
記住我
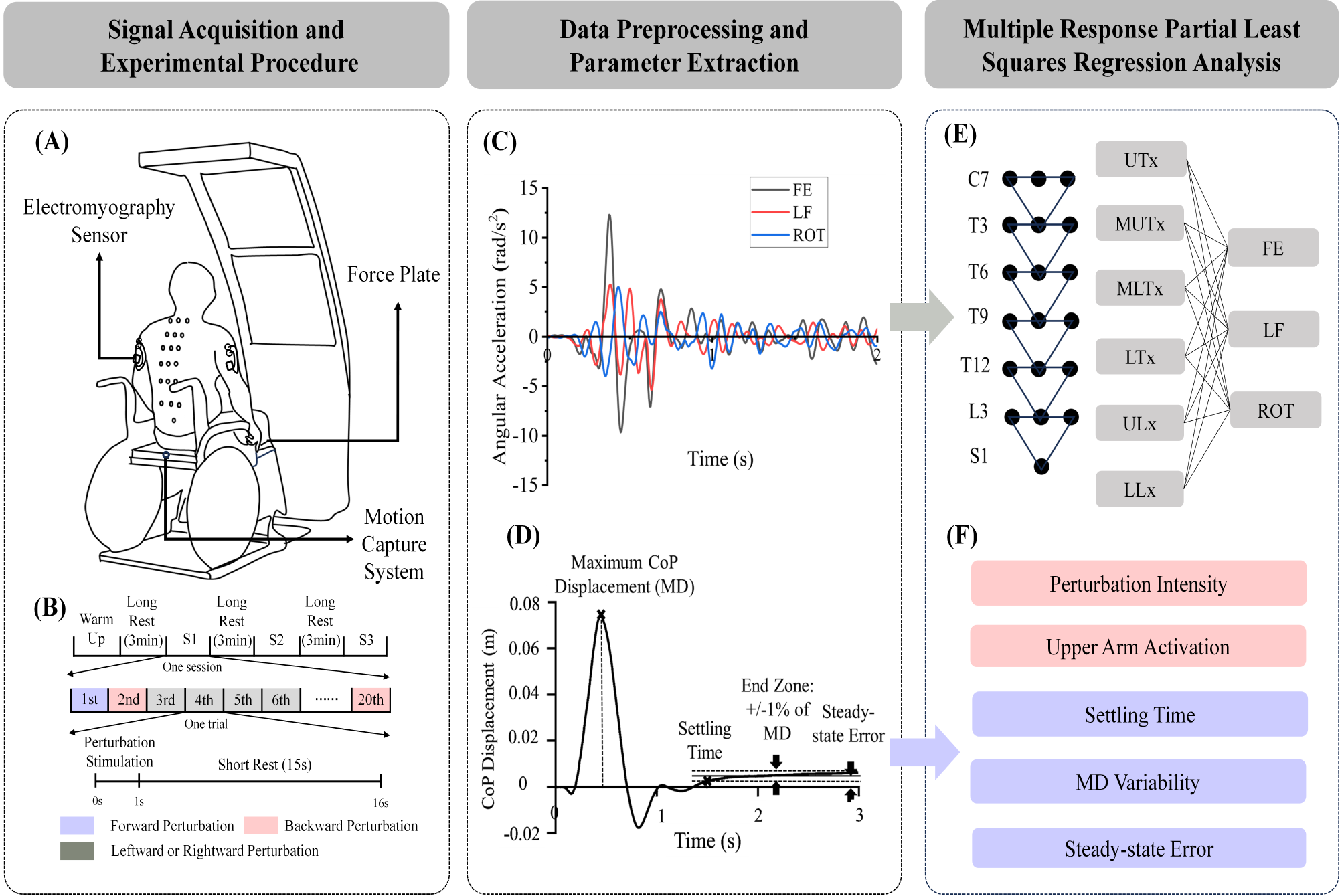

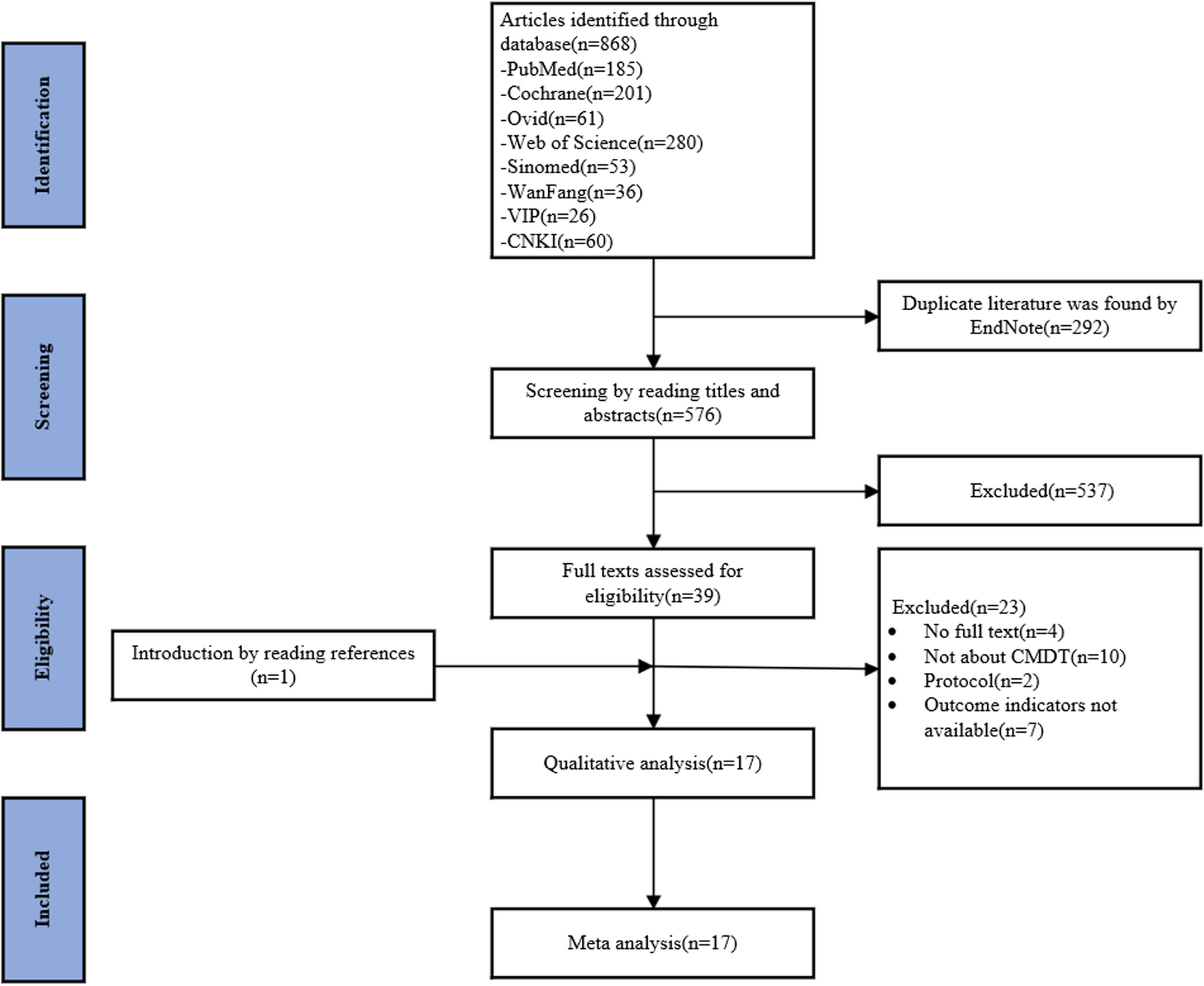
This double-blinded, parallel-group, randomized controlled trial was performed at a single rehabilitation hospital from August 2020 to December 2022. A computer-generated randomization table randomly allocated participants to the MI-contingent feedback BCI group or MI-independent feedback BCI group in a 1:1 ratio. The participants and assessors were blinded to the groups to which the participants were allocated. A CONSORT diagram is shown in Fig. 1. This study was approved by the Institutional Review Board of the Rehabilitation Hospital (NRC-2020-01-007) and registered at CRIS (KCT0009013). Participants provided informed consent before enrolment in the study.
Fig. 1
CONSORT flow diagram of participant recruitment
ParticipantsParticipants were recruited from a rehabilitation hospital, adhering to specific inclusion and exclusion criteria. Inclusion criteria comprised individuals who: (1) had hemiplegia due to a first-ever stroke with unilateral hemisphere lesions; (2) were in the chronic stage of stroke (≥ 6 months post-onset); (3) exhibited Medical Research Council (MRC) scale scores indicating affected wrist extensor muscle weakness (≤ 2); and (4) were aged > 19 years. Exclusion criteria included: (1) conditions hindering EEG signal recording, such as scalp wounds or metal implants; (2) wrist flexor spasticity rated ≥ 2 on the modified Ashworth scale (MAS); (3) cognitive impairments or aphasia affecting comprehension; (4) neurological or psychiatric disorders unrelated to stroke; (5) musculoskeletal issues or severe pain in the affected upper limb affecting intervention; (6) hemispatial neglect; and (7) uncontrolled medical conditions.
Given the lack of prior reports on the differential effects of MI-contingent feedback and MI-independent feedback with identical BCI systems, determining a precise sample size beforehand was unfeasible. Consequently, we set a sample size of 12 participants per arm, totaling 24, which met the minimum recommended sample size for pilot trials. To account for a potential attrition rate of 10%, we targeted 27 participants for this pilot study [11].
BCI-FES systemThe BCI system utilized in this study was the recoveriX-PRO, a non-invasive, neurofeedback-based stroke rehabilitation system. The recoveriX-PRO comprises an EEG, FES, and a computer screen projecting virtual hands. Sixteen channels (FC3, FCz, FC4, C5, C3, C1, Cz, C2, C4, C6, CP3, CP1, CPz, CP2, CP4, and Pz of the international 10–20 systems) of the EEG signal recording system were employed, sampling at 256 Hz and digitally filtered with a 0.5–30 Hz bandpass filter. The ground and reference electrodes were positioned over the forehead (FPz) and right earlobe, respectively. Spatial filtering was conducted using the common spatial pattern method to optimize variance for one MI category while minimizing it for the other. Subsequently, the spatially filtered data underwent classification through linear discriminant analysis. A comprehensive description of the signal processing methods can be found elsewhere [6].
One pair of FES electrodes was positioned on the skin over both forearms’ wrist extensors. The frequency of the FES devices (g.Estim FES, g.tec Medical Engineering GmbH, Austria) was set at 50 Hz, with a rectangular pulse width of 300 µs. The current amplitude was adjusted individually to ensure contraction of the affected wrist extensor without causing discomfort. Visual feedback was provided in the form of an embodied representation, where the bilateral forearms and hands of a virtual avatar were displayed on a monitor. The recoveriX-PRO system seamlessly acquired, analyzed, and interpreted EEG signals associated with MI. It then activated the FES system when the participant imagined movement on the instructed side (Fig. 2). Utilizing the recoveriX-PRO system involves integrating cortical and peripheral activities, thereby establishing a closed loop between brain signals during imagined movements and contingent visual and proprioceptive feedback. This process aids patients in learning to imagine or execute desired movements effectively.
Fig. 2
The recoveriX PRO training system
BCI interventionThe recoveriX-PRO interventions consisted of 240 trials of MI tasks involving both hands, divided into three runs of 80 trials each (refer to Fig. 3). Each run comprised two sets of 40 trials, separated by a 2-min break. An additional 3–5 min were allotted for the inter-run break. A trial commenced with an attention beep at 0 s. Subsequently, at 2 s, an arrow indicating the hand (“left” or “right”) for which MI was expected appeared on the monitor, accompanied by verbal instructions. Participants were instructed to imagine wrist dorsiflexion according to the system’s instruction, which alternated between “left” and “right” in a semi-random order. During the feedback phase (from 3.5 s to 8 s), FES and the virtual avatar were activated. The recoveriX-PRO interventions encompass two types of runs: calibration and rehabilitation runs. In the rehabilitation run, feedback was triggered only when the BCI system detected MI of the correct hand (MI-contingent feedback). Conversely, in the calibration run, feedback was consistently activated, irrespective of MI (MI-independent feedback). The feedback was updated at a rate of five times per second.
At 8 s, a relaxation signal indicated the end of the task period (MI), which lasted 6 s. The interval between trials varied randomly within a range of 1 s.
All participants underwent 20 sessions of 60-min BCI intervention, administered by research physical therapists, 5 days a week over 4 weeks. The BCI intervention session comprised one calibration run followed by two rehabilitation runs, where participants received MI-contingent feedback-based BCI intervention (Fig. 3A). In contrast, the MI-independent feedback group intervention session involved three consecutive calibration runs without any rehabilitation runs, providing participants with MI-independent feedback irrespective of their MI (Fig. 3B). Patients in the MI-independent feedback group used the same hardware, followed the same task instructions, and performed the same MI task of extending the affected wrist as those in the BCI group. Both groups had the same setup, with interventions starting based on the initial Calibration MI. The MI-contingent feedback group received FES only if it matched the Calibration MI, while the MI-independent feedback group received FES regardless of MI. Participants performed the MI task while seated, wearing the EEG cap, and observing the virtual avatar’s forearm and hand on a screen. The intervention and assessments were conducted in a dedicated, tranquil research room to facilitate task concentration. Additionally, all participants received 30 min of conventional therapy for the affected upper limb 5 days a week.
Fig. 3
The recoveriX PRO session
Outcome assessmentClinical and neurophysiological outcomes were evaluated by an independent team comprising a research physical therapist and a physiatrist who were blinded to the group allocation. Clinical assessments were conducted at baseline (W0), after 2 weeks (W2), and at the end of the 4-week intervention period (W4), while neurophysiological outcomes were recorded at W0 and W4.
Clinical outcomesWe assessed baseline demographics of participants, including sex, age, stroke type, hemiparetic side, and time since stroke onset. Our evaluation aimed to cover all domains of upper limb function outlined in the International Classification of Functioning, Disability, and Health (ICF): impairment, activity, and participation. For body function/structure, we recorded outcomes such as the MRC scale for muscle strength in the wrist extensor (MRC-WE; scored 0–5), active range of motion in wrist extension (AROM-WE), and MAS for wrist flexor spasticity (MAS-WF; scored 0–4), along with the FMA. Activity and participation were assessed using the Box and Block Test (BBT) and the Stroke Impact Scale (SIS), respectively [12]. The primary outcome was changes in the MRC-WE and AROM-WE at W4, the targeted outcomes of our intervention.
The FMA tool is used to evaluate motor performance in persons with stroke, with higher scores indicating better motor function [13, 14]. We examined four specific FMA variables: FMA-total (0–66), FMA-distal (0–24), FMA-wrist (0–10), and FMA-hand (0–14). The BBT measures gross manual dexterity by counting the number of blocks an individual can transfer between sections within one minute. To assess health-related quality of life (HRQoL), we utilized version 3.0 of the SIS, a self-reported questionnaire tailored for persons with stroke. We focused on SIS domains relevant to upper limb function: hand function, physical and instrumental activities of daily living (ADLs/IADLs), and social participation [15, 16]. MI accuracy is an indicator of how well a participant is adapting to a BCI system. Each participant underwent 20 sessions, and MI accuracy was recorded in each session. The mean MI accuracy over the 20 sessions was then calculated to determine the mean MI accuracy for each group.
Resting-state EEG measurementsResting-state EEG data were collected to assess changes in functional connectivity in the motor area pre- and post-intervention. EEG recordings took place during separate sessions at W0 and W4. Participants were seated comfortably and instructed to relax without focusing on any particular thoughts. Data were recorded at a sampling frequency of 256 Hz using a 32-channel g. nautilus system (g.tec Medical Engineering GmbH, Austria). The 32 electrodes were distributed across the scalp based on the extended 10–20 international system using an elastic electrode cap, with the reference channel positioned on the right earlobe of each participant. We acquired EEG from participants with their eyes closed and open at rest for 5 min twice, respectively, totaling 20 min of resting-state data.
Functional connectivity analysis using resting-state EEGTo analyze the changes in functional connectivity in the motor area before and after the intervention, the eyes-closed resting-state EEG data was first preprocessed as follows: The raw EEG data were bandpass-filtered using a 3rd-order Butterworth filter with cutoff frequencies of 1 and 50 Hz, and then segmented into 1-s epochs without overlaps [17]. Epochs containing significant artifacts exceeding a ± 120 µV signal threshold were removed, and 30 artifact-free epochs were randomly selected for each participant. Among the 25 participants, one participant’s data from the MI-independent BCI group was excluded due to insufficient artifact-free epochs (< 30). Thus, pre-processed EEG data from 24 patients (MI-contingent feedback BCI group = 12, MI-independent feedback BCI group = 12) were utilized for functional connectivity analysis. EEG channels were inverted for individuals with right-hemisphere lesions to ensure consistent data analysis across patients, aligning the lesion consistently over the left hemisphere in all the participants. For example, electrode C3* was assigned to cover the affected hemisphere, while electrode C4* was designated for the unaffected hemisphere. Partial directed coherence (PDC) [18] is a statistical measure used to determine the direction and strength of interactions between time series in the frequency domain, particularly in the context of neural data analysis such as EEG. PDC is derived from multivariate autoregressive (MVAR) models, which allows it to identify the direct influence of one variable on another while controlling for the effect of all other variables in the system. In this study, Partial directed coherence (PDC), a representative, effective functional connectivity measure, was employed to assess changes in directed functional connectivity pre- and post-intervention [9, 19]. PDC was calculated for each of the 30 pre-processed EEG epochs using a 6th-order multivariate autoregressive model implemented in the Hermes Matlab toolbox [20]. The µ (10–12 Hz) and β (18–24 Hz) bands, which are the frequencies most relevant to motor control. were used for PDC calculation [21]. Subsequently, PDC values were normalized to the range of 0–1 and averaged across all 30 epochs for each participant.
Transcranial magnetic stimulation (TMS)-induced motor evoked potential (MEP)Cortical excitability was measured using a TMS (MagPro stimulator, MagVenture, Lucernemarken, Denmark) at W0 and W4. Participants were seated comfortably in a reclining armchair with their hands pronated on a cushion. We used a figure-of-8 coil to stimulate the motor cortex with the coil handle oriented 45° posterior to the midline to ensure the electromagnetic current flowed perpendicularly to the central sulcus [22]. Electromyographic signals were recorded using an active surface electrode placed on the contralateral first dorsal interosseous muscle, while reference and ground electrodes were positioned on the index finger proximal interphalangeal joint and over the wrist, respectively. The optimal scalp location (hotspot) was determined as the site eliciting the largest MEP amplitude with the lowest stimulation intensity [23].
We examined cortical excitability using MEPs and resting motor threshold (RMT). The RMT (%) was the lowest stimulator intensity that could elicit MEPs with an amplitude of at least 50 microvolts in at least five out of 10 consecutive trials [23]. MEP amplitude was evaluated at 120% of the TMS intensity necessary to elicit RMT, and we measured the average peak-to-peak amplitudes of MEP from 10 consecutive MEP sweeps.
Statistical analysisWe employed a linear mixed model analysis for repeated measurements to compare intervention effects within and between groups across all time points. The statistical model included the outcomes as the dependent variable, with group (between-subject factor; MI-contingent feedback BCI or MI-independent feedback BCI), time (within-subject factor), group × time interactions, and baseline value of the outcome as fixed effects. Each participant’s intercept was considered a random intercept in the model. Group × time interactions were utilized to estimate intervention effects at all time points, while within-group time effects were assessed in each group. Results are presented as actual values and mean adjusted differences in outcomes between the two groups, with 95% confidence intervals (CI). Additionally, we examined correlations between primary outcomes (MRC-WE and AROM-WE) and PDC from premotor to motor in the µ and β frequency bands using repeated measures correlation (rmcorr) to identify linear relationships in paired data collected through repeated measurements. The analysis employed R version 4.3.2 (http://www.r-project.org) using the lme4 and rmcorr package [24, 25]. MEP data were not statistically analyzed because MEP was observed in only five participants.
留言 (0)