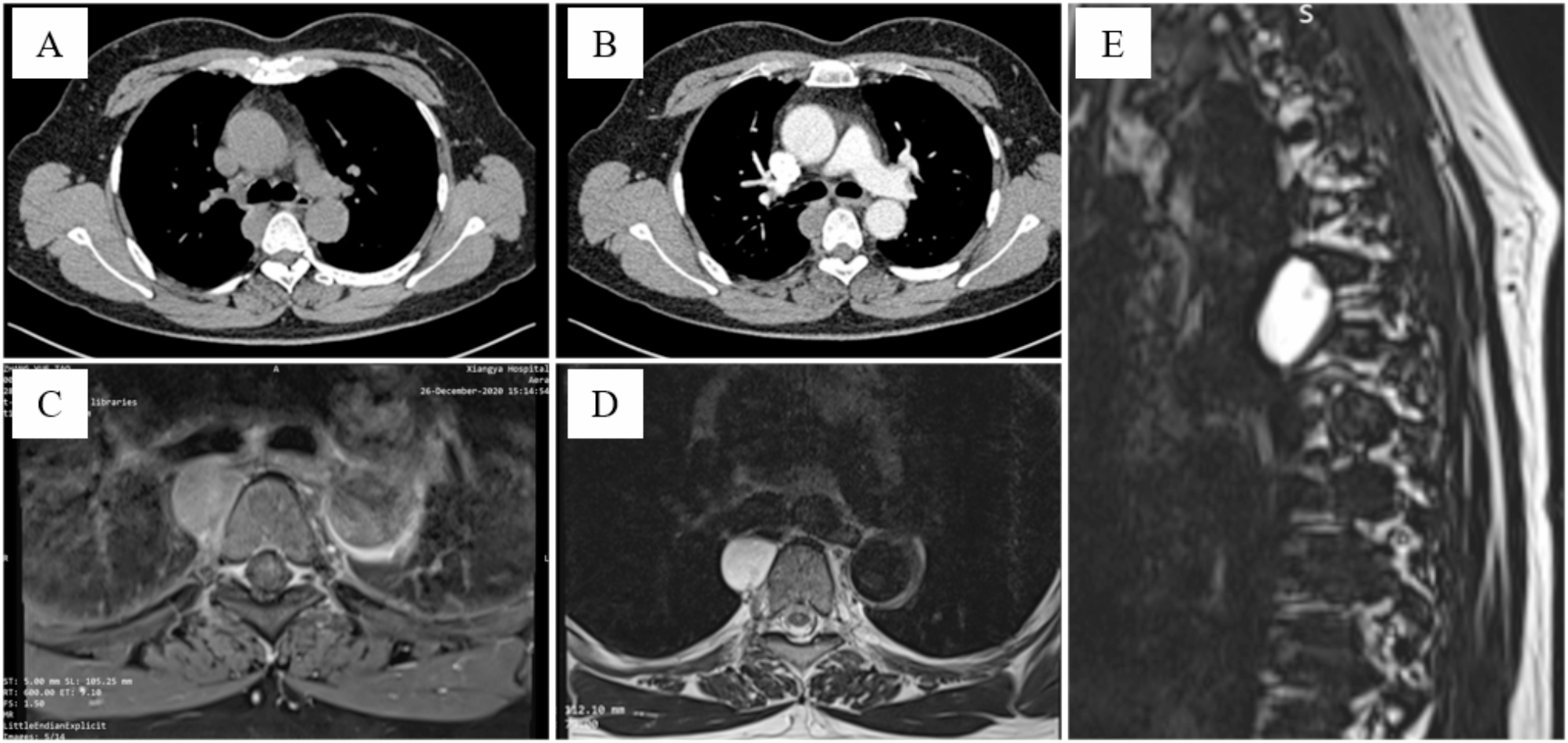
BBF is an abnormal communication between the hepatobiliary tract and the bronchial tree, which develops when bile is inadequately drained via the natural biliary system, leading to bilioptysis, biliary obstruction, and relevant inflammatory reactions in the subdiaphragmatic space followed by subsequent rupture through the bronchial system [7]. Clinical symptoms include bilioptysis (100%), fever (53%), jaundice (29%), abdominal pain (20%), and respiratory disorder (12%) [2]. Some cases presenting with an irritating cough accompanied by yellow or green sputum are often associated with suspicious pneumonia, which is importantly suggestive of potential BBF [2, 5, 7]. Reviewing literature, a total of 11 cases with BBF after radiofrequency ablation all presented with cough and bilioptysis, and other clinical manifestations included liver abscess and hepatic biloma [6]. Patients who develop BBF following hepatectomy often exhibit infectious inflammation, which is believed to contribute to the pathogenesis of BBF. Additionally, it has been mentioned that surgical injury may also play a role in the development of BBF after hepatectomy; however, possible forms of surgical injury in this process were not discussed. And the diathermy burn has been recognized as a pathogenesis of BBF after ablation, but it has not been considered in the case of BBF after surgery. In the past two decades, the increasing application of ultrasonic scalpels in surgery has led to a rise in the risk of undesirable intraoperative diathermy burn, which is uncommon but becoming more frequent. This burn can result in various post-burn effects and complications such as traumatic aneurysms. In this case, the accurate cause of BBF remained unknown. The atrophic liver in the patient may be attributed to cholestasis or an inflammatory reaction induced by hepatolithiasis and closely adhered to the diaphragm. This close adhesion might predispose to diathermy burns during tissue separation using an ultrasonic scalpel in hemihepatectomy. The patient with bilioptysis did not exhibit fever and showed no significant elevation in inflammatory index except for a slightly elevated CRP level. The sputum sample tested negative for bacterial presence. Additionally, ultrasound-guided percutaneous drainage of the right subdiaphragmatic space yielded no fluid collection, confirming the absence of infective inflammation beneath the diaphragm. Therefore, as observed during the surgical procedure, it was speculated that the diathermy burn, which exhibited pronounced corrosiveness and had delayed impact on surrounding tissue, was considered to be the most likely pathogenesis. It is generally believed that the diagnosis of BBF is highly reliable as long as we possess a comprehensive understanding of BBF and conduct meticulous differential diagnosis to distinguish it from pneumonia and sputum contaminated by digestive fluid. As we all well know, bilirubin is the major component in bile. Therefore, detecting bilirubin in sputum provides the most direct evidence of BBF. Both urinary dipstick tests and biochemistry tests can confirm the presence of bilirubin. Additionally, ERCP with contrast medium could trace the fistula tract, facilitating further assessment of BBF [2]. Fortunately, abdominal magnetic resonance imaging sometimes reveals the fistula tract as a useful diagnostic supplement [6].
After reviewing the English literature published on Medline in the past 40 years, less than 100 cases of acquired BBF were reported, and nearly half of these cases were cured through conservative treatments, including percutaneous drainage of subphrenic abscess, endobronchial blocker by fiberoptic bronchoscopy, and percutaneous transhepatic cholangiodrainage or ENBD. Generally, a watch-and-wait period of 1–2 weeks is sufficient to assess therapeutic effectiveness or ineffectiveness. Prolonged observation does not alter the initial trend or predictable final outcomes. Therefore, for refractory BBF cases where conservative treatments have proven ineffective, more surgeons are opting for surgical management rather than uncertain or ineffective non-surgical approaches [2, 5,6,7]. And thoracoscopic surgery alone or laparoscopic surgery alone can be used as well as a combination of both techniques or traditional open surgery. All these approaches can effectively address the problem, with the combined thoracoabdominal approach being the most reliable but causing more trauma. If the primary lesion is located in the chest cavity, the thoracic approach is recommended; whereas if it is in the abdominal cavity, then the abdominal approach should be considered. Following multidisciplinary discussions, we believed that for this case, opting for an abdominal approach would facilitate intraoperative exploration of the lesion site and avoid unnecessary additional trauma. In our opinion, the key to successful surgery lies in accurately identifying the fistula site and thoroughly removing any subdiaphragmatic foci or cutting off their connection between the bronchial tree and diaphragm. In some cases where it is difficult to separate the involved fistula due to intense adhesion or severe inflammatory reactions surrounding it, local limited en-bloc resection of suspicious foci is also clinically feasible and accessible. And pedicled greater omentum tamping in the subdiaphragmatic space would be favorable for absorbing residual inflammation and closing the fistula. Finally, we propose three principles in the management of BBF as follows: (1) Meticulous assessment through multidisciplinary discussion is necessary before considering therapeutic options; (2) Adopting a step-up approach as a therapeutic strategy, starting with non-invasive methods and progressing to minimally invasive, less invasive, and finally invasive methods; (3) Surgery should be chosen without hesitation when conservative therapies are proven ineffective or uncertain. Additionally, for diathermy burn associated BBF after hepatectomy, we advocate surgery due to a reasonable speculation based on this case that the diathermy burn may have affected the small peripheral bile ducts, resulting in stricture or even occlusion. This can subsequently lead to the late onset of BBF that often does not respond to biliary drainage. And regarding the prevention of BBF during hepatectomy, we believe that the following measures should be focused on: identifying high-risk patients with close adhesion between the liver and diaphragm before surgery; employing energy devices appropriately and performing operations with utmost care; meticulously ensuring hemostasis and inspecting the liver cross-section and diaphragm.





留言 (0)