Tumor markers commonly utilized in clinical practice for the diagnosis and treatment of various types of cancer [13], particularly NSCLC [14, 15]. However, few studies thus far have suggested the clinical significance of tumor markers for the early detection of cancer. In contract, several studies have indicated the usefulness of a combination of tumor markers. In the present study, we examined cases of NSCLC with high preoperative CEA levels. The findings, indicated that the postoperative reduction rate was useful for predicting prognosis, particularly OS.
The CEA exhibits high levels in colon cancer, gastric cancer, breast cancer, ovarian cancer and NSCLC. The mechanism underlying the prognostic role of serum CEA currently is unknown. Kozu et al. [12] not detect significant correlations among CEA levels and histologic types; nonetheless, they concluded that this relationship remains controversial. CEA values are affected by renal function and smoking status [16]. This study excluded cases with impaired renal function and other cancers. Cases of cancer with high preoperative CEA values are at a higher risk of advanced disease and have poor prognosis.
In patients with pathological stage IA NSCLC, the preoperative serum levels of CEA were not identified as an independent predictor of poor prognosis. However, in such patients preoperative CEA levels are an important indicator of tumor invasiveness and lymph node metastasis. Hence, preoperative assessment of serum CEA is essential in patients with early-stage NSCLC [7]. In NSCLC, the combination of preoperative serum CEA levels and other factors, such as C-reactive protein [17] and, Krebs von den Lungen 6 (KL-6) [18], may serve as a more accurate and useful prognostic factor versus individual variables.
The serum levels of tumor markers will change following tumor resection [19, 20]. Comparison of changes between the preoperative and postoperative CEA levels can be used to predict the prognosis of colorectal cancer [10], rectal cancer [21], and NSCLC [6, 11, 12], this offers guidance for the development and implementation of personalized treatment strategies. Duan et al. [6] reported that patients with high serum CEA or CYFRA 21–1 levels prior to and after following surgery had shorter OS and RFS than those with low levels. Tomita et al. [11] reported that, in patients with NSCLC, postoperative serum CEA is a more useful prognostic factor than the post/preoperative serum CEA ratio.
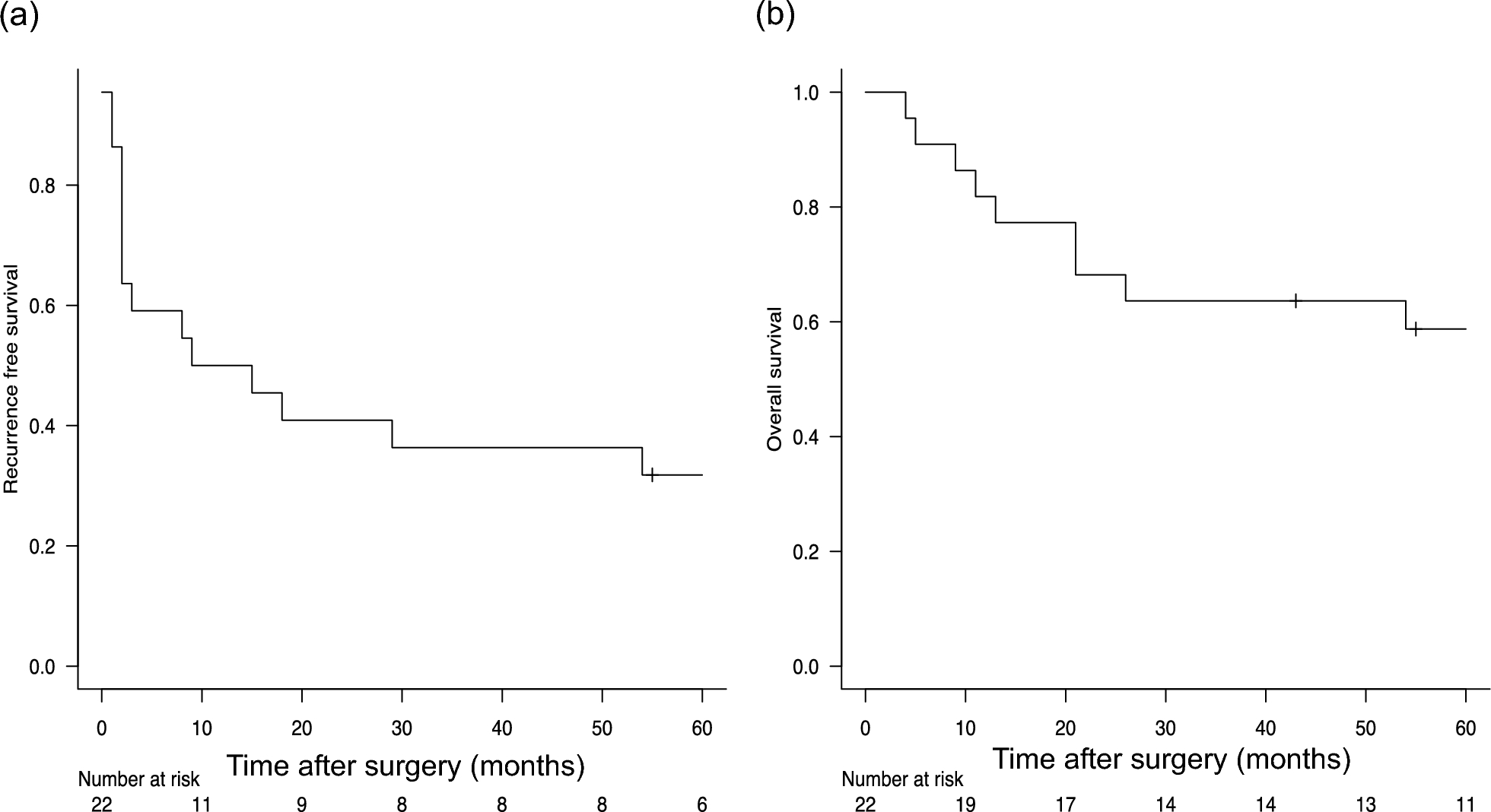
In our study, the CEA reduction rate was a more reliable prognostic factor compared with the postoperative CEA levels. In our study, the target CEA value was 10 ng/ml; in the study conducted by Tomita et al. [11], this value was ≥ 5 ng/ml. It can be considered that the postoperative change is more reflected. We recorded statistically significant differences in OS and RFS, as well as a non-significant difference in DSS. Adjuvant therapy was administered to 69.2% and 55.2% of patients with low and high CEA reduction rate, respectively. The lack of a significant difference in DSS may be partly attributed to the difference in the administration of adjuvant therapy.
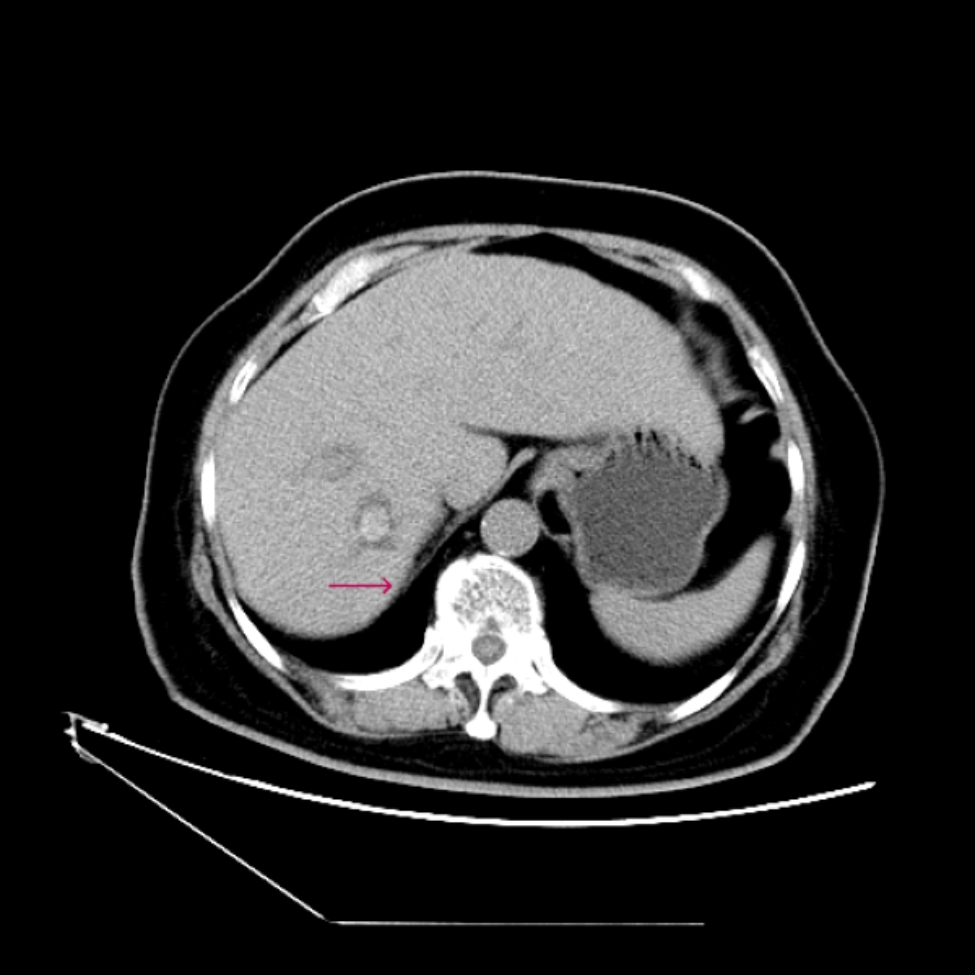
The CEA levels were decreased after surgery in most cases, whereas they were increased in three cases. Case 1 had pathological stage IB disease, and pleural dissemination was observed 47 months after surgery. The patient expired 80 months after surgery. Case 2 presented with pleural dissemination and expired due to acute exacerbation of interstitial pneumonia 4 months after surgery. Case.3 had pathological stage IA2 disease and developed bone metastasis 28 months after surgery; the patients expired duo to the cancer 34 months after surgery. Although the number of cases included in this investigation is small, all patients experienced disease recurrence resulted in death.
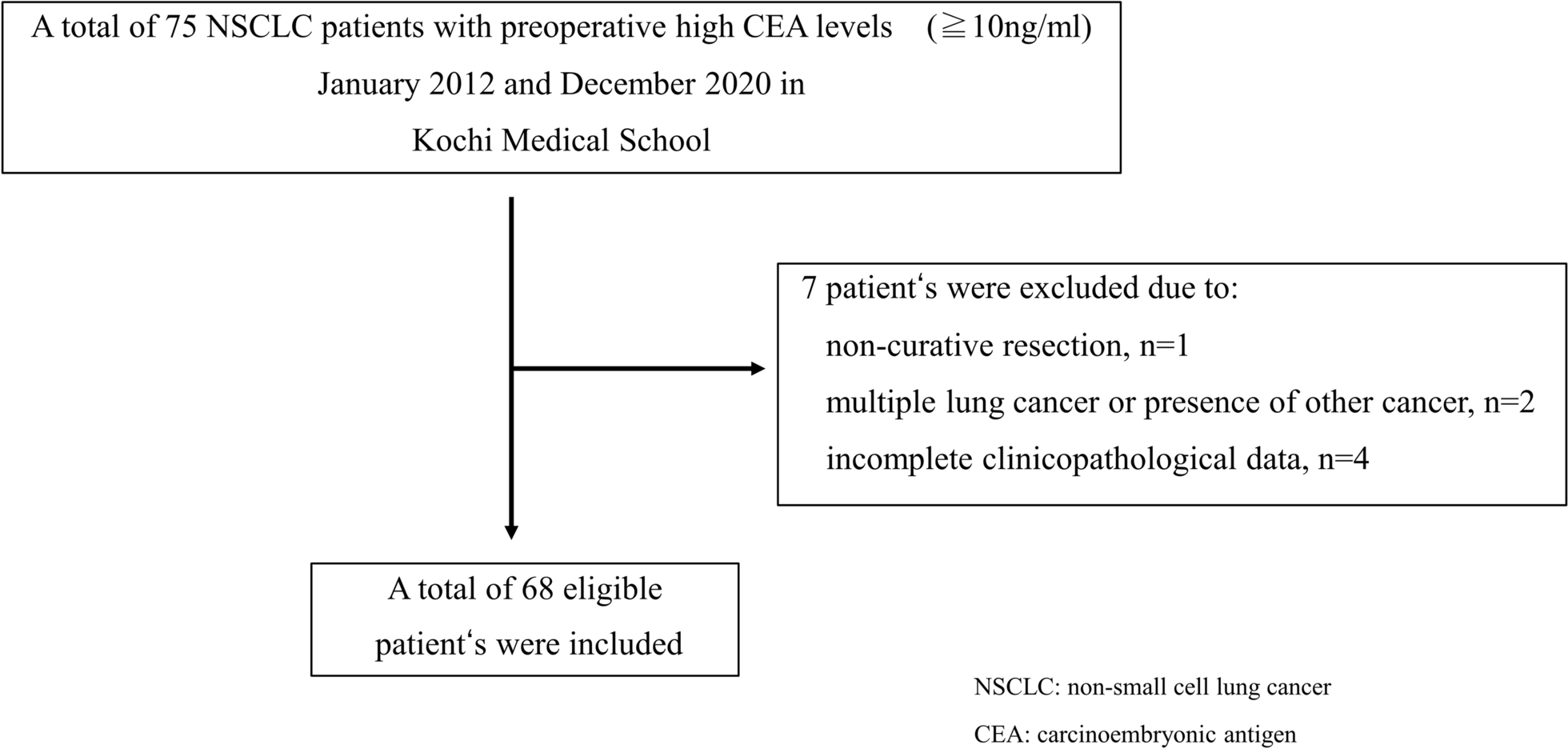
This study was characterized by several limitations, namely its retrospective nature, single-center investigation, and the limited number of cases included in the analysis. Most tests for preoperative CEA were performed within 1 month before surgery; however, there was no clear timeline for postoperative CEA measurements. Numerous other reports have examined the combination of CEA with multiple markers; nevertheless, the present study focused exclusively on CEA. In this study, we only included cases with CEA values ≥ 10 ng/ml. In the future, we plan to conduct a study including cases with CEA values ranging 5—10 ng/ml.





留言 (0)