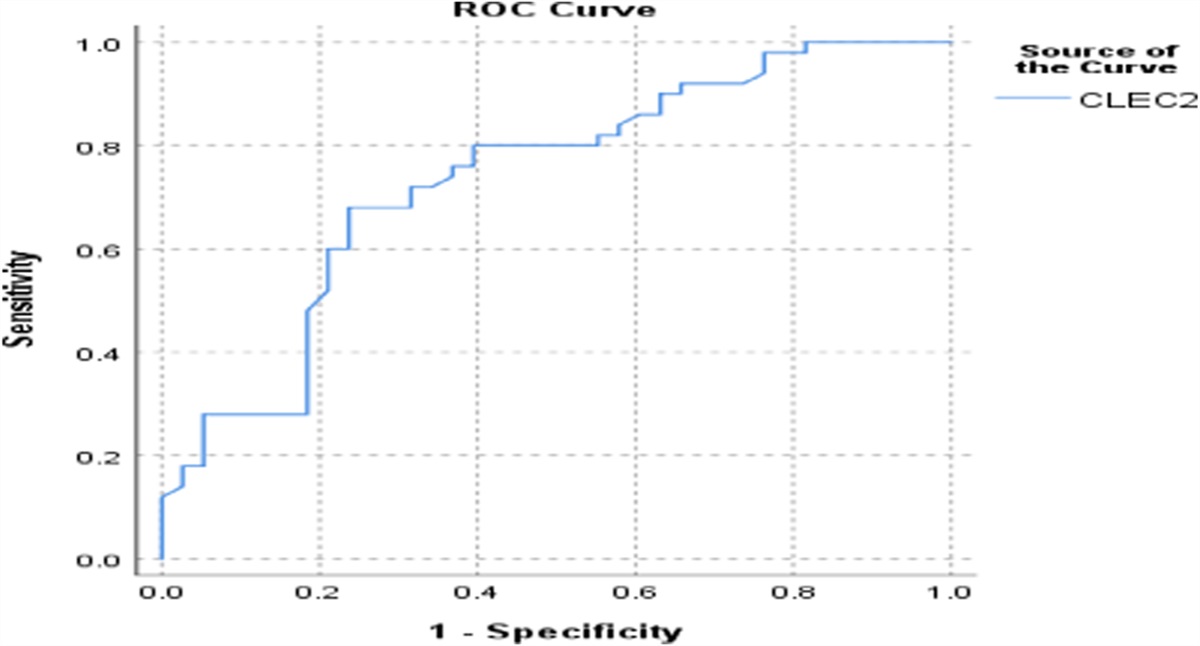
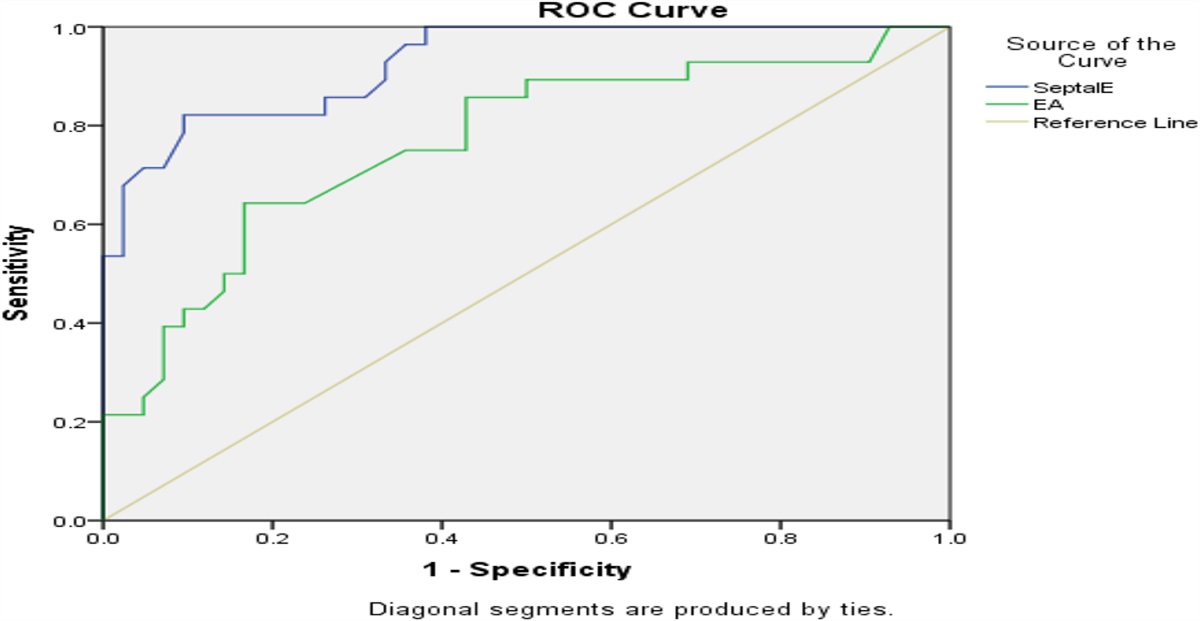
Using the receiver operator characteristics (ROC) curve, the cutoff values for E/A and septal e′ that predict mortality were 1.9 and 7.25 cm/sec., with areas under the curve (AUCs) 0.77 and 0.93, respectively (Figure 1).
 Figure 1.:
Figure 1.: Receiver-operating characteristic curve (ROC) for the detection of the cutoff value of E/A and septal e′ that predict mortality.
4. DiscussionThis study found that patients with sepsis and septic shock who had combined systolic and diastolic dysfunction had a higher incidence of mortality, with parameters such as E/A and e′ identified as independent predictors of mortality. It is good to mention that mitral annular early diastolic peak velocity (e′-wave) is known to be one of the most load-independent measures of diastolic dysfunction8,9 and is a known predictor of poor outcome in many cardiac diseases,10,11 which is in line with our study. Mean septal e′ was 6.10 ± 1.46 in nonsurvivors versus 10.15 ± 2.76 in survivors (P ≤ 0.001). Mean lateral e′ was 7.84 ± 1.94 in nonsurvivors versus 12.23 ± 3.21 in survivors (P ≤ 0.001).
Landesberg et al4 and Rolando et al12 found that diastolic dysfunction was associated with mortality in their cohorts. Another diastolic parameter, E/e′, was found to be an independent predictor of mortality in their study, which is in agreement with our study.
This may prove the deleterious effect of diastolic dysfunction in these patients. It may complicate hemodynamic management because of a poor clinical response to the fluid management.13 Fluid resuscitation is an important component of treating patients with septic shock; however, in patients with diastolic dysfunction and resultant decreased ventricular compliance, a positive fluid balance may aggravate pulmonary vascular congestion and edema, promoting pulmonary hypertension and hypoxemia.14
Mahjoub et al15 showed a significant increase in E/e′ after volume expansion in patients with sepsis-induced diastolic dysfunction and nonresponders to fluid challenge, which translates to an increase in left ventricular filling pressures, whereas patients with diastolic dysfunction and responders to fluid challenges showed an increase in e′ but not in E/e′, suggesting that left ventricular relaxation can be improved in preload-dependent patients. Many studies mentioned that septic patients with diastolic dysfunction should not be deprived of the standard therapy in early resuscitation,16–18 but its presence should alert the caregiver to have a more delicate approach during the resuscitation, making a continuous assessment of cardiovascular preload and response to volume expansion.19
This study also showed that patients with sepsis who had combined systolic and diastolic dysfunction were more associated with development of acute kidney injury with a subsequent need for RRT. To the best of our knowledge, the association of diastolic function and the need for RRT in septic patients with acute kidney injury has not been studied before; however, the effect of diastolic dysfunction is extensively studied in patients with chronic kidney disease, showing increased mortality and worse outcome.20
In this study, patients who had only systolic dysfunction had the lowest observed in-hospital mortality. This paradox was firstly described by Parker et al21 and Ognibene et al22 and confirmed later by Zanotti Cavazzoni et al.23 Explanation of why patients with sepsis-induced cardiomyopathy have better survival remains unclear; however, later studies noted that the reduced EF in the setting of septic shock may be reversible in patients who survive.24–26
In summary, this study supports the importance of diastolic function assessment in patients with sepsis and septic shock. Septic patients with diastolic dysfunction may have poor outcomes compared with other patients. Some diastolic function parameters could be used as a predictor of mortality in these patients. However, the small number of the studied patients may be the main limitation of this study. Our findings need to be reproduced in a study with a larger number of patients.
Research Quality and Ethics StatementThis study was approved by the institutional review board/ethics committee at the critical care department of Cairo University (approval date February 12, 2019).
References [1]. Suarez JC, Lopez P, Mancebo J, Zapata L. Diastolic dysfunction in critically ill patients. Med Intensiva. 2016;40(8):499-510. [2]. Bouhemad B, Nicolas-Robin A, Arbelot C, Arthaud M, Féger F, Rouby J-J. Isolated and reversible impairment of ventricular relaxation in patients with septic shock. Crit Care Med. 2008;36:766-774. [3]. Pulido JN, Afessa B, Masaki M, Yuasa T, Gillespie S, Herasevich V, et al. Clinical spectrum, frequency, and significance of myocardial dysfunction in severe sepsis and septic shock. Mayo Clin Proc. 2012;87:620-628. [4]. Landesberg G, Gilon D, Meroz Y, Georgieva M, Levin PD, Goodman S, et al. Diastolic dysfunction and mortality in severe sepsis and septic shock. Eur Heart J. 2012;33:895-903. [5]. Rolando G, Espinoza ED, Avid E, Welsh S, Del Pozo J, Vazquez AR, et al. Prognostic value of ventricular diastolic dysfunction in patients with severe sepsis and septic shock. Rev Bras Ter Intensiva. 2015;27(4):333-339. [6]. Singer M., Deutschman C. S., Seymour C. W., Shankar-Hari M., Annane D., Bauer M., et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801. [7]. Arora G., Morss A.M., Piazza G., et al. Differences in left ventricular ejection fraction using teichholz formula and volumetric methods by cmr: implications for patient stratification and selection of therapy. J Cardiovasc Magn Reson. 2010;12:P202. [8]. Nagueh SF, Sun H, Kopelen HA, Middleton KJ, Khoury DS. Hemodynamic determinants of the mitral annulus diastolic velocities by tissue Doppler. J Am Coll Cardiol. 2001;37:278–285. [9]. Kasner M, Westermann D, Steendijk P, Gaub R, Wilkenshoff U, Weitmann K, Hoffmann W, Poller W, Schultheiss HP, Pauschinger M, Tscho¨pe C. Utility of Doppler echocardiography and tissue Doppler imaging in the estimation of diastolic function in heart failure with normal ejection fraction: a comparative Doppler-conductance catheterization study. Circulation. 2007;116:637–647. [10]. Yu CM, Sanderson JE, Marwick TH, Oh JK. Tissue Doppler imaging a new prognosticator for cardiovascular diseases. J Am Coll Cardiol. 2007;49:1903–1914. [11]. Wang M, Yip GW, Wang AY, Zhang Y, Ho PY, Tse MK, Lam PK, Sanderson JE. Peak early diastolic mitral annulus velocity by tissue Doppler imaging adds independent and incremental prognostic value. J Am Coll Cardiol. 2003;41:820–826. [12]. Rolando G, Espinoza ED, Avid E, et al. Prognostic value of ventricular diastolic dysfunction in patients with severe sepsis and septic shock. Rev Bras Ter Intensiva. 2015;27(4):333-339. [13]. Boyd JH, Forbes J, Nakada TA, Walley KR, Russell JA. Fluid resuscitation in septic shock: a positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit Care Med. 2011;39:259-265. [14]. Sanfilippo F, Scolletta S, Morelli A, Vieillard-Baron A. Practical approach to diastolic dysfunction in light of the new guidelines and clinical applications in the operating room and in the intensive care. Annals of Intensive Care. 2018;8(1):100. https://doi.org/10.1186/s13613-018-0447-x [15]. Mahjoub Y, Benoit-Fallet H, Airapetian N, Lorne E, Levrard M, Seydi A-A, et al. Improvement of left ventricular relaxation as assessed by tissue Doppler imaging in fluid-responsive critically ill septic patients. Intensive Care Med. 2012;38:1461-1470. [16]. Mouncey PR, Osborn TM, Power GS, Harrison DA, Sadique MZ, Grieve RD, et al. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med. 2015;372:1301-1311. [17]. Peake SL, Delaney A, Bailey M, Bellomo R, Cameron PA, Cooper DJ, et al. Goal-directed resuscitation for patients with early septic shock. N Engl J Med. 2014;371:1496-1506. [18]. Yealy DM, Kellum JA, Huang DT, Barnato AE, Weissfeld LA, Pike F, et al. A randomized trial of protocol-based care for early septic shock. N Engl J Med. 2014;370:1683-1693. [19]. Sabatier C, Monge I, Maynar J, Ochagavia A. Assessment of cardiovascular preload and response to volume expansion. Med Intensiva. 2012;36:45-55. [20]. Han JH, Han JS, Kim EJ, Doh FM, Koo HM, Kim CH, et al. Diastolic dysfunction is an independent predictor of cardiovascular events in incident dialysis patients with preserved systolic function. PLoS ONE. 2015;10(3):e0118694. [21]. Parker MM, Shelhamer JH, Bacharach SL, Green MV, Natanson C, Frederick TM, Damske BA, Parrillo JE. Profound but reversible myocardial depression in patients with septic shock. Ann Intern Med. 1984;100:483–490. [22]. Ognibene FP, Parker MM, Natanson C, Shelhamer JH, Parrillo JE. Depressed left ventricular performance. Response to volume infusion in patients with sepsis and septic shock. Chest. 1988;93:903–910. [23]. Zanotti Cavazzoni SL, Guglielmi M, Parrillo JE, Walker T, Dellinger RP, Hollenberg SM. Ventricular dilation is associated with improved cardiovascular performance and survival in sepsis. Chest. 2010;138:848–855. [24]. Jardin F, Brun-Ney D, Auvert B, Beauchet A, Bourdarias JP. Sepsis-related cardiogenic shock. Crit Care Med. 1990;18:1055–1060. [25]. Vieillard-Baron A, Schmitt JM, Beauchet A, Augarde R, Prin S, Page B, Jardin F. Early preload adaptation in septic shock? A transesophageal echocardiographic study. Anesthesiology. 2001;94:400–406. [26]. Bouhemad B, Nicolas-Robin A, Arbelot C, Arthaud M, Fe´ger F, Rouby JJ. Acute left ventricular dilatation and shock-induced myocardial dysfunction. Crit Care Med. 2009;37:441–447.
留言 (0)