CL is primarily composed of mature adipose cells in the interatrial groove or adjacent to the epicardium, and it can be classified as subendocardial lipomas, intramyocardial, and subepicardial according to the location of occurrence. The right atrium, left ventricle, and pericardium are the most commonly described sites in the literature [3]. Based on the microscopic manifestations, CL can be divided into isolated, intramuscular, and special forms, such as atrioventricular valve lipomatous hamartoma and lipomatous hypertrophy of the interatrial septum [4].
The clinical manifestations of CL are determined by the tumor’s texture, size, location and obstruction status. The most common consequences are dyspnea and arrhythmia. Angina pectoris can be caused by a compression of the coronary artery. If the left ventricle is compressed, the left heart’s systolic function is impaired. Arrhythmia can occur when there is damage to the conduction system. Because lipomas usually have a relatively complete envelope, embolism symptoms are uncommon.
CL should be distinguished from lipomatous hypertrophy of the interatrial septum, myxoma, thrombus, and malignant tumors based on locations, imaging characteristics, mobility, clinical presentation, and age of presentation [5] (Table 1). A probable etiology can be determined by integrating multimodal imaging features with clinical expertise, thereby facilitating further diagnostic investigations and guiding management strategies.
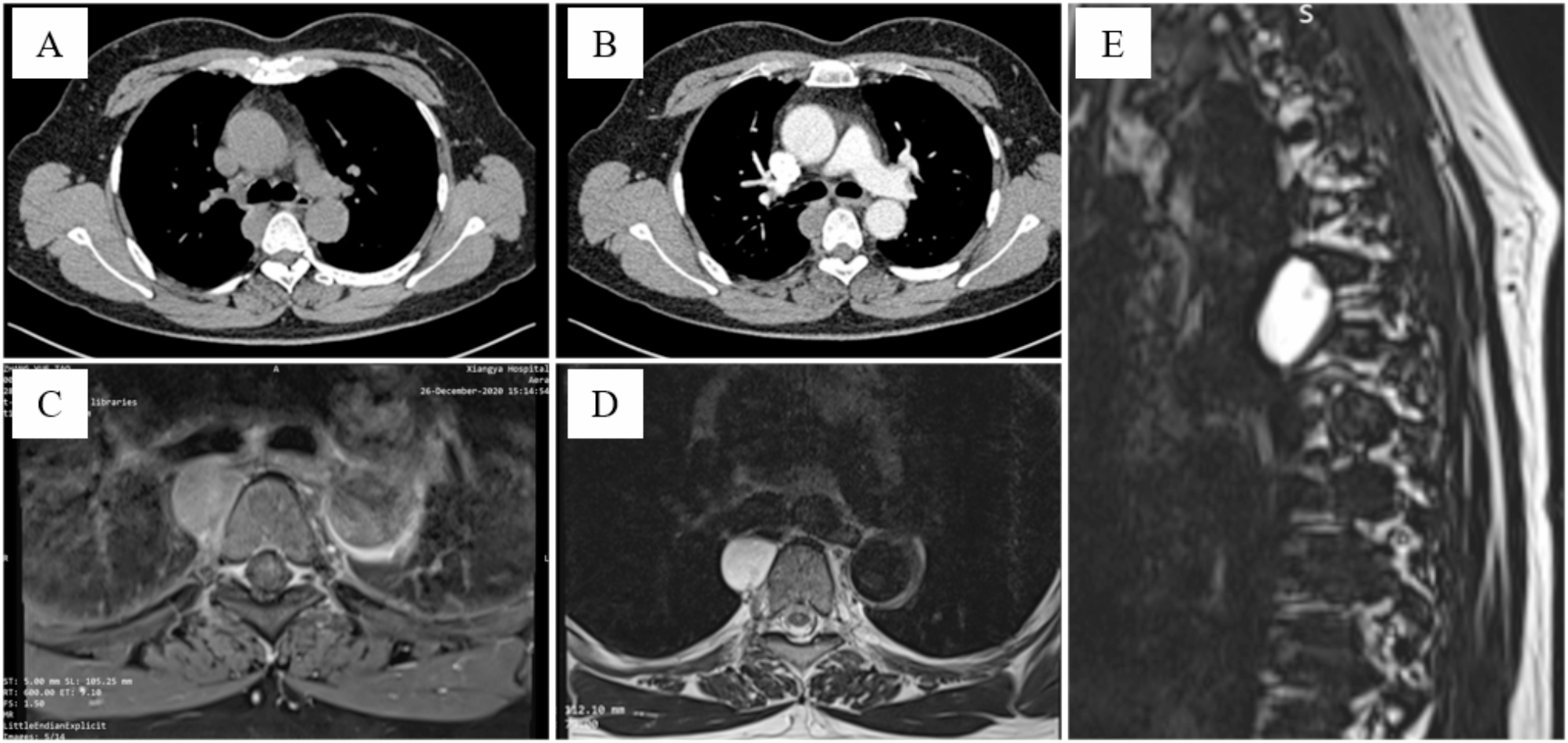
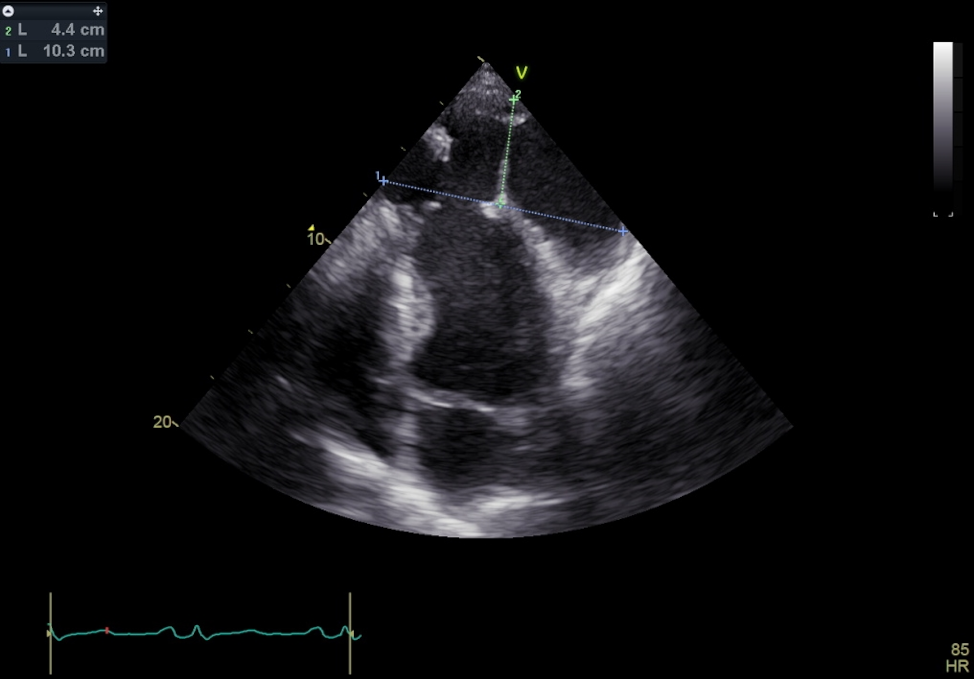
Table 1 Differential diagnosis of Cardiac LipomaIn this case, although the tumor was large, there were no obvious symptoms, which could be attributed to the fact that the tumor did not block the tricuspid valve opening and the patient was young and well tolerated. Due to the large size and mild compression of the right atrium, surgical resection was performed, followed up for three months, and the recovery was satisfactory. This study also has some limitations, such as the lack of genetic testing [6] and the short postoperative follow-up period. The diagnosis of CL often relies on multimodality imaging. Echocardiography can be used as the primary screening and follow-up method and can provide information on echo intensity, homogeneity, and hemodynamic abnormality related to the tumor. The blood supply of tumors provided by contrast-enhanced ultrasound has suggestive significance for benign and malignant. CT can further clarify the neighborly relationship of the tumors and make up for the lack of ultrasound image quality, and the lipoma presents a low-density change, with a specific CT value range of -10~-100. The appearance of CL in MRI has differential significance for the pathological diagnosis of tumor. T1- and T2-weighted image have a high signal, while the fat saturation sequence has a low signal.
The clinical detection rate of CL has increased over the years, and multimodal imaging information was valuable for selecting the intubation method for CPB, determining the location and size of the right atrial approach incision, and assessing the need for valve repair or replacement.





留言 (0)