Chronic empyema associated with BPF is a highly severe complication following pulmonary resection. The effectiveness of treatment typically hinges on proper drainage of pus, closure of fistula, and eradication of remaining cavity [8, 9]. Early surgical intervention may prevent the deterioration of the condition, but some patients may show obvious weakness when they experience infectious symptoms, losing the opportunity to repair the fistula early and eventually developing chronic empyema [10]. The common characteristics observed in these patients include prolonged drainage with a chest tube, chronic consumption by the body, and irregular changes in the huge abscess cavity in some patients with a larger body size. These factors can pose challenges in clinical management.
The optimal management strategy for treating chronic empyema associated with BPF remains a topic of debate in the medical field, especially in patients undergoing pulmonary surgery. While surgical treatment is often recommended as the primary approach, there are still numerous uncertainties that thoracic surgeons face post-treatment, despite advancements in medical technology [9, 11, 12]. Hippocrates documented chest drainage techniques over 2000 years ago, which are still utilized in modern medicine [13]. Historically, the treatment of chronic empyema has involved classic methods such as Heller’s thoracomyoplasty. The primary surgical approach consists of intraperiosteal resection of the ribs and thickened fibrous tissue, which may also necessitate the resection of a portion of the transverse process. This technique aims to preserve the periosteum and intercostal muscles, while also taking care to avoid damage to blood vessels and nerves. However, this method results in complete collapse of the thorax and is associated with significant surgical trauma. Ongoing research and advancements in treating empyema have established the removal of abscess cavities and closure of fistulas as essential components of clinical cure. The process of eliminating dead space in the body involves two main approaches: reducing the volume of the chest cavity and filling the remaining space [7, 14, 15]. The reduction of chest cavity volume typically requires the removal of a significant portion of the ribs to reshape the thorax. On the other hand, filling the remaining space involves using autologous tissue flap with a rich blood supply to effectively fill the abscess cavity, ultimately controlling infection and preventing its recurrence.
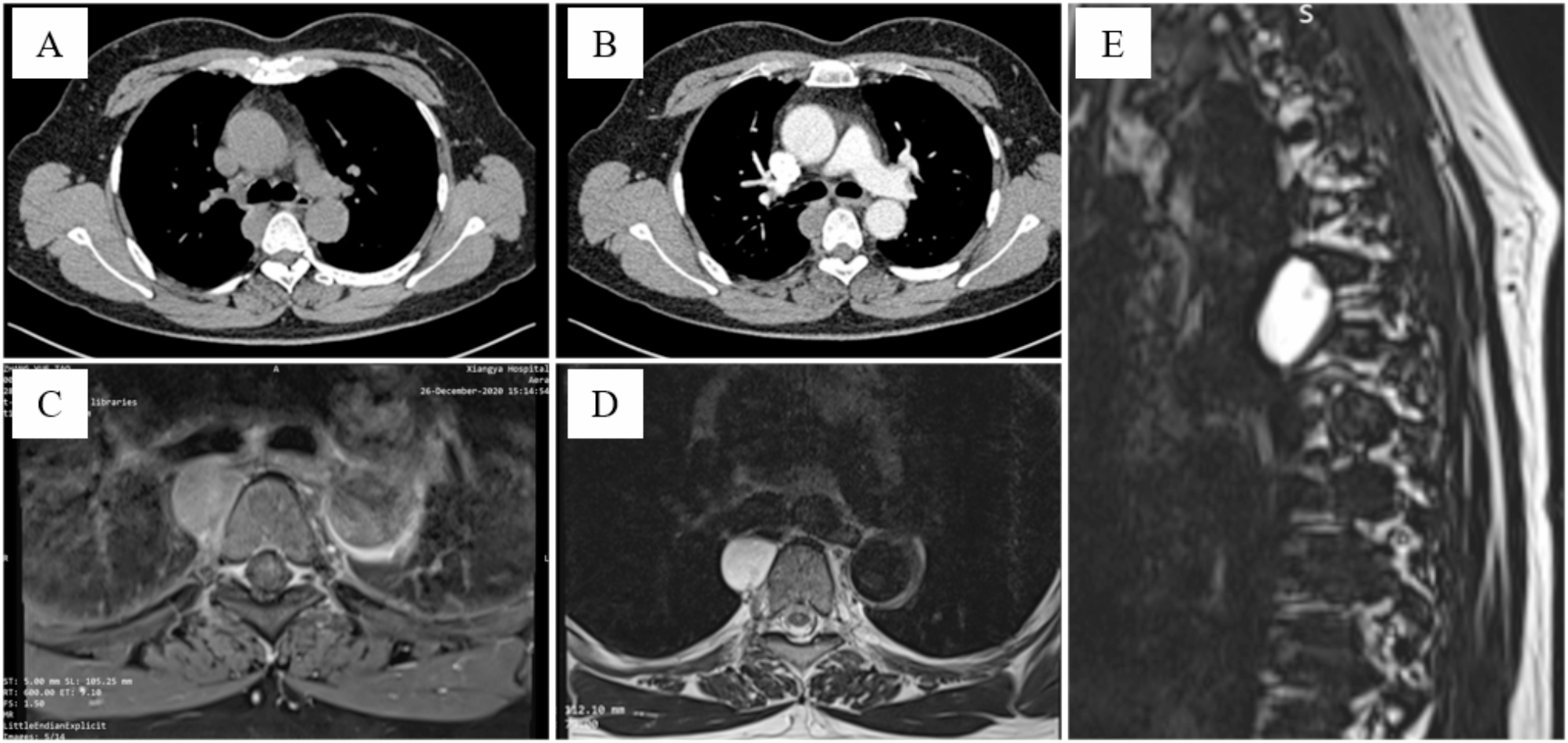
In cases of chronic empyema with a huge abscess cavity distributed across multiple regions, there have been reports of utilizing microsurgical techniques to transfer free myocutaneous flap for treatment. However, the use of pedicled tissue flap for treatment is uncommon [16,17,18]. The primary challenge lies in the insufficient volume of the tissue flap obtained, which may not adequately fill the residual cavity, potentially leading to empyema recurrence or healing failure due to migration. This particular patient has a tall and slender physique. Unfortunately, post-lung surgery complications have resulted in wide range of abscess cavity and complicated with BPF. Generally speaking, in order to achieve clinical cure, we often ensure that the infection in the abscess cavity is well controlled, the BPF is completely closed, and the volume of abscess cavity is reduced and controlled within ideal range. Based on the preoperative bronchoscopy and chest CT examination results, we showed that the shape of abscess cavity was complex and changeable, the abscess cavity was huge. In addition, it was also accompanied by BPF. How to finally complete the filling of the complex abscess cavity on the basis of controlling infection and closing fistula is the key to subsequent treatment, especially the repair and reconstruction of the abscess cavity under ideal conditions.
In recent years, there has been an increasing prevalence of autologous tissue flap transplantation in the management of chest wall infections and chronic empyema [19, 20]. Commonly utilized flaps include the PM, LD, and greater omentum. The PM muscle flap is superficial in location and has dual blood supply. As a pedicled muscle flap, it offers a large and thick area for harvesting, capable of covering the entire superficial chest wall space. The LD muscle flap, with its rich blood supply and minimal anatomical variations, provides advantages such as large volume, extensive range of motion, and high safety. It can be transferred to the entire ipsilateral chest, midline, and contralateral axillary folds [21, 22]. In this case, we made improvements on the basis of Heller’s thoracomyoplasty, primarily utilizing a muscle flap thoracoplasty approach combined with partial rib segment resection. Additionally, this method adheres to the concept of staged surgery, incorporating a transitional treatment involving window opening and dressing changes between the first and second stages of the procedure. This approach facilitated the spontaneous collapse of the chest and contributed to the reduction of the abscess cavity. Following the principle of adjacent repair, the abscess cavity was filled regionally, dividing it into three areas: upper, middle, and lower. The upper area was primarily addressed with PM muscle flap, whereas the middle and lower areas were predominantly treated with LD muscle flap and greater omentum flap. The LD is well-known as the largest and most dependable muscle flap, taking on a V-shaped form. The proximal end of the muscle can be pedicled by either the thoracodorsal blood vessels or the serratus branch [21, 23]. Considering that the abscess cavity of this patient was narrow and long, multi-spatial distribution and irregular, and the application of a single pedicled muscle flap could not meet the filling requirements, we used OWT to control infection based on the completion of empyema debridement and fistula closure in the first-stage surgery, which changes the volume of the abscess cavity or further promotes the expansion of the remaining lung, so as to create conditions for the second-stage surgery [24]. The practice of packing sterile gauze into the abscess cavity via an open wound primarily relied on the principle of siphon action, utilizing the pressure gradient between the inside and outside of the wound to facilitate the gradual drainage of pus along the gauze. This approach accelerated the outflow of pus, particularly in deeper cavities where pus tends to accumulate. The use of sterile gauze proved advantageous in ensuring unobstructed drainage, effectively preventing pus accumulation, controlling infections, and fostering the development of new granulation tissue [25]. When the residual cavity was reduced to the ideal range, the pedicled combined muscle flaps transfer were applied according to the abscess cavity area division to complete the repair and reconstruction. The case involved ongoing dressing changes for a duration of six months. The volume of the abscess cavity was reduced by nearly 50% compared to its original size, and the patient’s BMI showed significant improvement from baseline. However, managing the residual cavity remained a considerable challenge. Given the patient’s psychological trauma and strong desire for surgical intervention, we formulated an individualized treatment plan for him. In consideration of the unique circumstances surrounding the patient’s abscess cavity, we attempted to use a portion of the LD divided into bifurcations for the first time. Despite the utilization of the pedicle PM for closure, a residual defect in the region above the abscess cavity persisted. The primary focus of these procedures was to ensure adequate blood supply to the dominant vessels, emphasizing the necessity for the bifurcated secondary muscle flap to possess substantial tissue rather than a fragile composition. It is crucial to maintain the tissue integrity of the pedicle of the muscle flap to prevent potential muscle necrosis resulting from inadequate blood flow. By eliminating dead space and minimizing postoperative effusion and blood accumulation, the likelihood of empyema infection recurrence is significantly reduced.
In cases of chronic empyema with huge irregular residual cavities, our use of the pedicle combined muscle flaps sub-regional treatment method shows promise in clinical practice. However, it is essential to be prepared with multiple alternatives should the pedicled muscle flap approach fail. For instance, treatment models utilizing free myocutaneous flap or greater omentum to fill the abscess cavity exist, although the former necessitates microsurgery and carries higher surgical risks. The latter option involves additional abdominal trauma, and the volume of the omentum cannot be reliably assessed preoperatively. Regardless of treatment strategy, it is essential to fully control infection and close BPF in order to create optimal conditions for the second-stage surgery and improve the chances of curing empyema. Therefore, utilizing combined pedicled muscle flaps to address chronic empyema with BPF is a viable and effective surgical approach. These muscle flaps offer flexibility in design, ease of acquisition, and demonstrate positive clinical outcomes.





留言 (0)