
記住我



The study protocol was approved by the Swedish Ethics Review Authority (Dnr 2019–00450/1074–18) and was registered on ClinicalTrials.gov (reference number NCT04154371). This study follows the SCRIBE guideline reporting checklist [14].
Study designThis study used a single case experimental A-B-A design with multiple participants, enabling the evaluation of individual intervention effects over time, with each participant acting as their own control [15,16,17]. Single case experimental designs are recommended for investigating novel rehabilitation interventions in their early stages and serve as a preliminary assessment of intervention effect while also allowing refinement of the study protocol, inclusion criteria and/or outcome selection prior a larger trial [16,17,18].The study included a baseline phase (A1), an intervention phase (B), a post-intervention phase (A2), and a follow-up phase (FU). Phases A1 and A2 each consisted of 5 assessment sessions distributed over 2–3 weeks. The intervention phase included 18, 2 h sessions, 3 times a week for 6 weeks. During the intervention phase, assessments were performed approximately once a week. The follow-up sessions were planned 1 and 3 months after the post-intervention phase.
Moreover, during the final session of the intervention phase, all participants took part in a semi-structured interview to assess their perceptions and experiences of the intervention. The findings from the qualitative study are presented in a separate article [19].
ParticipantsA convenience sample was recruited through advertisements at rehabilitation centres, patient organizations, and support groups in the Gothenburg urban area. Inclusion criteria were: at least six months since the stroke onset, between 18 and 80 years old, severe or moderate impairment of the upper extremity (defined by a score ≤ 50 points on the Fugl-Meyer Assessment of Upper Extremity) [20], Modified Ashworth Scale score < 4 points on the 0–5 scale of elbow and wrist muscles [21], Montreal Cognitive Assessment score ≥ 22 points [22], detectable sEMG signal on the paretic arm, ability to communicate and follow instructions, and have the availability and transportation to follow the sessions protocol. Exclusion criteria were: open wounds, other non-stroke related complications that could influence the upper limb function, and uncorrected visual impairment. Informed written and oral consents were obtained from all participants prior to inclusion. All participants were allowed to continue with their ongoing activities, including their own home training. None of the participants had an ongoing therapy focusing on upper limb between the baseline and post-intervention phases.
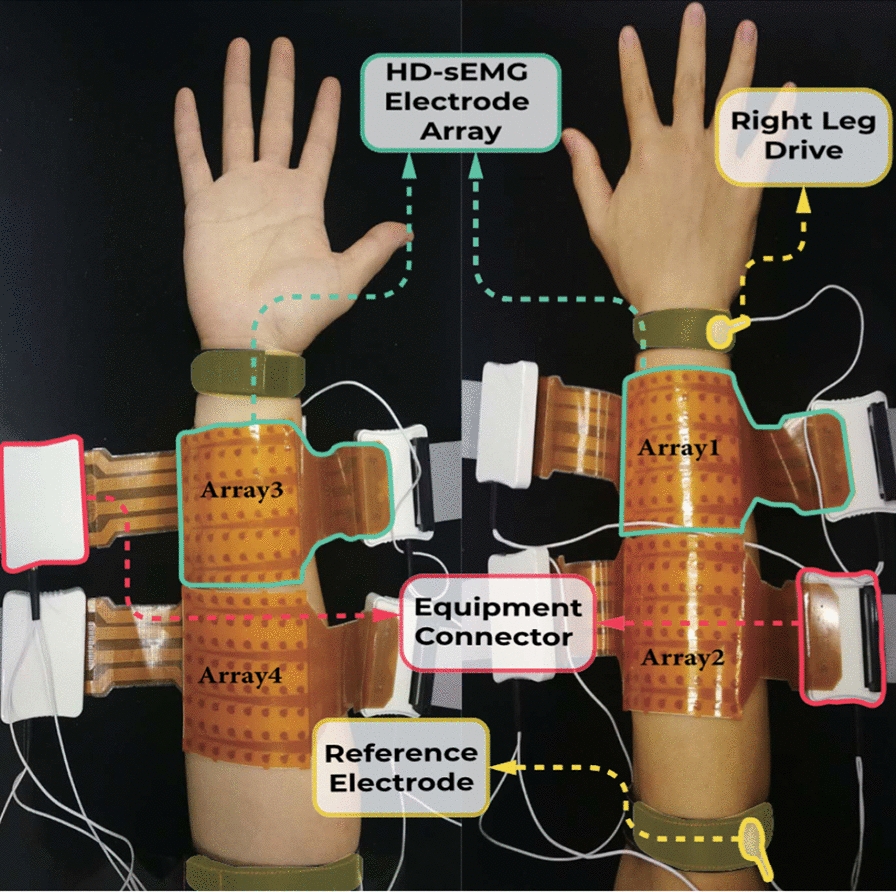
Intervention and proceduresThe intervention was provided by using an sEMG device with 8 bipolar channels capable of MPR (Neuromotus, Integrum AB, Sweden) [11, 12] The sEMG signals from the paretic arm were used to train the MPR algorithm, which decoded the user’s intention of movement to then control virtual environments during the training session (Fig. 1).
Fig. 1
Set-up of the system for a training session
Each intervention session involved: electrode placement, signal check and movement selection, initial sEMG recording, free control training, position match training, and gaming (Fig. 1). Disposable silver/silver-chloride (Ag/AgCl) surface electrodes were placed on the paretic arm's target muscles and connected to the sEMG recording device. The targeted muscles varied depending on the specific movement that was trained. For flexion and extension of the elbow and wrist, pronation and supination of the forearm, opening and closing of the hand, and flexion–extension of the thumb, the electrodes were placed on the midpoint of the muscle belly on the biceps, triceps, extensor and flexor carpi radialis and ulnaris, as well as the flexor and extensor digitorum, respectively. The sEMG signals from the target muscles were displayed on the computer screen, and the therapist verified if the participants could contract and relax the selected muscle groups and confirm the correct electrode placement. During the initial sEMG recording, the participants were instructed to perform three repetitions of each selected movement, with each repetition lasting 3 to 5 s of contraction and relaxation, respectively. The initial sEMG recording of each training session were used to train the MPR algorithm, in which each movement was associated with distinct muscle activation pattern performed by the participant. For the following steps of training a 75% or higher accuracy of MPR algorithm was required to control the system. In the free control training mode, the participants freely controlled a virtual arm to familiarize themselves with the selected movements. In the position match training mode, the participants had to match a random target posture of the virtual arm within a specified time frame with the completion rate percentage displayed at the end. In the game mode, participants controlled a car or a bar using the selected movements. The order of the training modes, number of repetitions of each step, and difficulty level varied depending on the participant's performance. Breaks were provided in all training sessions based on each participant's needs.
All sessions took place at Gothenburg University and were guided by a physiotherapist experienced with the training device (MMN). The therapist's role was to set up the system, select the exercises, supervise the synchronization between the training movements from the virtual environment and the paretic arm, and verbally guide the training. The therapist aimed to challenge participants, keeping them engaged at a difficulty level where they could still perform the required tasks, by gradually introducing more complex movements, advancing game levels, or extending training duration. To address challenges faced by some participants during specific movements, resistance was applied, a soft ball was used as an external reference for hand closing, or a towel was used to reduce friction between the forearm and the table during elbow flexion and extension. Moreover, participants were guided to focus on the virtual arm visualization on the computer screen instead of their physical arm.
AssessmentsAll assessments were conducted by an experienced physiotherapist otherwise not involved in the treatment sessions (MAM).
Motor functionThis study's primary outcome was motor function of the upper limb, assessed with the Fugl-Meyer Assessment of Upper Extremity (FMA-UE) [20]. The FMA-UE includes 33 items assessing the ability to perform voluntary shoulder, elbow, wrist, and hand movements within and outside synergies. Items are scored on a 3-point scale (0–2) and summed to a maximum score of 66, indicating the highest and best score. The minimal clinical important difference (MCID) in chronic stroke ranges from 4.25 to 7.25 points for the total FMA-UE score [23].
Activity capacityThe Action Research Arm Test (ARAT) was used to assess upper limb activity capacity. The ARAT includes 19 items that assess grasp, grip, pinch, and gross movements. Items are scored from 0 to 3, with a maximum score of 57 indicating full capacity. The MCID has been defined as 6 points change in the total ARAT score [24].
Grip strengthA hydraulic hand dynamometer (Sammons Preston Rolyan, IL, USA) was used to assess grip strength [25]. A mean of 3 trials in pound-force (lbf) was used as the test score. The MCID was 5.0 kg (11.1 lbf) and 6.2 kg (13.7 lbf) for the dominant and the non-dominant arm, respectively [26].
Kinematics analysis of the drinking taskUpper limb movement performance and movement quality were measured by kinematic analysis of the drinking task [27]. A 5-camera high-speed motion caption system (240 HZ, Qualisys AB, Sweden) collected 3D coordinates from 8 retroreflective circular markers placed on anatomical landmarks according to a standardized protocol. The task consisted of reaching, grasping, and lifting a cup filled with 100 mL of water located 30 cm from the edge of a table, taking a drink, releasing the cup, and returning to the starting position [27]. The participants were instructed to perform the drinking task at a comfortable self-paced speed, as naturally as possible, first with the non-paretic arm (not analyzed) and then with the paretic arm, collecting at least five successful trials for each arm. The data was analyzed using a custom-made Matlab script (R2022b, The Mathworks Inc).
The three kinematics variables, identified as key variables for stroke populations, were extracted for this study: movement time, movement smoothness, and trunk displacement [27, 28]. Movement time refers to the time required to complete the entire drinking task and starts when the hand movement begins (the hand marker velocity exceeded 2% of the peak velocity) and ends when the hand is back at the initial position [27]. The MCID has been defined as between 2.5 to 5 s [28]. Movement smoothness was measured as the number of movement units (NMU) during the four transport phases (reaching, forward and backward transport, and returning phases) [27]. One movement unit was defined as the difference between a local minimum and the next maximum velocity value that exceeds the amplitude limit of 20 mm/s, with at least 150 ms between subsequent peaks [27]. The minimum number of movement units for the drinking task is 4, with an estimated MCID between 3 to 7 units [28]. Trunk displacement was defined as the maximal forward displacement of the trunk marker in the sagittal plane during the entire task. The MCID ranges between 2 and 5 cm [28].
Active training timeThe time spent in the initial sEMG recording and the position match training were automatically saved in the training software, and the therapist manually recorded the approximate training time for the free control and the gaming modes. The average training duration of all sessions was calculated for each participant using the automatically and manually recorded training times.
Additional clinical assessments before and after trainingThe modified Ashworth scale was used to assess muscle tone during passive movements on a 6-point scale ranging from 0 (no increase in muscle tone) to 5 (rigid) [21]. The total score was calculated by summing elbow flexion/extension and wrist flexion/extension scores, with 20 being the highest score [21].
The non-motor domains of the FMA-UE were used to assess passive joint motion and joint pain [20]. Each domain has a maximum score of 24, indicating a normal passive range of motion and no pain.
Data analysisThe data of this A-B-A single case design study was evaluated by visual and statistical analysis [15, 16]. The visual analysis was conducted to evaluate data trends, stability, levels, variability, and overlap within and in between phases. Two authors (MMN and MAM) independently conducted the visual analysis and reached a consensus. Tau-U, which combines two non-parametric tests (Kendall's rank correlation test and Mann–Whitney U statistic), was used to quantify the magnitude of the intervention effect. Tau-U combines non-overlap between phases with intervention phase trends and corrects for baseline trend. Tau-U can adjust for the baseline trends and is applicable to ordinal data. The Tau-U summary index (A1 vs. A2 − trend A1) can be understood as an effect size coefficient, showing the proportion of the data that improves from baseline to post-intervention after adjusting for the baseline trend [29, 30]. The Tau-U calculator from College Station, Texas University (http://singlecaseresearch.org/) was used to analyze the A1 and A2 phases. The Tau-U effect sizes were interpreted as 0.00–0.25 (very low), 0.26–0.49 (low), 0.50–0.69 (moderate), 0.70–0.89 (large), and 0.90–1.00 (very large) [31]. The statistical significance level was set at p < 0.05. The statistical analysis excluded the follow-up phase due to inconsistent follow-up times and missing data.
To provide an overview of observed individual changes in relation to established MCIDs, a percentage of change (difference in median scores from baseline to post-intervention) was calculated. A value of 100% indicated that the change reached the established MCID.
留言 (0)