Ventricular pseudoaneurysm or false aneurysm is a rare and life-threatening condition. This outpouching happens when cardiac rupture contains pericardium, scar tissue, or thrombus, and there is no myocardial tissue [8]. It results from acute myocardial infarction, trauma, bacterial infection, or previous cardiac operations [1]. Patients with LVP can be completely asymptomatic or have nonspecific clinical presentations such as chest pain, arrhythmia, dyspnea, or symptoms of heart failure, acute MI, syncope, tamponade, and embolism that can delay their diagnosis. Also, they can be infected and cause recurrent septicemia [4, 8]. The diagnosis of LVP should be suspected in any patient with a history of cardiac surgery, especially with these nonspecific symptoms. Also, it may be presented with fever, draining fistula, recurrent sepsis, or even pulsatile anterolateral chest wall mass. In the literature review, Staphylococcus aureus was the most commonly reported causative microorganism, responsible for 52% of cases, excluding MRSA. Similarly, in our case, Staphylococcus aureus was identified as the cause of the infection [9]. False aneurysms are more likely to occur posteriorly and laterally, while true aneurysms occur in apical and anteroseptal walls [10]; however, in this case, there was a large pseudoaneurysm formation in the apex and lateral of LV.
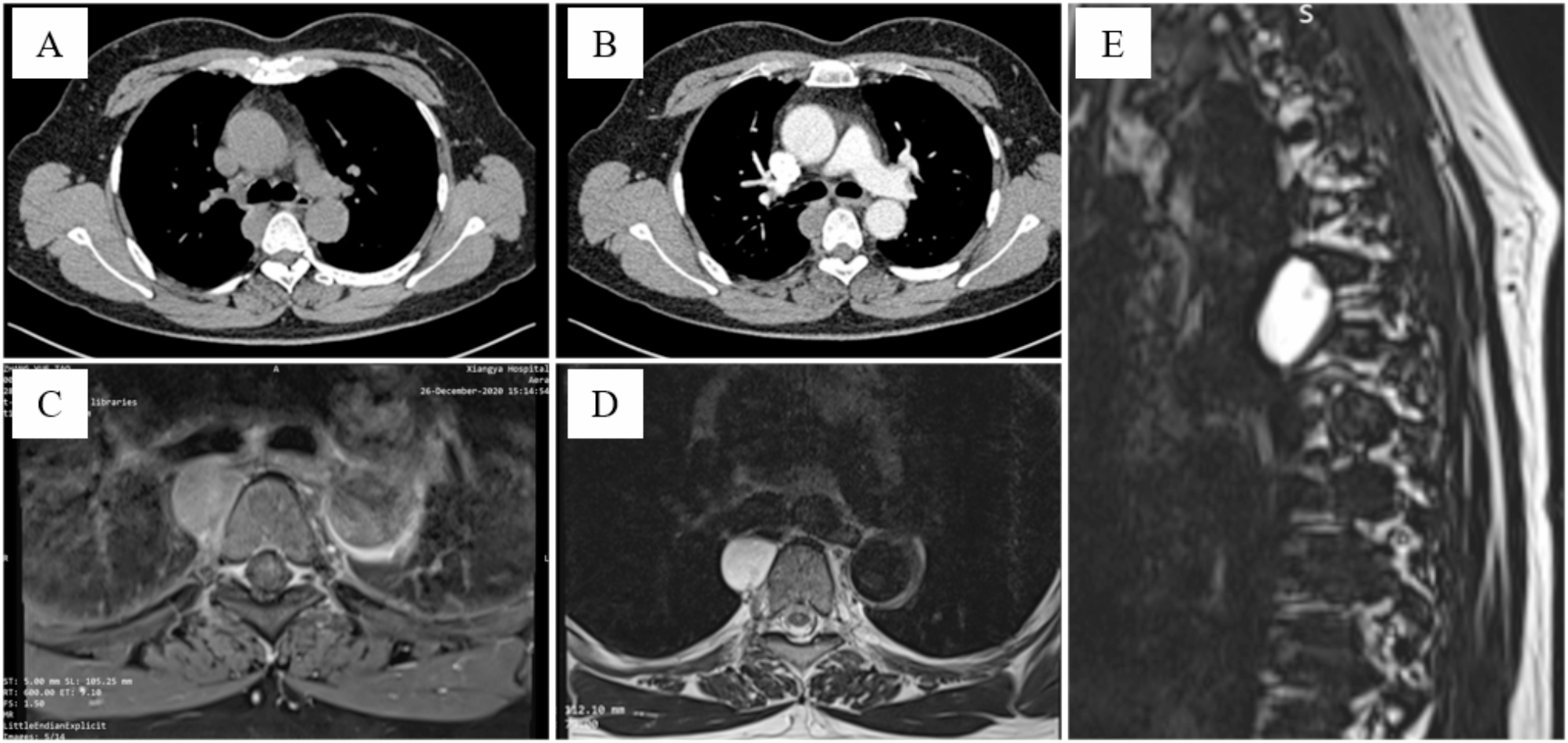
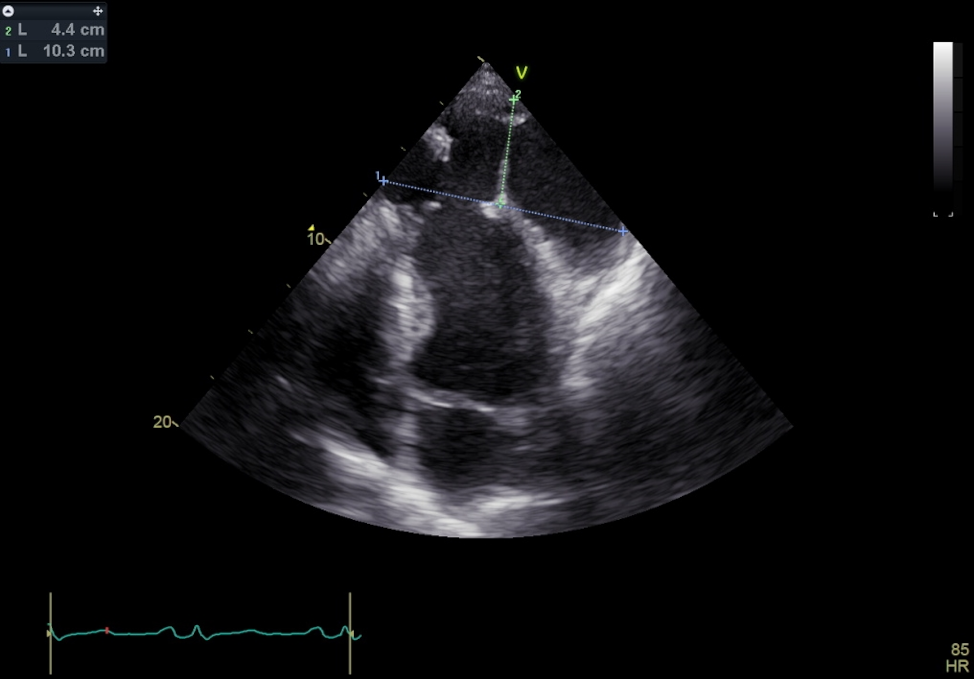
Pseudoaneurysm aneurysms tend to rupture up to 45%, so early diagnosis and therapy are essential [3, 5, 11]. LVP diagnosis is by using noninvasive imaging techniques, including TTE, transesophageal echocardiography (TEE), computed tomography angiogram, and cardiac magnetic resonance imaging [3]. The accuracy of TTE and TEE in providing a conclusive diagnosis is 26% and 75%, respectively [12]. The hallmarks of a pseudoaneurysm on echocardiography include a narrow neck and wide apex, as we detected in our patient, too [8, 13, 14]. In a case series of 23 patients with infectious LVP, echocardiography was the most commonly used imaging tool for diagnosis [9]. Ventricular angiography and Contrast ventriculography have helped diagnose LVP [12, 14]. For the identification of LVPs, multimodality imaging with various axes is advised, which also aids in defining margins and designing a patient’s surgical plan [15].
Surgical repair of an LVP with patch closure is strongly recommended as a first option, particularly for patients with symptomatic or acute conditions, and an operation should be done as soon as possible [3, 5, 16]. However, conventional treatment may be appropriate in specific situations [17]. The surgical approach can be median sternotomy or thoracotomy. The selection process should account for the LVP’s location, preoperative surgery, lung function, and the potential need for concurrent procedures [18]. Median sternotomy is typically performed using peripheral cannulation and deep hypothermia and may require total circulatory arrest [1]. While it offers complete access to the heart, especially in cases requiring revascularization, it has potential drawbacks, including the risk of cardiac chamber injuries, significant bleeding, and the need for extensive dissection during re-operative surgery. It’s also important to note that surgeries of this nature tend to have longer durations. The anterior thoracotomy with peripheral cannulation we used in our patient approach has several advantages. It significantly reduces the need for extensive surgical dissection, eliminates the risk of aorta and right heart chamber injury, and maintains the integrity of previous coronary graft conduits, lessens the probability of sternal wound infection and dehiscence, and also diminishes the risk of peripheral thromboembolization, primarily due to reduced manipulation of the heart [18]. In our case, because of the location of LVP and the surgeon’s decision to perform the procedure via left thoracotomy due to better accessibility. This approach, rather than the more traditional sternotomy, allowed for optimal exposure and repair of the pseudoaneurysm, demonstrating an innovative and patient-specific surgical strategy.
To prevent recurrent infections in the management of LVP, early identification of an infectious pseudoaneurysm is essential, as it significantly reduces the risk of complications, including recurrence. After that, delayed surgical intervention increases the likelihood of infection due to the prolonged exposure of necrotic or damaged cardiac tissue, which creates a breeding ground for bacteria. It is critical to remove all infected and necrotic tissue during surgery. Strict adherence to sterile surgical techniques is equally important to prevent the introduction of new pathogens. The use of biocompatible materials, such as pericardial patches, is recommended for repair, as proper closure minimizes the risk of infection by sealing off areas where bacteria could potentially invade or persist. Another critical component in avoiding recurrent infection is antimicrobial therapy. Targeted antibiotic treatment should be initiated preoperatively and postoperatively based on microbial cultures and sensitivities. Prolonged antibiotic administration, often extending over several weeks or even months, may be necessary to ensure complete eradication of the infection. Post-surgical monitoring is also vital. Patients must be closely observed for any signs of infection, as early detection and intervention can prevent recurrence and improve overall outcomes [2, 9].
In conclusion, this case report underscores the complexities associated with infected LVPs in redo surgery. It demonstrates the potential advantages of the anterior thoracotomy approach with peripheral cannulation in select cases. While our experience yielded favorable results, it’s important to note that this approach is not universally applicable and may require careful patient selection. Further research and clinical studies are essential to evaluate this surgical technique’s broader applicability and long-term outcomes.





留言 (0)