The initial report of a mediastinal Müllerian cyst was made by Hattori in 2005 [2]. Since then, over 20 case reports have been documented. Sullivan et al. reviewed data from 39 patients with posterior mediastinal Müllerian cysts, revealing that all patients were female, with an average age of 47.2 years and an average cyst diameter of 30.4 mm [3]. The demographic characteristics of our reported cases align with these previous findings.
The etiology of mediastinal Müllerian cysts remains elusive. It is hypothesized that these cysts result from residual Müllerian tissue during embryogenesis [4]. Hattori suggests that the cyst may originate from the transformation of mesothelial cells into Müllerian epithelium. This transformation may involve mesothelial cells converting into cells with Müllerian characteristics under certain conditions, leading to the formation of the cyst [2]. Predominantly, mediastinal Müllerian cysts manifest during the peri-menopausal phase and are frequently associated with a history of obesity and various gynecological interventions, including hormone therapy, hysterectomy, induced abortion, and oophorectomy. These associations suggest that hormonal imbalances may contribute to the development of mediastinal Müllerian cysts [5].
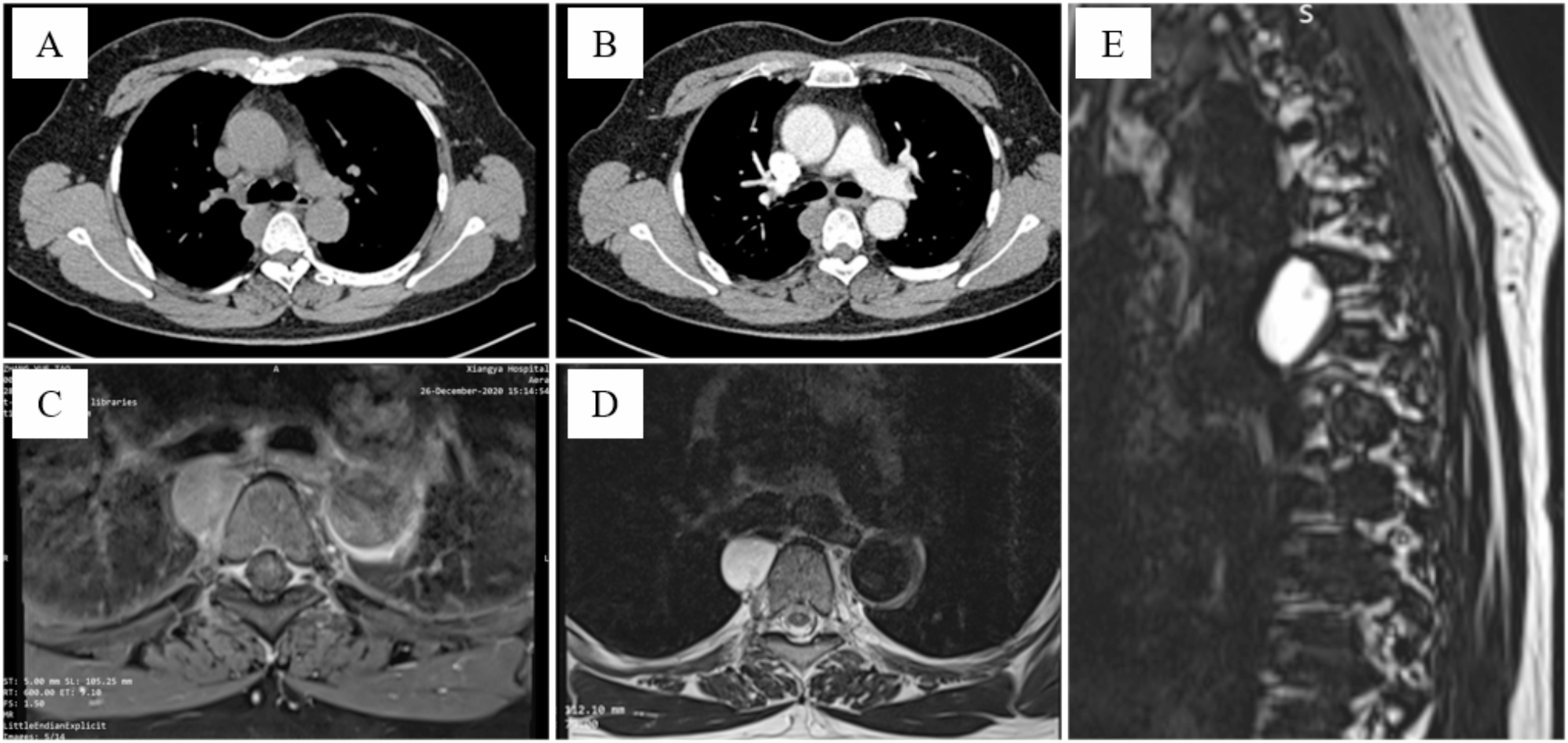
Common posterior mediastinal cysts include lymphatic malformations, spinal meningeal cysts, neurogenic lesions, and foregut cysts. Preoperative imaging often poses challenges in differentiation, with definitive diagnosis primarily relying on postoperative pathological examination. When encountering cystic findings in the posterior mediastinum, the possibility of a Müllerian duct cyst should be considered, especially in peri-menopausal and obese female patients.
PAX8 is a transcription factor belonging to the paired box gene family. It regulates the organogenesis of the thyroid gland, kidney, and Müllerian system. PAX8 immunohistochemistry is a recognized Müllerian marker, expressed in tumors originating from the Müllerian system. It is instrumental in differentiating between Müllerian and non-Müllerian tumors [6]. In this case, the cyst’s epithelium expressed PAX8, ER, and PR, indicative of Müllerian differentiation. The expression of PAX8 is a crucial immunohistochemical marker for Müllerian origin, and the presence of ER and PR suggests a hormonal influence on the cyst’s development. However, the serous papillary cystadenoma-like features observed in the cyst wall’s epithelium have not been previously documented in Müllerian cysts.
Our case presents an extraordinary and rare presentation that distinguishes it from typical Müllerian cysts encountered in clinical practice. Unlike conventional Müllerian cysts, which are benign fluid-filled sacs derived from Müllerian tissue, this case involves a complex transformation into a Müllerian epithelial papillary tumor, closely resembling ovarian serous papillary tumors. This unusual development underscores the complexity and diversity within the spectrum of Müllerian-derived lesions. A critical point to emphasize is that the presence of a papillary growth pattern might initially raise concerns about malignancy, particularly a low-grade carcinoma. However, key diagnostic features that differentiate a benign papillary tumor from a neoplastic one include minimal cellular atypia, well-defined borders, absence of invasive patterns on microscopic examination, and a low proliferation index. These characteristics are essential in distinguishing a benign entity from a potentially more aggressive tumor.
Our case exemplifies the importance of detailed pathological analysis and immunohistochemical profiling in cases with atypical features, such as a Müllerian cyst evolving into a papillary tumor. The rarity of this finding necessitates meticulous evaluation to ensure an accurate diagnosis, which is crucial for guiding patient management and prognosis.





留言 (0)