In clinical solid organ transplantation, strategies that achieve long-term immunosuppression-free graft survival without the need for intense myeloablative conditioning remain elusive. In this issue of Cell Research, Liu et al. report that in murine transplant model, central deletional tolerance achieved by transduction of donor MHC alloantigen expression on the recipient thymus results in long-term skin allograft survival.
Since the introduction of ciclosporin in the 1970s made transplantation a clinical reality, massive advances have been made, and kidney transplants from deceased donors are now expected to last between 15 and 20 years. However, for the majority, graft survival is still dependent upon continual administration of immunosuppression. This confers heightened risks of infection and cancer development, and even then, eventual graft loss is generally considered a consequence of adaptive immune recognition of mismatched alloantigen.
Despite the initial enthusiasm that the ‘Holy Grail’ of transplantation — transplant tolerance without requirement for immunosuppression1 would be unearthed within a few short years, it has remained fittingly elusive, with the term still used reverently today.2 Immunosuppression-free solid organ allograft survival has been achieved in small numbers of select recipient, but generally requires aggressive myeloablative conditioning and creation of a haematological chimeric state by reconstitution with haemopoietic stem cell transplantation from the same donor as the solid organ transplant.3 Such conditioning carries substantial morbidity, and thus has not been widely adopted.
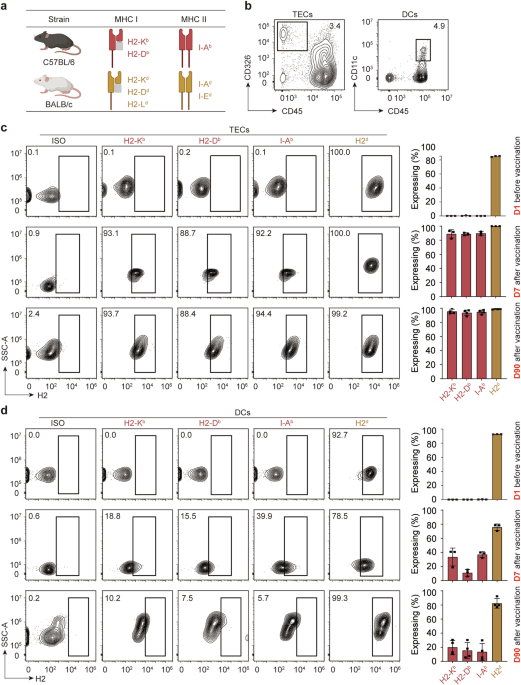
Transplant tolerance achieved via a chimeric state likely depends upon central deletion,4 wherein developing T cells that recognize MHC alloantigen in the thymus with sufficient avidity are deleted, leaving a hole in the clonal repertoire that enables transplant engraftment without rejection. In this issue of Cell Research, Liu and colleagues report a different approach in a murine transplant model to achieve central deletion against donor MHC alloantigen, by using adeno-associated viral constructs to transduce expression of mismatched donor MHC alloantigen on recipient thymic epithelial cells, a technique they termed donor MHC-specific thymus vaccination (DMTV).5 Donor strain skin allografts transplanted two months later did not provoke alloantibody responses in the recipient and survived long term.
Tolerogenic strategies centered on thymic expression of alloantigen are not novel; indeed, intrathymic injection of either alloantigenic cells or cDNA encoding MHC heavy chain was a major focus of early transplant research, principally using rat transplant models, in the early 1990s.6 Notably, in a ‘low-responder’ donor-recipient strain combination, intrathymic injection of plasmid cDNA encoding the α chain of the donor MHC class I alloantigen resulted in prolonged liver allograft survival, although a single simultaneous administration of anti-lymphocyte serum was also required.7 Conventional cytotoxic T lymphocyte limiting dilution analyses suggested deletion of the alloreactive T cell clones as the principal mechanism responsible for avoidance of early rejection.
This begs the question of how much the study by Liu and colleagues advances our understanding of transplant tolerance and whether it takes us closer to realizing the early vision of long-term transplant survival in the absence of immunosuppression. Liu and colleague’s work undoubtedly provides a more in-depth analysis of the mechanisms responsible for operational tolerance to the graft, with T cell clonal analysis confirming deletion of the alloreactive T cell repertoire. The authors also detail for the first time the potential effectiveness of this approach in humans, by using humanized mice to demonstrate survival and multilineage expression of third-party human embryonic stem cells, provided that the recipients had also been inoculated with fetal thymic tissue that had been transduced with viral vectors encoding the donor strain HLA antigens.
Liu and colleagues further show that intrathymic transduction of donor MHC antigen could achieve long-term graft survival without a requirement for adjuvant T cell depletion, by simply delaying challenge with the skin allograft for several months, by which time the peripheral T cell repertoire had been replenished according to the modified thymic environment. Whether such an approach would be effective in humans is debatable. The murine experiments were performed using naïve recipient mice kept in specific pathogen-free conditions, whereas in human adult transplant recipients, the alloreactive T cell population consists largely of memory cells that have arisen earlier from cross-reactive ‘heterologous’ immunity.8 Clonal persistence9 will likely maintain these memory populations independent of ongoing thymic output. Hence, aside from the practical difficulties posed by thymic involution in adulthood, it is likely that some form of T cell ablation would also be required in humans to delete existing memory against non-self HLA, and allow repopulation according to the new thymic landscape. Liu et al. also show that DMTV was effective in recipients previously sensitized against the donor, but additional total body irradiation and T cell depletion of the recipient was required to achieve skin graft survival.
Liu and colleagues expressed all the mismatched donor MHC class I and class II alloantigens in the recipient thymus, to ensure deletion of all developing T lymphocytes with reactivity against donor MHC. This approach was presumably thought necessary because in contrast to peripheral tolerance, central deletional tolerance would not trigger the ‘linked epitope suppression’10 necessary for actively inhibiting otherwise aggressive responses against additional graft alloantigen not transduced on the recipient’s thymus. This requirement for expression of all mismatched donor MHC antigens limits the potential for clinical translation, because it would require advance knowledge of the detailed HLA genotype, and this would only be an option for living donor transplantation.
Perhaps the most straightforward initial clinical application would be to use DMTV to achieve deletional tolerance in the recipient against specific non-self MHC antigens that are commonly expressed in the donor pool. Kidney transplant outcomes are influenced by the degree of HLA mismatch between donor and recipient, and although the impact of this mismatch has lessened with the use of modern immunosuppression, such an approach may improve long-term transplant outcomes and thus reduce the proportion of patients active on the waiting list who have already received a transplant, currently ~20%. Such a strategy may provide the additional benefit of limiting germinal center humoral alloimmune responses. These can result in production of durable and high-affinity, class-switched donor-specific alloantibody, that can develop either during transplant follow-up or after the graft has failed and immunosuppression is tapered. Such ‘sensitization’ is one of the main barriers to a transplant, and for individuals ‘highly’ sensitized against multiple class I and class II HLA antigens found in the donor pool, may probibit their chance of transplantation altogether.

留言 (0)