
記住我
In the state of New South Wales (NSW), Australia, there are about 4000 severe polytrauma hospital admissions per year, which are those defined as having an Injury Severity Score (ISS) of more than 12.1 About 50% of severe polytrauma patients sustain blunt chest injuries and about 12.5% will have a severe chest injury, defined as three or more rib fractures.1 Multiple rib fractures are associated with high mortality as well as high risk complications like pulmonary atelectasis, hospital-acquired pneumonia (HAP), respiratory failure, and lung contusions.2 In addition, multiple rib fractures increase both the Intensive Care Unit (ICU) and hospital length of stay (LOS), which leads to increased total healthcare costs.3 Flail chest segments are associated with worse outcomes and an even higher incidence of pulmonary morbidity.4 There is widespread acceptance of the recommended management of multiple rib fractures. This includes the use of aggressive pain management, respiratory support, physiotherapy, and surgical fixation of flail segments that cause respiratory failure that is severe enough to require mechanical ventilation.5,6
The use of multimodal analgesia that includes regional techniques with local anaesthetic is considered by many as the standard of care. It has been found to confer important benefits like decreasing pulmonary complications, shorten the duration of mechanical ventilation, and reducing mortality in rib fractures with or without flail segments.5 However, surgical fixation is not always available and the evidence about its benefits is mixed in multiple rib fractures without a flail chest.5,6
More and more, the use of bundles of care in ICU, such as ventilator-associated pneumonia (VAP) bundles and sepsis bundles, have become commonplace.7 They provide guidance in terms of what diagnostic procedures and treatment techniques when used together, yield better outcomes for patients.7 In blunt chest trauma with multiple rib fractures the application of a Chest Injury Protocol (ChIP) was associated with a decreased incidence of pneumonia of 56%.8 Bundles of care for severe polytrauma patients with rib fractures have been proposed, but evidence about their effectiveness is still being developed.9
This study aims to answer whether in adult severe polytrauma patients with multiple rib fractures, does the complete bundle of care made up of physiotherapy, respiratory support, regional analgesia, and surgical rib fixation when indicated improves patient-centred outcomes when compared to care that does not provide all of those elements as a bundle.
2 Materials and methodsThis is a single-center, retrospective, cohort observational study undertaken at John Hunter Hospital (JHH), a tertiary-referral, major trauma center, with an average 630 major trauma admissions per year.1
All severely injured patients with multiple rib fractures, with or without flail segments, who were admitted to the ICU at JHH between June 2014 and June 2019 were screened. The International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) Version for 2010,10 codes S22.3, S22.4, and S22.5, were used to select patients. Archived electronic medical files were reviewed by the authors. Approval from the local human research ethics committee was obtained before data collection began (AU201909-17).
The inclusion criteria were: (1) adult patients 18 years or older, (2) 3 or more rib fractures, and (3) non-penetrating chest trauma. The exclusion criteria were: (1) patients younger than 18 years of age, (2) non-traumatic rib fractures, and (3) pregnant patients.
The primary outcome was to describe the characteristics of severe polytrauma patients with multiple rib fractures and the treatment they received when admitted to the ICU of a major trauma center in Australia. The secondary outcomes were to compare the group that received a bundle of care made up of physiotherapy, respiratory support of any kind, regional analgesia techniques, and rib fixation to the group that received the incomplete bundle: either physiotherapy or respiratory support along with regional analgesia only, surgical rib fixation only, or neither. The decision to divide the groups based on whether they received the complete bundle or not is based on the recommendations from the Institute of Healthcare Improvement that states that elements of a bundle need to be delivered collectively and consistently and that eligible patients should receive all of the elements unless medically contraindicated.11
Comparisons were made to determine whether there were differences between: (1) the duration of invasive mechanical ventilation, (2) the hospital and ICU lengths of stay, (3) the incidence of pneumonia, defined as a deterioration of respiratory status after a period of stability on the invasive mechanical ventilator, evidence of infection or inflammation, and laboratory evidence of respiratory infection,12 and (4) the in-hospital mortality rate.
Data was collected on: demographics, mechanism of trauma, ISS at hospital admission, Acute Physiology and Chronic Health Evaluation-II (APACHE-II) at ICU admission, number of rib fractures, associated injuries, respiratory support requirements including invasive mechanical ventilation (IMV), non-invasive ventilation (NIV), High Flow Nasal Prongs (HFNP), regional pain management interventions including type and location, incidence of pneumonia, and management of rib fractures, whether surgical fixation or conservative. Data was collected from the hospital's Digital Medical Records (DMR) system.
Descriptive statistics are presented as percentages, with numerator and denominator in parenthesis. Data collected were considered non-parametric, and outcome measures were expressed as medians with interquartile ranges. Statistical analysis was performed using Prism 9 software. Mann-Whitney U test or Chi-square test were used for comparison between groups depending on the type of variables. Statistically significant differences are considered when P < .05.
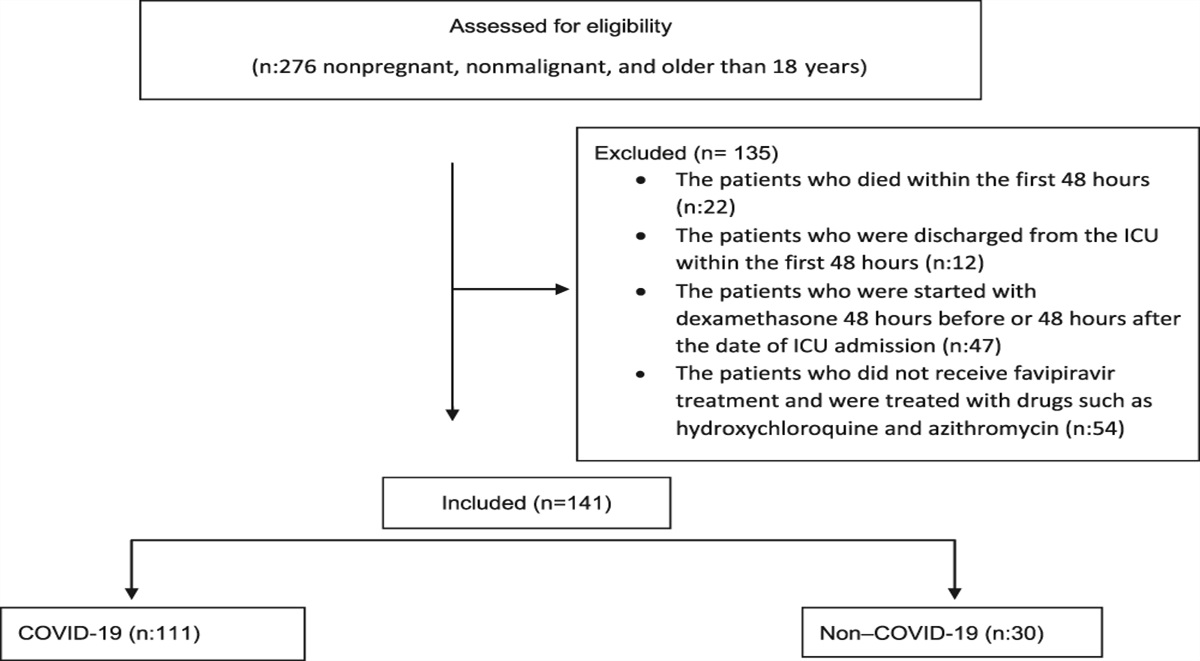
3 ResultsDuring the study period, between June 2014 and June 2019, there were 416 patients screened who were admitted to ICU with multiple rib fractures, and of these 322 patients were included in the analysis (Fig. 1).
 Figure 1:
Figure 1: Screening and analysis flowchart.
There was an average of 60 severe polytrauma with severe chest injury admissions to ICU per year. The most common causes of severe chest injuries with multiple rib fractures were traffic accidents with 69.5% (224/322) of the patients followed by falls 22.3% (72/322). The median age was 56years (IQR 18–94) and males made up 69.5% (224/322) of patients. The median APACHE-II score at ICU admission was 12 (IQR 2–35), the median ISS was 25 (IQR 4–75), and the median number of rib fractures was 6 (IQR 3–20). The in-hospital mortality rate was 10.6% (34/322), while the rate of pneumonia was 14.3% (46/322). The ICU readmission rate was 9% (30/322), tracheostomy rate was 5% (16/322), and one patient required ECMO. Detailed characteristics can be seen in Table 1.
Table 1 - Demographic characteristics and interventions Basic characteristic n = 322 Age: median (IQR) 56 (18–94) Male gender 69.5% (224/322) APACHE-II score: median (IQR) 12 (2–35) ISS score: median (IQR) 25 (4–75) GCS: median (IQR) 15 (3–15) Mechanism of trauma Traffic accident 69.5% (224/322) - Car 50.9% (164/322) - Motor bike 18.6% (60/322) Fall 22.4% (72/322) Assau t 1.5% (5/322) Others 6.5% (21/322) No. of rib fractures: median (IQR) 6 (3–20) Flail chest 34.8% (112/322) Flail chest that underwent ORIF 26.8% (30/112) IMV 52.8% (170/322) Duration of IMV, days: median (IQR) 1 (1–62) NIV 17.1% (55/322) HFNP 45.3% (146/322) Regional analgesia 44.1% (142/322) ORIF 11.8% (38/322) ORIF for flail chest 79% (30/38) Pneumonia 14.3% (46/322) Tracheostomy 5% (16/322) ICU LOS, days: median (IQR) 4 (1–65) Hospital LOS, days: median (IQR) 16 (1–248) In hospital mortality rate 10.6% (34/322) ICU readmission rate 9% (30/322)APACHE II, acute physiology and chronic health evaluation II; HFNP, High-flow nasal prongs; ICU, intensive care unit; IMV, invasive mechanical ventilation; IQR, interquartile range; ISS, injury severity score; N, number; NIV, non-invasive ventilation; ORIF, open reduction and internal fixation.
Pulmonary complications from chest injuries occurred in the majority of patients, the type and rates can be seen in Figures 2 and 3. Patients in the cohort admitted to ICU with polytrauma had a variety of extra-thoracic injuries, with spine fractures being the most frequent concomitant injury with a rate of 43% (141/322). The type and frequency of these injuries can be seen in Figure 4.
 Figure 2:
Figure 2: Pulmonary complications.
 Figure 3:
Figure 3: Type and rate of regional analgesia blocks.
 Figure 4:
Figure 4: type and rate of extra-thoracic injuries.
Patients were divided into 2 groups, one group of patients who received all the elements of the treatment bundle (Group 1) and the other group made up of patients who did not receive one or more of the elements of the treatment bundle (Group 2). There were statistically significant differences between the 2 groups in characteristics like the number of rib fractures, the rate of regional analgesia used, and the ICU LOS. Comparison between the 2 groups can be seen in Table 2.
Table 2 - comparison between the two groups Basic characteristics Group 1 (n = 32) Group 2 (n = 290) P –Age, years: median (IQR) 60.5 (21–80) 52.5 (18–91) .373 –Gender - Male 62.5% (20/32) 70.34% (204/290) .41 - Female 37.5% (12/32) 29.66% (86/290) –APACHE II: median (IQR) 13.5 (3–23) 11 (2–35) .308 –ISS score: median (IQR) 29 (9–48) 25 (4–75) .301 Rib fractures: median (IQR) 8.5 (3–20) 6 (3–19) .002 Thoracic epidural 18.8% (6/32) 5.5% (16/290) .014 Regional blocks other 81.3% (26/32) 40% (116/290) .0001 IMV 75% (24/32) 50% (146/290) .0088 NIV 21.8% (7/32) 16.5% (48/290) .458 HFNP 71.8% (23/32) 42.4% (123/290) .0023 Duration of IMV, days: median (IQR) 3.5 (0–54) 1 (0–62) .0063 Rib fixation 100% (32/32) 2.1% (6/290) <.0001 ICU LOS, days: median (IQR) 7 (1–57) 4 (1–65) .0045 Hospital LOS: IQR median (IQR) 16.5 (7–127) 15.5 (1–248) .20 Pneumonia 25% (8/32) 13.1% (38/290) .117 In hospital mortality rate 3.1% (1/32) 11.3% (33/290) .222APACHE II, acute physiology and chronic health evaluation II; HFNP, High-flow nasal prongs; ICU, intensive care unit; IMV, invasive mechanical ventilation; IQR, interquartile range; ISS, injury severity score; N, number; NIV, Non-invasive ventilation; ORIF, open reduction and internal fixation.
This study provides a reliable description of the characteristics, treatment received, and outcomes of severely injured patients with multiple rib fractures who were admitted to a tertiary-referral, major trauma ICU. As in other Australian reports, older middle-aged males involved in traffic collisions made up the majority of the patients in this cohort.1,13 The patients in this cohort had a very high ISS, with a median of 25. In some countries, an ISS of more than 16 is classified as major trauma and considered for ICU admission, but in Australia, an ISS of more than 12 is classified as major trauma.1 The patients in this cohort had a median ISS twice that. Regardless of where the cut-off is made, ISS correlates with morbidity and mortality, with higher scores leading to worse outcomes.14 Number of rib fractures also has been shown to correlate with higher mortality and morbidity in blunt chest trauma.15,16 According to some reports, odds ratios can be 1.19 and 1.16 for death and pneumonia respectively, for any additional rib fracture from trauma.15,17 In this study the median number of rib fractures was 6. Based on their ISS and number of rib fractures, the patients in this cohort would have been at a high risk of complications and in-hospital deaths, very likely higher than the 10% reported for the average ISS of between 18 and 20.5 from recent reports.1
In terms of treatment received by these patients, we can see how respiratory support was ubiquitous, with most patients receiving HFNP, or requiring on the first instance IMV. The rate of NIV use was the lowest of the 3 modalities. HFNP has been shown in some reports to be as effective as other forms of NIV in patients with blunt chest trauma, but does not decrease the rate of intubation when compared to NIV. Since HFNP is as effective while being better tolerated by patients it could be argued that this approach is adequate.18,19
In this cohort, we can see how the vast majority of patients received paravertebral blocks as the preferred mode of regional analgesia (Fig. 3), with a smaller number of patients receiving thoracic epidurals or serratus anterior blocks. Paravertebral blocks are emerging as a good approach for thoracic analgesia due to relative ease of administration when compared to thoracic epidurals, providing just as good analgesic cover to the affected areas as thoracic epidurals, and with fewer side effects20–22 (Fig. 3).
The in-hospital mortality rate in multiple rib fractures depends on patient age, the number of rib fractures, and concomitant injuries,17,23,24 in this cohort in-hospital mortality rate was 10%. this was similar to a report from American National Trauma Data Bank.15 Likewise, the incidence of pneumonia in multiple rib fractures depends on age and number of ribs fractured,15,23 and varies between 17% and 31% depends on patient age,5 we reported a pneumonia rate of 14.3%.
This data shows how rib fixation was reserved for only the most severely injured patients, with the highest numbers of rib fractures, and the highest severity scores. For the patients that underwent rib fixation, the median ISS was 29.5, median APACHE-II was 13.9, and the median number of rib fractures was 9 ribs. Of these, 79% (30/38) had a flail chest. Rib fixation has been recommended for patients with more than 5 rib fractures with flail segments, and can even be considered for patients with more than 3 rib fractures that are not requiring mechanical ventilation.25 In this cohort, the patients were much more severely injured than this, showing that the approach in the participating hospital is much more conservative. The component of the treatment bundle that was most often missing and kept patients from receiving the complete bundle was rib fixation. There were a few instances where patients did undergo rib fixation with no regional analgesia, but this did not occur often.
Despite their high initial risk for morbidity and mortality, the mortality rate was similar to the overall trauma death rate reported in Australia for patients that had a lower ISS and fewer fractured ribs, which is between 9% and 12.5%.1,13 The rate of pneumonia was also similar to that of Group 2, which had a lower risk profile.
When comparing patients in this cohort who received the complete bundle (Group 1) to those that did not receive the complete bundle (Group 2), although there was no statistically significant difference, the patients in Group 1 were slightly older and more severely injured. Variables with a statistically significant difference between these 2 groups included the number of rib fractures present, the likelihood of receiving regional analgesia, the likelihood of undergoing rib fixation, and the duration of IMV and ICU LOS. In general, the patients in Group 1 had higher severity of risk factors for morbidity and mortality than the patients in Group 2. The severity of risk factors for morbidity and mortality of Group 2 was similar to the overall cohort. We would expect the patients in Group 1 to have a higher rate of morbidity and mortality, particularly the incidence of pneumonia, but that was not the case. In this study, Group 1 and Group 2 had the same rate of pneumonia and in-hospital mortality. It would seem that it is possible to achieve the same mortality rate for severely injured polytrauma patients with multiple rib fractures to the overall trauma mortality rate by using a complete treatment bundle.
There was a statistically significant lower rate of regional analgesia and rib fixation provided to the patients that were in Group 2. This might be an area where gains could be made. Given the invasiveness of the procedure, it might be reasonable that rib fixation continues to be reserved for the most severely injured patients, but it might be possible to improve on the number of patients that received regional analgesia, particularly given that some techniques are less complicated to perform, are just as efficient, and are associated with fewer side effects.
The strengths of this trial are the inclusion of a large number of severely injured patients, which is quite specific and therefore provides a more detailed look at the characteristics and outcomes in this level of severity. This data is similar to previous reports, which would indicate that it is accurate and generalizable. The limitations of this trial are that it is a single-center study, retrospective, and observational trial, which makes it susceptible to the limitations of such. Also, because of it is an observational study, select bias is possible despite the best efforts to limit it.
5 ConclusionIn this high-volume, tertiary-referral major trauma center, severe polytrauma patients with chest injuries admitted to ICU have a high risk of morbidity and mortality. The use of a bundle of care was reserved for severely injured patients. It seems that when the complete bundle was administered to severely injured patients it was able to decrease their risk of complications and death to about the same as other less severely injured patients admitted to ICU. More research, prospective multicenter trial, is needed to help determine who would benefit the most from these interventions and which interventions are the most beneficial.
AcknowledgmentsAssistance with the study: none.
Financial support and sponsorship: none.
References [2]. Lin FC, Li RY, Tung YW, Jeng KC, Tsai SC. Morbidity, mortality, associated injuries, and management of traumatic rib fractures. J Chin Med Assoc 2016;79(6):329–334. [3]. Sirmali M, Turut H, Topcu S, et al. A comprehensive analysis of traumatic rib fractures: morbidity, mortality and management. Eur J Cardiothorac Surg 2003;24(1):133–138. [4]. Dehghan N, de Mestral C, McKee MD, Schemitsch EH, Nathens A. Flail chest injuries: a review of outcomes and treatment practices from the National Trauma Data Bank. J Trauma Acute Care Surg 2014;76(2):462–468. [5]. Witt CE, Bulger EM. Comprehensive approach to the management of the patient with multiple rib fractures: a review and introduction of a bundled rib fracture management protocol. Trauma Surg Acute Care Open 2017;2(1):e000064. [6]. Beks RB, Peek J, de Jong MB, et al. Fixation of flail chest or multiple rib fractures: Current evidence and how to proceed. A systematic review and meta-analysis. Eur J Trauma Emerg Surg 2019;45(4):631–644. [7]. Deborah LHMC. Care bundles in intensive care continuing education in anaesthesia. Crit Care Pain 2012;12(4):199–202. [8]. Curtis K, Asha SE, Unsworth A, Lam M, Goldsmith H, Langcake M, et al. ChIP: An early activation protocol for isolated blunt chest injury improves outcomes, a retrospective cohort study. Australas Emerg Nurs J 2016;19(3):127–132. [9]. Kourouche S, Buckley T, Munroe B, Curtis K. Development of a blunt chest injury care bundle: An integrative review. Injury 2018;49(6):1008–1023. [11]. Resar RGF, Haraden C, Nolan T. Using care bundles to improve health care quality. IHI innovation series white paper Cambridge. Massachusetts: Institute for Healthcare Improvement; 2012. [14]. Liman ST, Kuzucu A, Tastepe AI, Ulasan GN, Topcu S. Chest injury due to blunt trauma. Eur J Cardiothorac Surg 2003;23(3):374–378. [15]. Flagel BT, Luchette FA, Reed RL, et al. Half-a-dozen ribs: The break point for mortality. Surgery 2005;138(4):717–723. discussion 23-5. [16]. Battle CE, Hutchings H, Evans PA. Risk factors that predict mortality in patients with blunt chest wall trauma: A systematic review and meta-analysis. Injury 2012;43(1):8–17. [17]. Bulger EM, Arneson MA, Mock CN, Jurkovich GJ. Rib fractures in the elderly. J Trauma 2000;48(6):1040–1046. discussion 6–7. [18]. Halub ME, Spilman SK, Gaunt KA, et al. High-flow nasal cannula therapy for patients with blunt thoracic injury: A retrospective study. Can J Respir Ther 2016;52(4):110–113. [19]. Zhao H, Wang H, Sun F, Lyu S, An Y. High-flow nasal cannula oxygen therapy is superior to conventional oxygen therapy but not to noninvasive mechanical ventilation on intubation rate: A systematic review and meta-analysis. Crit Care 2017;21(1):184. [20]. Kim M, Moore JE. Chest trauma: Current recommendations for rib fractures, pneumothorax, and other injuries. Curr Anesthesiol Rep 2020;10(1):61–68. [21]. Yeung JH, Gates S, Naidu BV, Wilson MJ, Gao Smith F. Paravertebral block versus thoracic epidural for patients undergoing thoracotomy. Cochrane Database Syst Rev 2016;2:CD009121. [22]. Linda Le-Wendling JD, Allison Haller and Barys Ihnatsenka Analgesia for the Trunk: A Comparison of Epidural, Thoracic Paravertebral and Transversus Abdominis Plane Blocks. In: Noe GBRaCE, editor. Pain and Treatment 2014. 243–73. [23]. Kent R, Woods W, Bostrom O. Fatality risk and the presence of rib fractures. Ann Adv Automot Med 2008;52:73–82. [24]. Holcomb JB, McMullin NR, Kozar RA, et al. Morbidity from rib fractures increases after age 45. J Am Coll Surg 2003;196(4):549–555. [25]. de Moya M, Nirula R, Biffl W. Rib fixation: Who, what, when? Trauma Surg Acute Care Open 2017;2(1):e000059.
留言 (0)