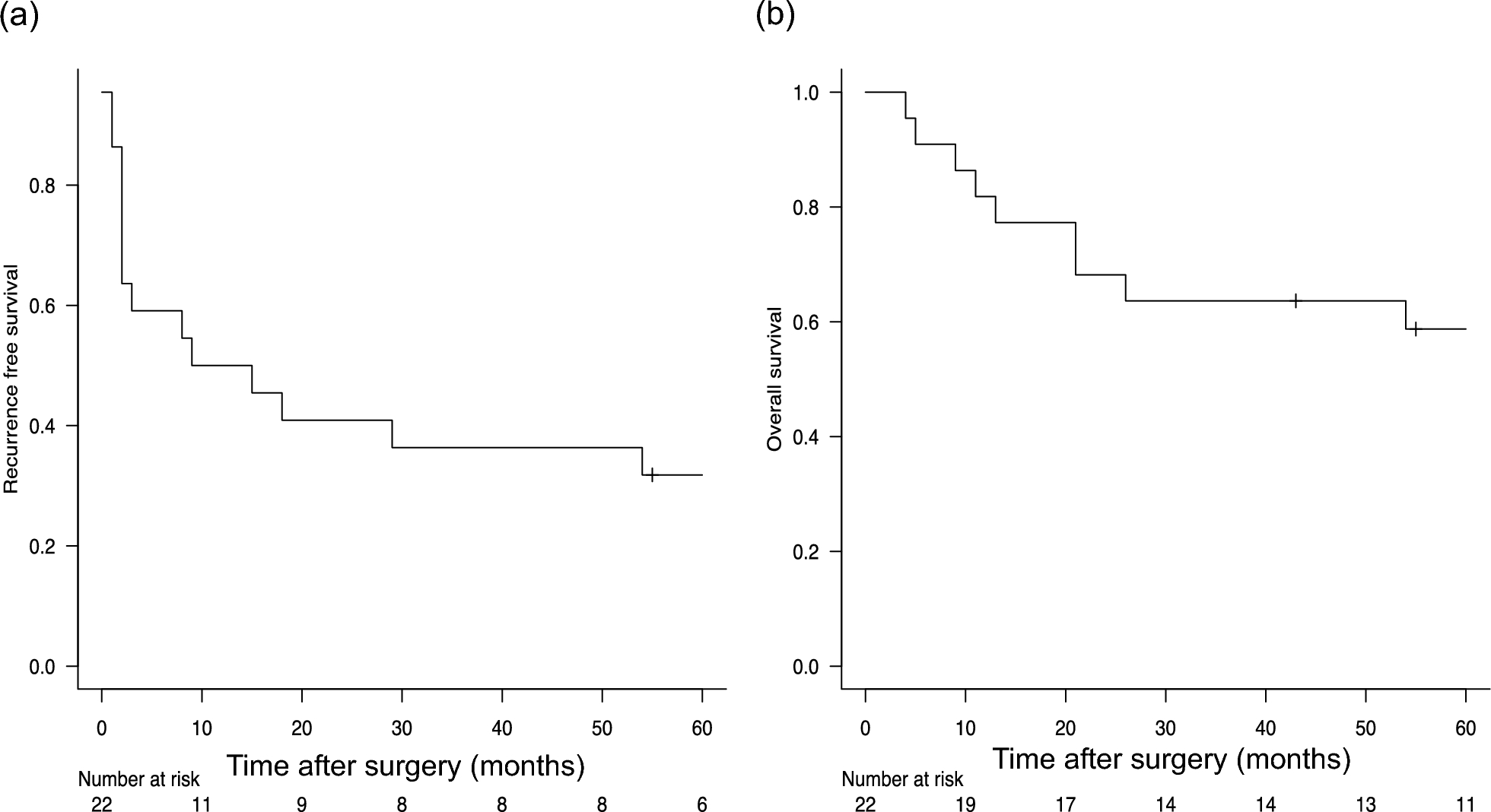
The present study demonstrated that bifocal treatment for patients with synchronous oligometastatic NSCLC with brain metastases provided favorable long-term outcomes, with a 5-year OS rate of 58.7%. It has also been demonstrated that patients who receive TKI therapy have favorable outcomes after recurrence.
The 5-year OS of patients with synchronous oligometastatic NSCLC with brain metastasis who underwent bifocal treatment in our study was much better in comparison to the previously reported rates (8–21.4%) [4, 6, 8, 9]. PET/CT is thought to play a large role in selecting patients with oligometastatic NSCLC for whom bifocal treatment is appropriate. PET/CT has been reported to identify extrathoracic disease more accurately than conventional staging and contributes to the improvement of long-term outcomes in patients with oligometastatic NSCLC [10, 11]. In addition to the accurate diagnosis of distant metastasis, PET/CT has been reported to increase the diagnostic accuracy of nodal status assessment, which is a significant prognostic factor for recurrence-free survival [12]. However, 6 of 22 (27%) cases were upstaged from the clinical to pathological nodal stage in this study. Because the diagnostic accuracy of PET-CT for lymph node metastasis is limited, it is important to thoroughly evaluate lymph nodes during surgery in patients with synchronous oligometastatic NSCLC with brain metastases. Although a bifocal treatment strategy is associated with the limitations of the preoperative assessment for lymph node metastasis described above, we believe that this strategy itself can be justified because of its favorable long-term outcomes.
In addition to the advancement of staging modalities, the improvement in treatment after recurrence may have contributed to a better prognosis in the present study. Although the recurrence rate remained high (i.e., 15 of 22 patients [68%]), the median survival time after recurrence was relatively long (24 months). Frost et al. reported that repeated local ablative therapy for recurrent brain metastases resulted in favorable long-term outcomes [13]. In the present study, two patients had no relapse after local ablative therapy, indicating the importance of aggressive local treatment for brain relapses to provide long-term disease control. The use of TKIs is another factor contributing to prolonged post-recurrence survival. In the present study, it was observed that the five patients who used TKIs after recurrence survived longer than those who did not use TKIs, in accordance with previous reports [14, 15]. Recently, the effectiveness of radiotherapy for primary tumors in patients with oligometastatic NSCLC who underwent TKI therapy was assessed in a randomized controlled trial. In their study, the addition of upfront radiotherapy for primary tumors significantly improved the progression-free survival and OS for EGFR-mutated NSCLC compared with first-line TKI alone [16]. Based on this report, resection of the primary tumor may have contributed to an improved prognosis, even in patients with EGFR mutations.
Based on these findings, aggressive local treatment for brain relapses and appropriate use of EGFR-TKIs are important for the treatment of relapse after bifocal treatment for NSCLC with synchronous brain metastases.
It is important to select cases for which bifocal treatment is effective. In previous studies on synchronous oligometastatic NSCLC with brain and other metastatic sites, several factors, such as old age, multiple metastatic lesions, and lymph node metastasis, were associated with poor prognosis [3, 17]. In the present study, pathological N0 status was the only factor that was significantly associated with better recurrence-free survival. The lack of significance of the pathological N0 status as a prognostic factor for OS may be attributed to the effective treatment of recurrent disease with TKIs in patients with lymph node metastasis. Since all cases that eventually experienced no recurrence had a pathological N0 status, it is thought that patients with a pathological N0 status have a particularly high chance of long-term recurrence-free survival and potential for curative treatment. This supports the proactive application of bifocal treatment in patients with a pathological N0 status.
Whether systemic chemotherapy should be added to bifocal treatment is controversial. In previous reports on oligometastatic NSCLC, patients who underwent chemotherapy first and had no disease progression were allowed to receive additional local treatments [18,19,20]. The National Comprehensive Cancer Network Guidelines also recommend chemotherapy and confirm the absence of disease progression prior to local treatment. In contrast, in our study, most patients underwent thoracic surgery without chemotherapy, and their prognoses were relatively good. Whether chemotherapy should be administered prior to local treatment remains a topic for future investigation. Regarding postoperative chemotherapy, an analysis of the effect of systemic chemotherapy after surgery in patients with NSCLC with synchronous brain metastasis showed that postoperative chemotherapy improved the prognosis in patients with pathological N1, but not in those with pathological N0 [21]. In our study, all patients with pathological nodal involvement experienced recurrence, which led us to consider adjuvant chemotherapy for patients with pathological nodal involvement. Determining whether postoperative chemotherapy should be administered to patients with pN0 disease is a future task.
Immune checkpoint inhibitors (ICIs) have recently become the standard therapy for NSCLC without driver gene mutations. Takamori et al. conducted a propensity-matched analysis using the National Cancer Database to analyze the survival benefit of ICIs in patients with stage IV brain metastases [22]. In their study, multivariable Cox modeling after propensity score matching confirmed the survival benefits of ICIs. In Japan, ICIs have been available since 2017, but only three cases in this study were treated with ICIs; as such, a sufficient analysis has not been conducted. Determining the indication for bifocal treatment for brain metastatic NSCLC without driver gene mutations is a future task.
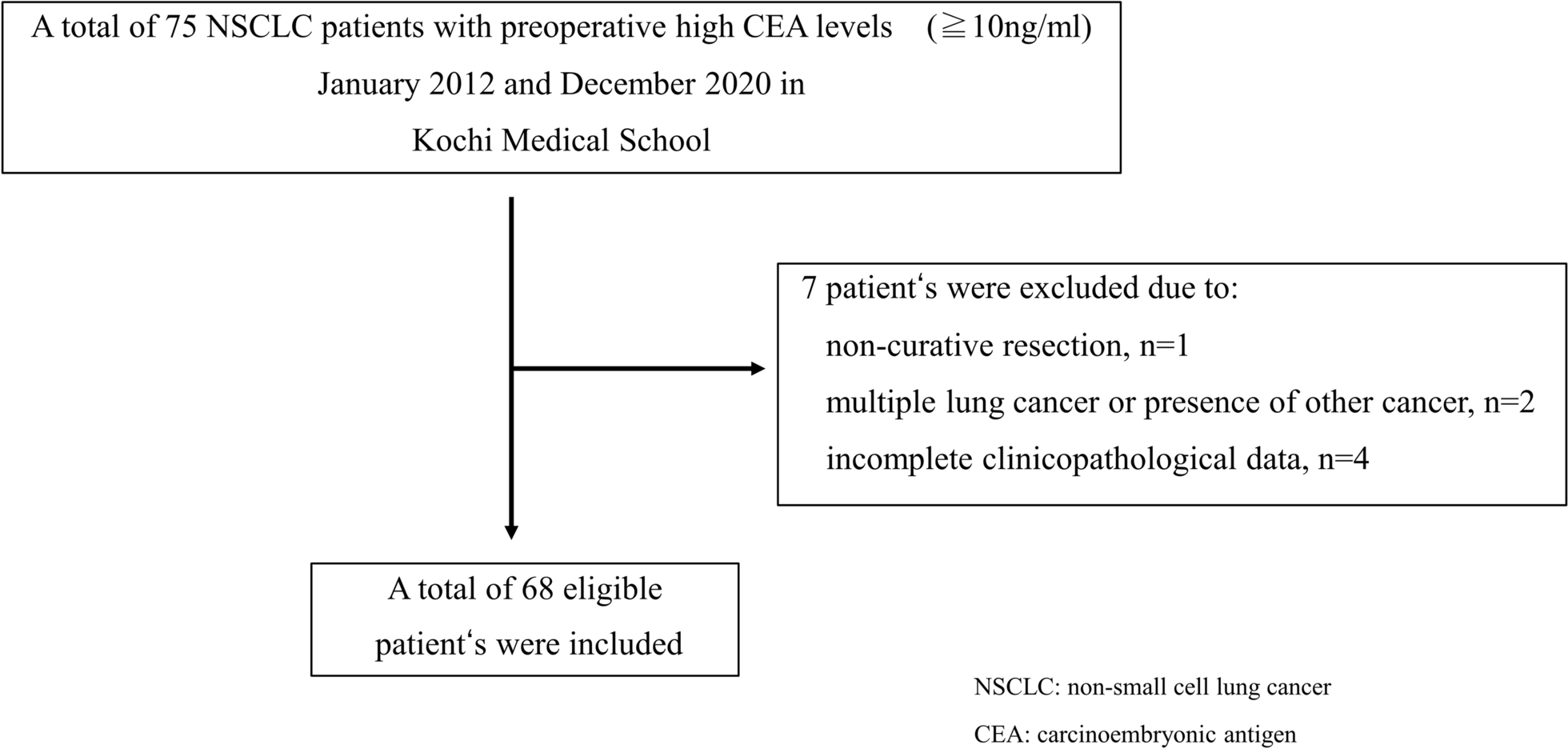
The present study has several limitations. First, this was a single-center retrospective study with a limited number of patients. The favorable outcomes may have been influenced by selection bias. Second, not all cases had pathologically confirmed brain metastases [23]. This may have influenced the outcome of the present study. Third, the analysis involved patients who received treatment for over a decade, during which there were alterations in therapeutic modalities. In particular, the development of second- and third-generation TKIs has had a great impact on outcomes in patients with EGFR mutation-positive tumors. These factors may have influenced the study outcomes. Fourth, the group receiving bifocal treatment was not compared to the control group treated with chemotherapy alone. A multicenter randomized phase III study is needed to answer the question of whether initial surgery plus metastasis-directed therapy or initial systemic therapy is better.
In conclusion, the long-term outcomes in patients with synchronous oligometastatic NSCLC with brain metastases who underwent bifocal treatment, including pulmonary resection, were favorable. In particular, bifocal treatment may provide a chance for a cure in patients without lymph node involvement.





留言 (0)