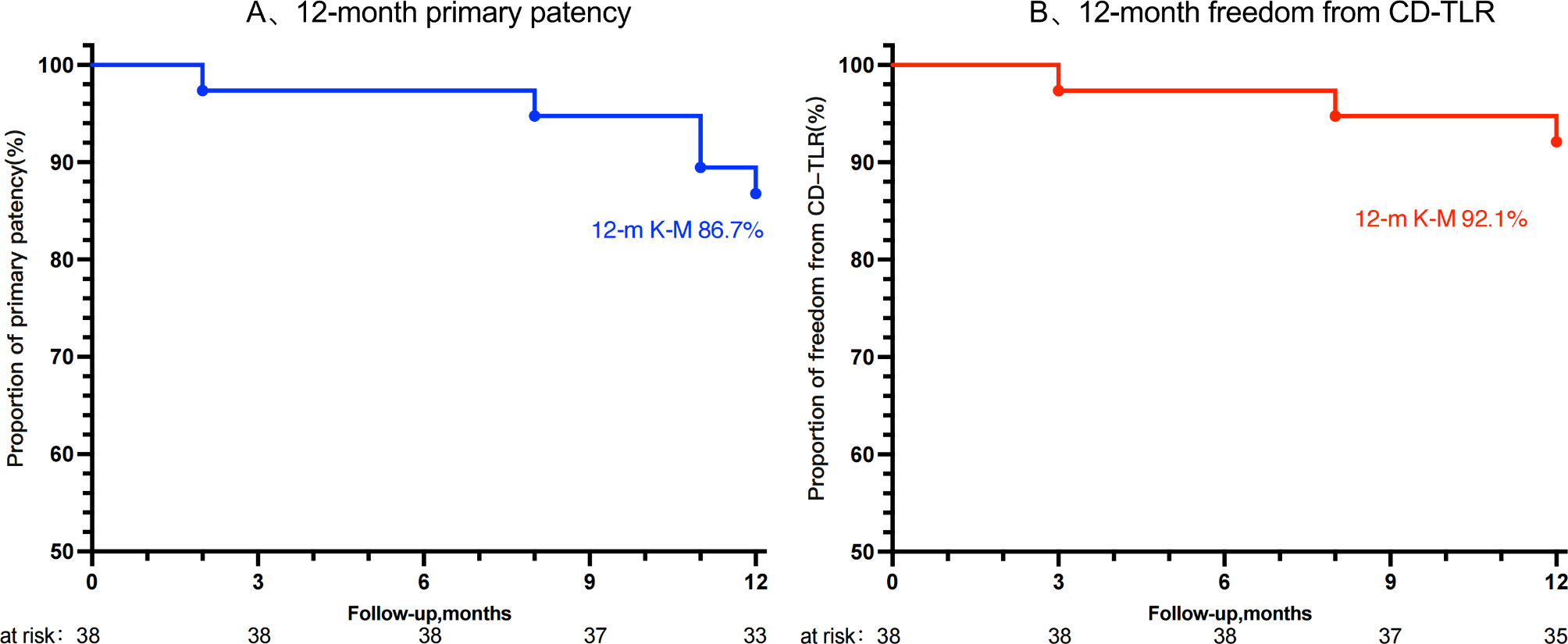
Our study demonstrates that using RA and DCB for treating FP-ISR lesions during the perioperative period is associated with higher safety. All patients underwent successful surgery without any adverse events, and all patients were limb-salvage. Only one patient died due to coronary artery disease. During the 1-year follow-up period, there was a higher initial patency rate and freedom from clinically driven target lesion revascularization. Subgroup analysis based on lesions ≤ 200 mm did not reveal statistically significant differences in primary patency or CD-TLR between the two groups.
The mechanisms of FP-ISR are complex and include progression of atherosclerosis, inadequate postoperative anticoagulation therapy, and continuous intimal compression resulting in smooth muscle cell migration and proliferation, as well as massive extracellular matrix formation and release of various inflammatory cytokines; FP-ISR can be caused by any of these factors [16, 17]. In the early stage, ISR is mainly caused by platelet aggregation and thrombosis due to endothelial injury. Late ISR is primarily due to an inflammatory response induced by long-term stimulation of the endothelium by the stent. This results in smooth muscle cell proliferation, extracellular matrix formation, and a reduction in luminal diameter [18, 19].
To effectively solve the problem of FP-ISR, many scholars have proposed and studied various methods for treating ISR, such as POBA, bare metal stent, cutting balloon, DCB, drug-eluting stent, resorbable scaffolds, etc. POBA is the oldest treatment for FP-ISR; however, the midterm and long-term results were disappointing [13, 20]. Tosaka et al. [15] retrospectively analyzed 133 cases of FP-ISR; the recurrent ISR rate was 49.9% in Class I, 53.3% in Class II, and 84.8% in Class III after POBA treatment at two years. Repeat bare metal stent implantation is not recommended because it can further stimulate the inflammatory response, leading to recurrent stenosis [6, 21, 22].
Because intimal hyperplasia is the main contributor to ISR, which differs from de novo atherosclerotic lesions, in recent years, DCB has been widely used in the FP-ISR. When the DCB is inflated, the antiproliferative drug is released into the vessel wall, inhibiting intimal hyperplasia and inflammation caused by local vascular injury; some studies showed that DCB is advantageous in reducing TLR and recurrent ISR [11, 23]. However, debulking combined with DCB appears to provide more definitive efficacy for long-segment complex lesions. Endovascular debulking devices could be divided into four categories: directional, rotational, orbital, and laser atherectomy [24]. This paper conducted a 1-year follow-up study on FP-ISR patients receiving RA treatment, which proved the effectiveness and safety of RA.
The Straub Rotarex®S catheter tip comprises two overlying metal cylinders with two side openings. The inner cylinder is connected to the catheter shaft, and the outer cylinder is connected to the rotating helix. The outer cylinder is fitted with facets at its foremost head, which, when working, abrade thrombotic material lying in front of it. The helix and the catheter tip rotate at 40,000–60,000 rpm; when a thrombotic occlusion is met, the rotating head breaks down the material with its small, blunt facets in its forward aspect. At the same time, the rotation of the catheter tip creates a vortex effect in the circulation, which helps to erode occlusive material from the vessel lumen [25,26,27] further.
Due to its unique working method, the Rotarex®S device not only can remove thrombi and emboli from the peripheral arterial system without thrombolytics used in the treatment of acute mesenteric ischemia or acute limb ischemia but also is a purely mechanical endovascular atherectomy [28,29,30]. Liao et al. [31] reported on RA angioplasty in 32 patients with FP-ISR at 12-month follow-up, primary patency (86.2%), and freedom from TLR (89.7%), consistent with our study’s results. According to retrospective multicenter research, the primary clinical success/patency rate for the Rotarex®S device in peripheral artery ISR was 92.3% at 12-month follow-up, and the TLR rate was 19.5% [32].
Clinically, the distinction between long and short lesions is typically made at 150–200 mm. To investigate whether there is any significant difference between long and short lesions when treated with RA, a subgroup analysis was carried out in this research using 200 as the border. There was no statistically significant difference because both groups used the RA method. However, some studies have indicated that Debulking may offer a statistically meaningful benefit for long-segment complicated FP-ISR lesions [33, 34].
Although many studies have confirmed the safety and efficacy of RA, the following points should be noted during operation: First, to prevent incomplete aspiration caused by the head end of the aspiration catheter being advanced too quickly and the embolus being rushed to the distal end by the blood flow, which may result in a distal artery embolism, it is advised to first slowly advance the aspiration catheter from the proximal end to the distal end. Second, halt the procedure immediately if you hear anything unusual during the operation to prevent damaging the stent or vessel wall, then remove the catheter for flushing to ensure safety. Finally, a filter may be considered to lessen the likelihood of embolic complications when patients only have one outflow pathway below the knee.





留言 (0)