
記住我




The porcine Freestyle stentless bioprosthesis (Freestyle; Medtronic Inc., Minneapolis, MN, USA) has been implanted as a full root replacement in patients at Haukeland University Hospital since 2001. The performance and durability of the valve have both been reported to be acceptable [1, 2]. Recent observations at our institution show an increasing trend of patients being readmitted with structural valve degeneration (SVD). The type of degeneration in the Freestyle prosthesis differs from that of other bioprostheses as it consists mainly of leaflet tears, and the valve itself usually does not become calcified. Although the incidence is low and it presents after many years, when it occurs the clinical presentation is often acute, with rapid symptom progression [1, 3, 4].
Severe aortic regurgitation (AR) due to SVD or endocarditis is an indication for redo surgery. However, a complete excision of the aortic root, which may be necessary for extended Freestyle root destruction, presents a significant surgical burden and risk. If only leaflet destruction without endocarditis is present, transcatheter aortic valve implantation (TAVI) is an option, but often declined due to lack of valve calcification and anatomical issues inherent to the Freestyle. An alternative strategy when one can preserve the root is to do a surgical valve-in-Freestyle replacement. Rapid deployment and sutureless valves have emerged as alternative to standard surgical aortic valves [5,6,7,8,9,10]. One such is the balloon-expandable stented EDWARDS INTUITY Elite rapid deployment valve (RDV; Edwards Lifesciences, Irvine, CA, USA). The valve has been built upon proven pericardial technology, but also shares technical aspects with TAVI, and the durability should be addressed. More data is warranted, but recent publications show convincing results [6]. The use of RDVs has been advocated in redo surgery to avoid disruption of the fragile tissue found in biological root prostheses [10]. The experience of implanting Intuity in a Freestyle full root is limited [11, 12]. Vendramin et al. have reviewed and recommend the use of RDVs and sutureless valves in challenging reoperations, but the Intuity was employed in a Freestyle full root in only two of these cases [12]. A recent multicenter study found favourable results following implantation of the sutureless Perceval prosthesis (Corcym UK Limited, London, UK) in degenerated stentless aortic valves and full root bioprostheses [13]. On this basis we aimed to assess the outcomes of 6 patients with failing Freestyle full roots treated with implantation of the Intuity valve at our institution.
Case presentationThe results of Intuity valve implantation in 6 patients with a degenerated Medtronic Freestyle full root replacement are reported (Fig. 1). All patients have provided written informed consent for inclusion and publication. Pre-, per- and postoperative data are presented in Table 1 and echocardiographic data in Table 2. Due to few observations the data are presented on an individual level. Continuous variables are presented as mean ± standard deviation (SD) or median (range). Paired-sampled t-test was used to compare echocardiographic values at discharge and follow-up. A p-value \(\:\le\:0.05\) was considered significant. All statistical analyses were performed using SPSS 26.0.
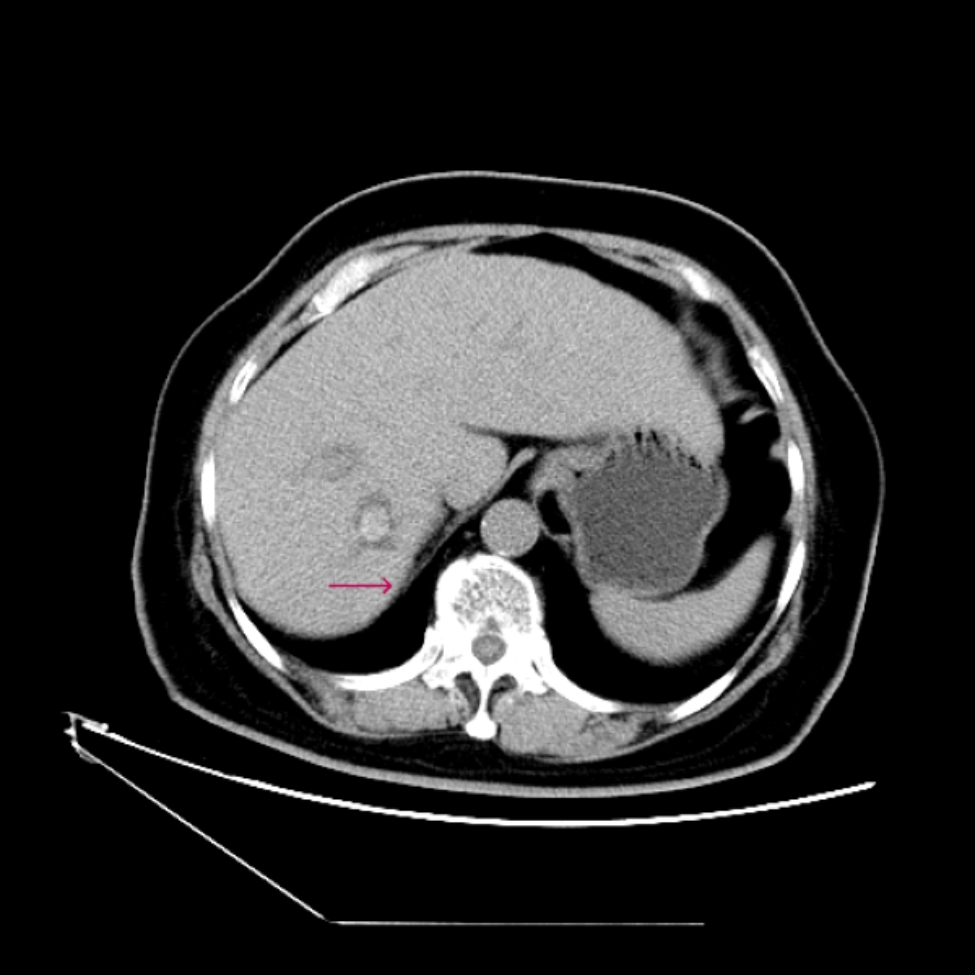
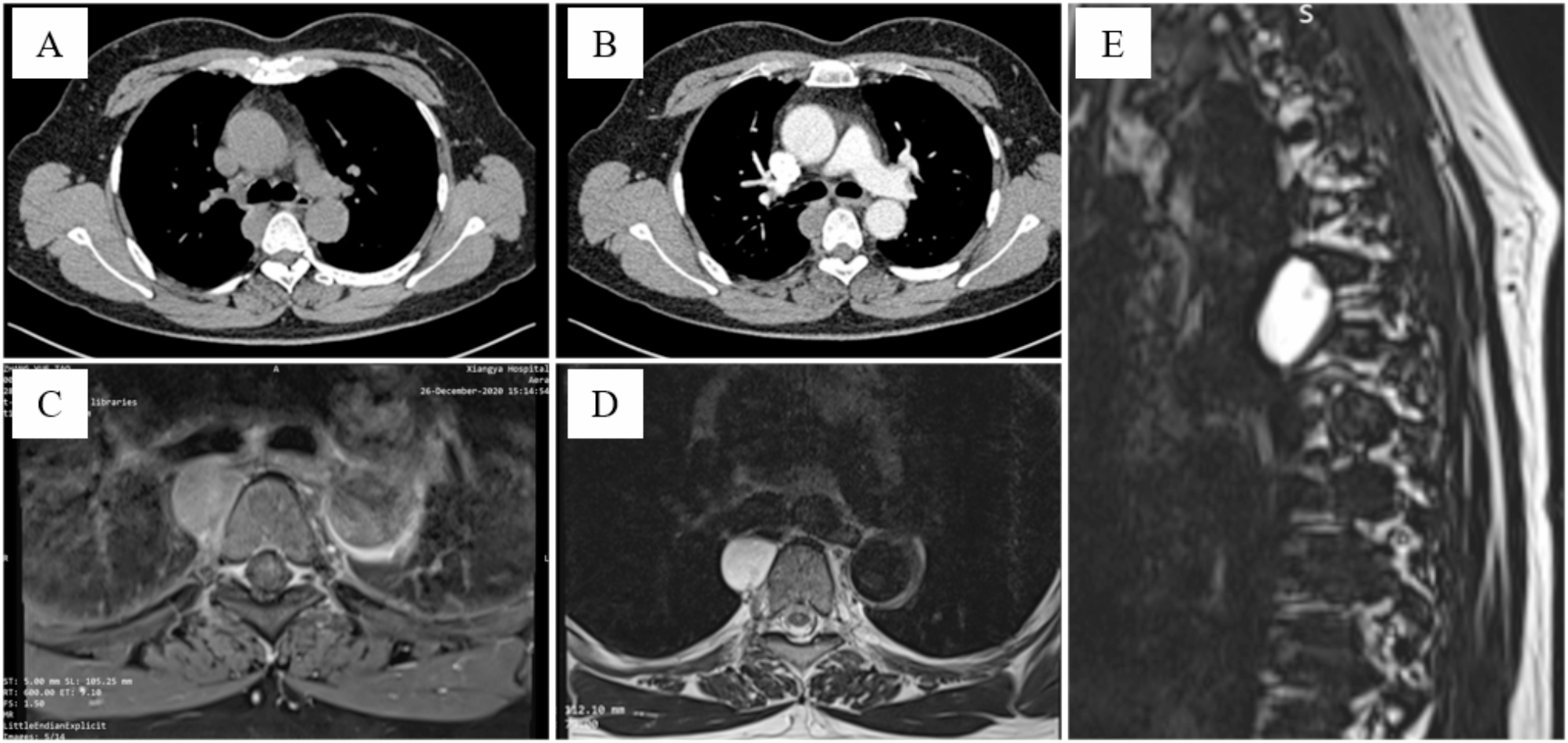
Fig. 1
Intuity in Freestyle. Clockwise from the left: Peroperative image of Intuity implanted in Freestyle after aortic root enlargement. Follow-up cardiac CT-scan as illustrated here showed adequate conditions in the Freestyle root after Intuity-implantation in all
Table 1 Pre- per- and postoperative variablesTable 2 Echocardiography at discharge and latest follow-upPatientsSevere AR was the main indication for surgery. Preoperative cardiac CT and transesophageal echocardiography were performed for detailed assessment of the aortic root and valve. No periannular pathology such as abscesses or pseudoaneurysms were present. All were complex high-risk patients expected to benefit both from a rapid valve insertion, and the favourable haemodynamic and structural profile of the Intuity valve.
Patients 1–3 had a history of endocarditis. At diagnosis blood cultures were positive and preoperative imaging showed involvement of the Freestyle leaflets. Truncal CT-scan and cerebral MRI demonstrated septic emboli to the spleen and brain in patients 2 and 3. Only patient 1 had active infection at surgery treated with intravenous antibiotics for 4 weeks preoperatively. At surgery C-reactive protein (CRP) was reduced to 13 mg/L and valve culture was negative. 16 S rDNA PCR of the leaflets showed streptococcus sanguinis. Patients 2 and 3 were operated after completed antibiotic treatment (≥ 6 weeks) and without any remaining signs of active infection. In patient 2, TAVI was initially performed to treat the AR, but the valve dislocated causing a large paravalvular leakage (PVL) necessitating surgery. Patients 4–6 had SVDs with leaflet tears that manifested more than 10 years after Freestyle implantation. In two of these the tears were in the commissural area.
One patient was female. Age ranged from 48 to 82 years. Mean EuroSCORE II was 12 ± 7. Patients 1 and 6 were second time redo. One patient refused blood transfusion during the complete treatment course.
Surgical techniqueAll patients underwent redo-sternotomy and central cannulation for cardiopulmonary bypass. Antegrade cold blood cardioplegia was administered, and in one patient supplemented with retrograde infusion. The aortotomy was distal to the Freestyle graft, except for patient 1 in which the aortotomy also included the Freestyle root for root enlargement. In patient 2 the TAVI was explanted. The degenerated Freestyle leaflets were completely excised in all patients. In line with the preoperative imaging there were no abscesses or pseudoaneurysms and the Freestyle root could be retained in all, also in the patients with history of endocarditis. The optimal Intuity size was then determined by assessment of the Freestyle root and annulus with the Intuity sizer. It was observed that the largest possible valve implant was systematically 1–2 sizes below the original Freestyle size. The Freestyle size ranged from 21 to 29 mm, while the Intuity size ranged from 19 to 27 mm. The patient with the smallest Freestyle (21 mm) had been narrowed and only Hegar 17 sizer could pass through. The patient underwent root enlargement by an extended aortotomy through the commissure between the left and non-coronary sinus in which a bovine pericardial patch was sewn. This enabled accommodation of the smallest Intuity valve (Fig. 1). Implantation of the Intuity was performed by certified surgeons in accordance with the manufacturer’s guidelines. Three guiding stitches (Ethibond 2 − 0) were placed at nadir. The valve was thereafter parachuted inside the annulus with the Intuity implantation system, and the balloon inflated after achieving a correct position. A safe distance between the coronary ostia and the annulus of the valve was secured.
Postoperative course and outcomeOne patient was reoperated due to bleeding. Otherwise, there were no severe per- or postoperative complications such as myocardial infarction, stroke, need of postoperative mechanical circulatory support, postoperative hemofiltration/dialysis or a new indication for permanent pacemaker. The patients were treated with anti-thrombotic prophylaxis in-hospital. If no other indication for therapeutic oral anticoagulation were present, they were treated with aspirin for a minimum of 3 months postoperatively.
Postoperative echocardiography was performed at baseline (discharge) and after a median of 24 months (range 1–31), presented in Table 2. The peak gradient was 19 ± 7 mmHg at baseline and 14 ± 7 at follow-up. A considerable decrease in both the LV mass index (157 ± 19 g/m2 at baseline vs. 125 ± 19 g/m2 at follow-up, p = 0.007) and LV end-diastolic dimension (6.4 ± 0.6 cm at baseline vs. 5.5 ± 0.5 cm at follow-up, p = 0.005) was observed. A trend towards improvement in the LVEF was evident, but statistically insignificant (baseline 47 ± 6% versus 54 ± 9% at follow-up, p = 0.085). No PVL was noted in any of the 6 patients. All patients had cardiac CT follow-up with no signs of coronary ostial occlusion, valve thrombosis, pseudoaneurysm or other postoperative complications (Fig. 1). During a median follow-up of 30 months (range 7–45) there were no incidents of biological valve failure or any events within the composite endpoint of major adverse cardiac and cerebrovascular events [14].
留言 (0)