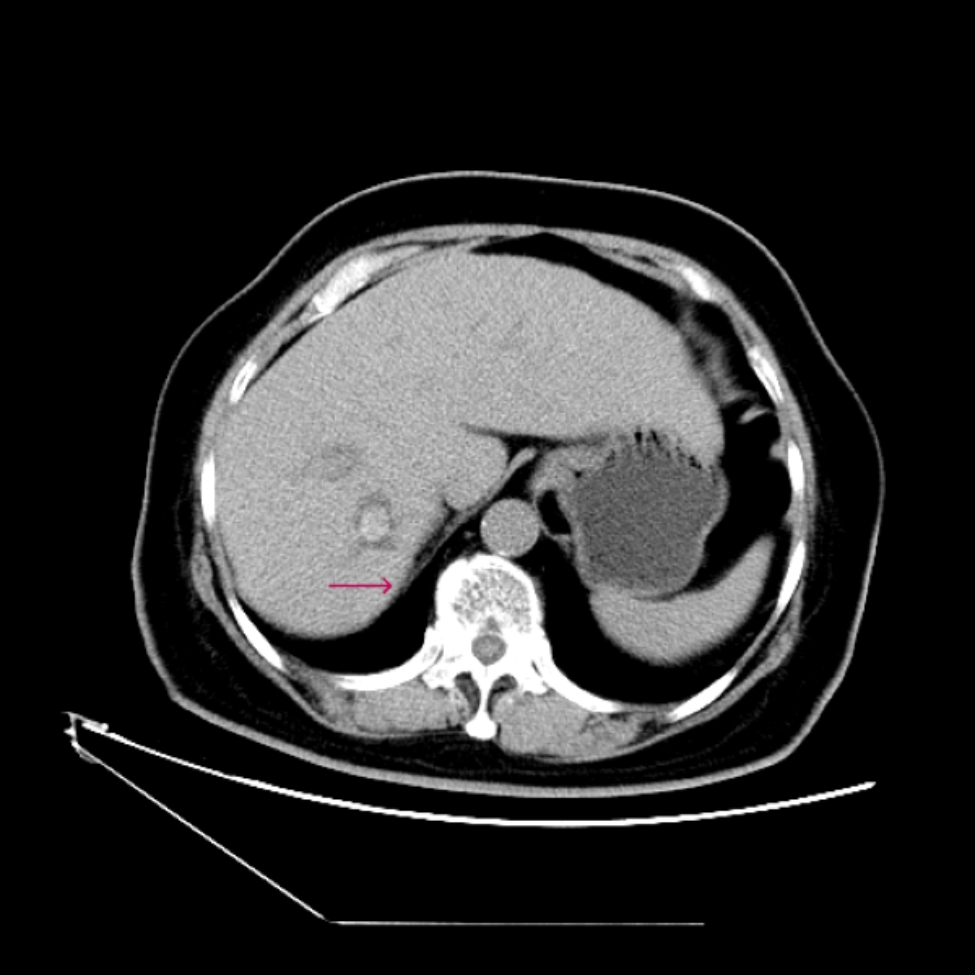
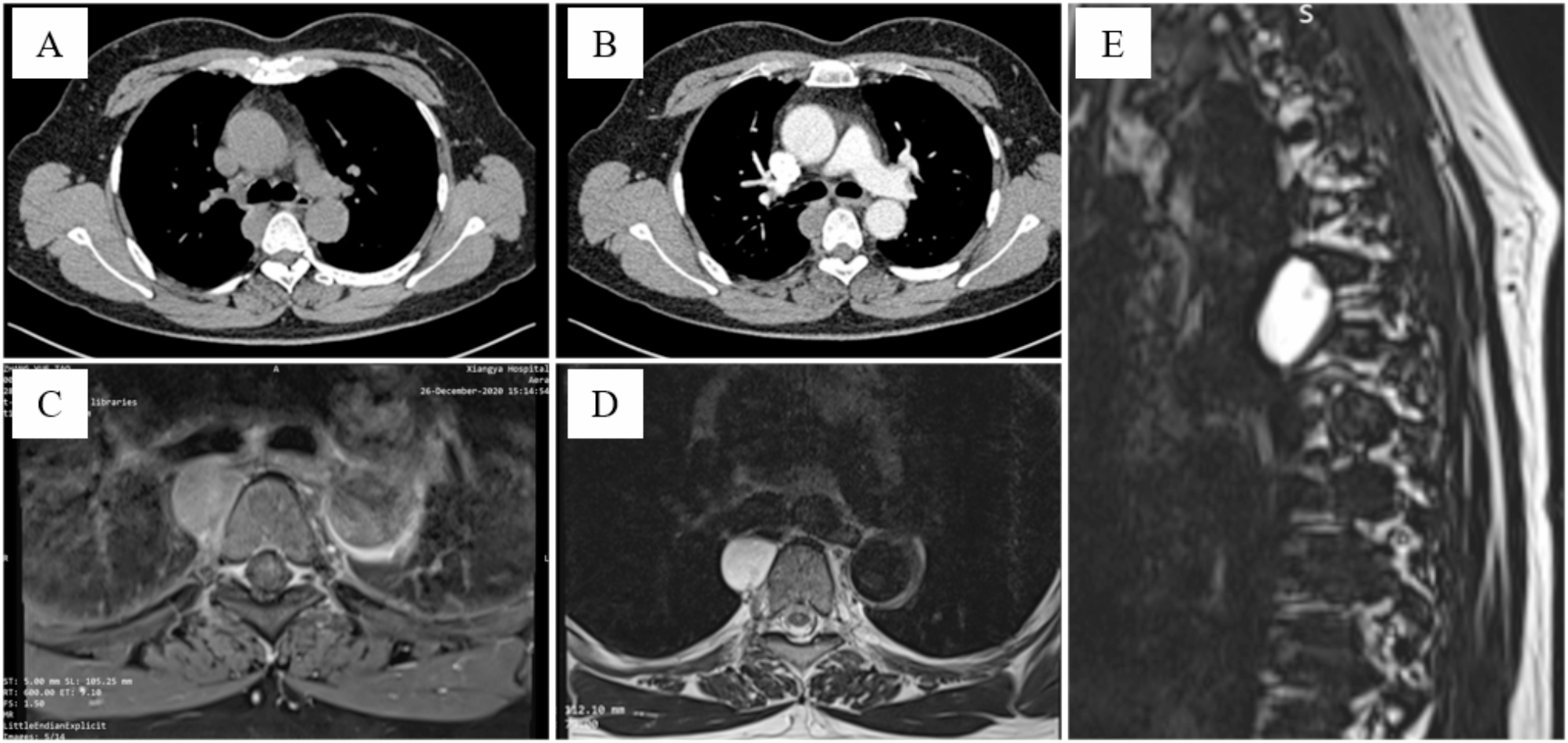
Thymomas and thymic adenocarcinoma are the most common primary anterior mediastinal masses, while thymic adenocarcinoma is far rarer but much more likely to spread [7]. Patients with early thymic tumors often have no obvious clinical symptoms. With the continuous growth of thymic tumors, patients may develop symptoms such as chest tightness, chest pain, and even superior vena cava syndrome. These symptoms are generally caused by tumor infiltration or compression, making it difficult to operate at this stage and challenging to achieve complete removal [2, 8]. With the development of the economy and society, more and more healthcare facilities have included low-dose spiral CT in routine physical examinations. Many patients with early thymic tumors have been identified for the first time during these examinations [9], indicating that chest CT plays an irreplaceable role in screening and diagnosis [10, 11]. When a thymic tumor is first detected, we suggest performing an enhanced CT to evaluate its relationship with the innominate vein, pericardium, aorta, and branches, and to assess the feasibility of tumor resection. When the diagnosis is difficult, enhanced MRI [11, 12] can be performed to distinguish solid tumors or cysts. Thymic tumors are the most common mediastinal tumors. They are often located in the anterior superior mediastinum, with the sternum in front, innominate veins, pericardium, aorta, and branch vessels behind, and bilateral pleura and lung tissue on both sides [8]. Because of its special anatomical location, thymic tumor resection is often considered high-risk surgery [8]. Since Landreneau [13] et al. first reported video-assisted thoracoscopic resection of mediastinal tumors in 1992, video-assisted thoracoscopy has played an important role in the diagnosis and treatment of thymic tumors [3, 14, 15]. However, there is no article that uses a standardized approach to surgery as we do, so there is an urgent need for a standardized surgical method to simplify the operation.
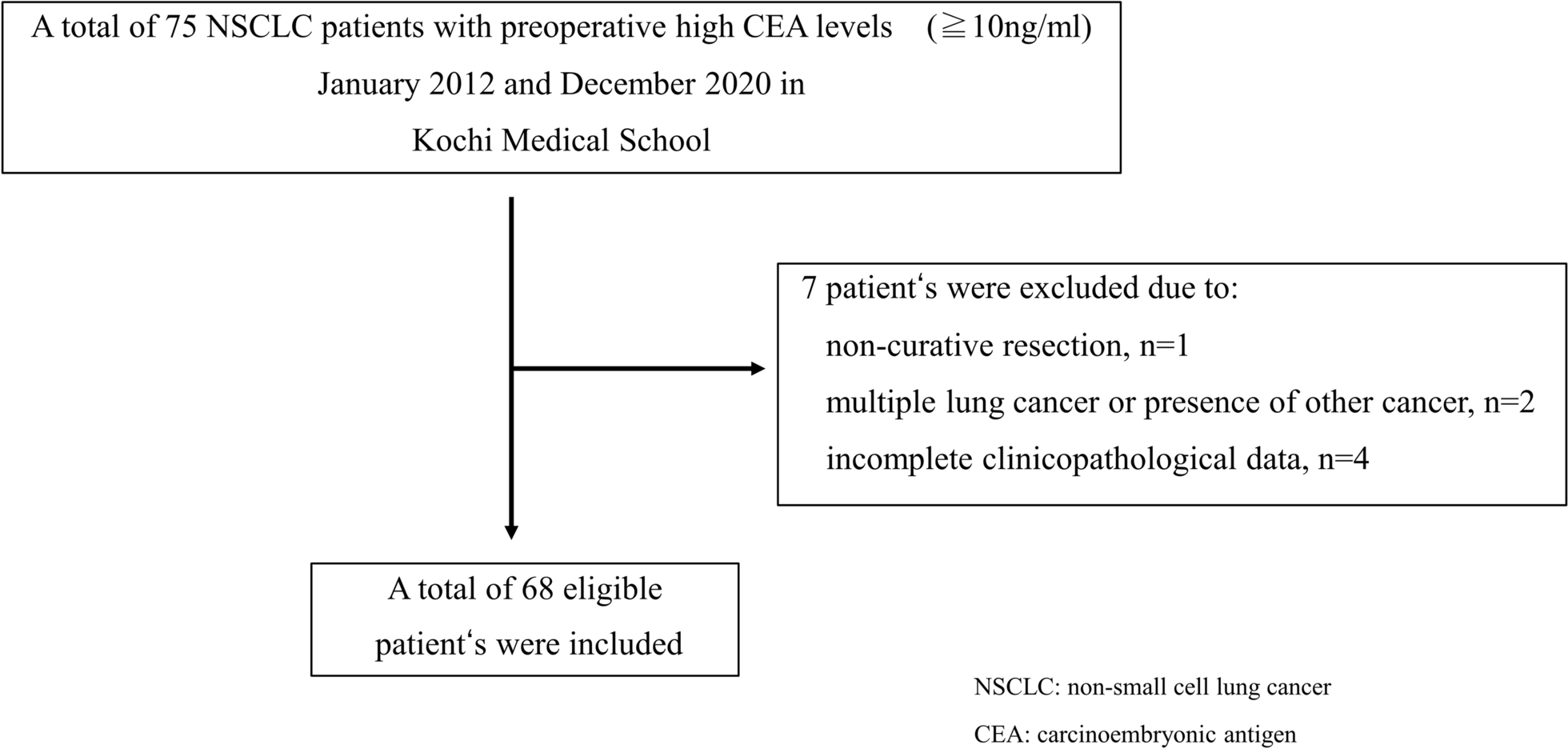
All 62 patients (98.4%) underwent standardization right thoracic incision for thoracoscopic thymic tumors and mediastinal fat resection. Only 1 patient (1.6%) underwent thoracoscopic biopsy because of tumor infiltration into superior vena cava and innominate vein. There were no postoperative severe pulmonary infections, pulmonary embolism, or death; these results were satisfactory. A meta-analysis [14] showed that the operation time was 65–249.8 min, intraoperative blood loss was 92.3-137.5 ml, and postoperative hospital stay was 2.9–10.6 days for minimally invasive thymic operations. Our methods showed that the mean operation time was 57.3 ± 14.2 min, intraoperative blood loss was 22.5 ± 14.7 ml, and postoperative hospital stay was 3.7 ± 1.4 days. No secondary operations were required, and no severe complications or mortality were observed during the perioperative period. We have better performance in the above data, demonstrating that the standardized operation improves the efficiency of the procedure.
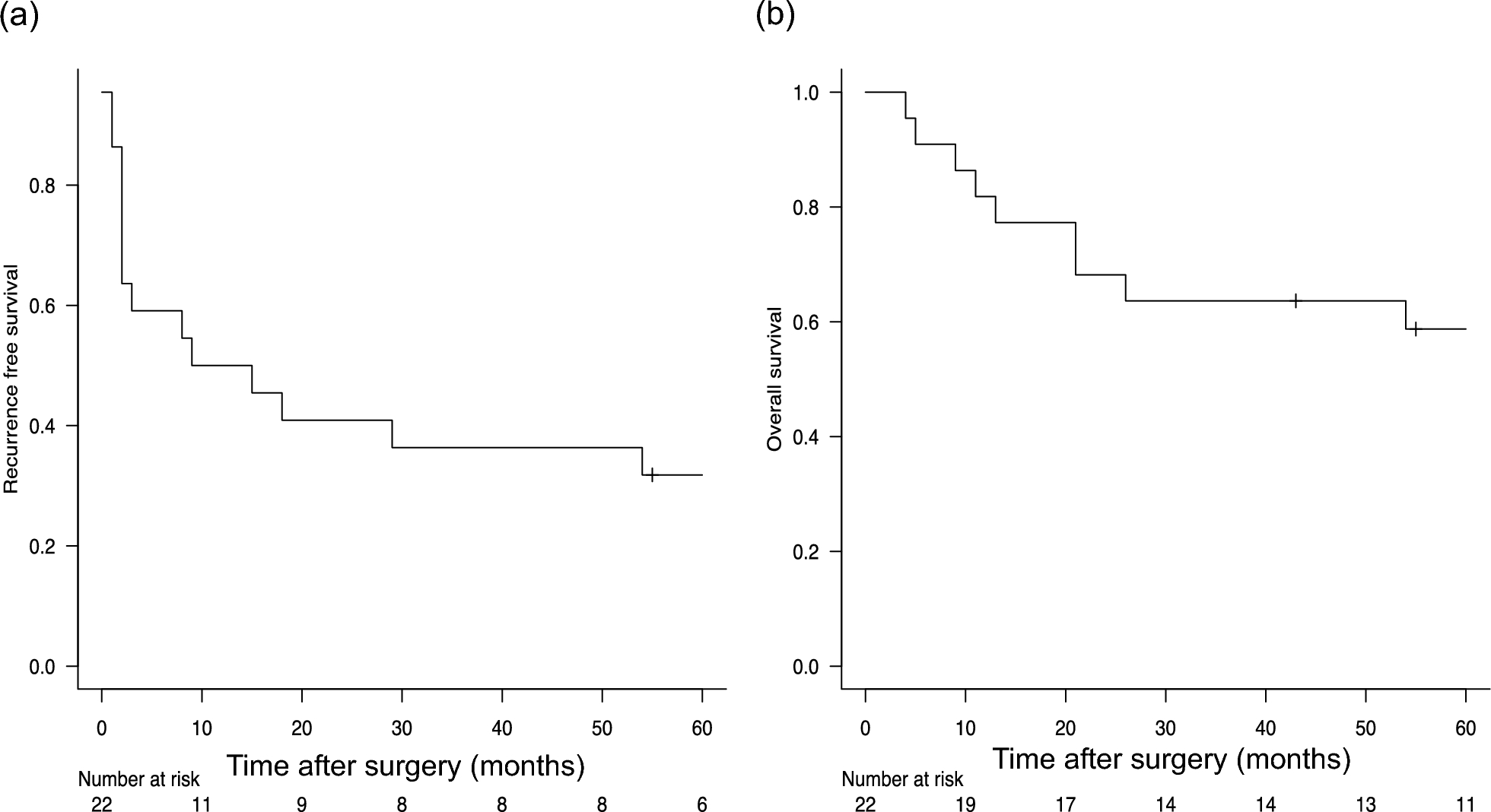
Fifty-three patients were followed up for 6 to 12 months, with no recurrence, metastasis, or death during the follow-up period. Two patients with thymic adenocarcinoma were advised to undergo postoperative radiotherapy, which is considered to have an ideal curative effect and survival rate [16, 17]. With the continuous progress of medical technology, new treatments for thymic adenocarcinoma, such as targeted therapy [18,19,20] and immunotherapy [19, 21], may become important treatments in the future [20,21,22].
Thymectomy, the surgical removal of the thymus gland, can be performed using various techniques, each with distinct advantages and disadvantages. The primary methods include median sternotomy, transcervical approach, video-assisted thoracoscopic surgery (VATS), and robotic-assisted thoracic surgery (RATS). Median sternotomy offers excellent exposure of the anterior mediastinum, facilitating thorough resection crucial for advanced thymomas and thymic carcinomas [23]. However, it is highly invasive, associated with significant morbidity, prolonged recovery times, and increased postoperative pain [23]. The transcervical approach, although minimally invasive and avoiding sternal complications, is limited by restricted exposure, making it less suitable for larger or invasive tumors and presenting a steep learning curve for surgeons [24]. VATS, on the other hand, is less invasive, with reduced postoperative pain, faster recovery, and better cosmetic outcomes [25]. Despite these benefits, it has a limited field of vision compared to open surgery and requires significant expertise, posing challenges for larger or more invasive tumors [25]. RATS enhances precision and dexterity with robotic instruments, providing superior visualization through 3D imaging, but it is costly, less widely available, and demands a steep learning curve with longer setup and operative times [26]. In addition to these methods, some recent studies have introduced hybrid techniques that combine the benefits of different approaches to overcome individual limitations. For example, combining VATS with robotic assistance can leverage the minimally invasive nature of VATS while utilizing the precision and enhanced visualization of robotic systems [26]. This hybrid approach can potentially address the challenges of limited field of vision and improve the resection of complex or larger tumors. Another emerging technique is single-port VATS, which aims to minimize trauma further by using a single incision, thereby enhancing cosmetic outcomes and reducing recovery time [27]. However, these newer techniques require extensive training and have their own set of challenges, including limited instrument maneuverability and increased technical difficulty.
Our standardized right thoracic incision for thoracoscopic thymic tumor resection presents several distinct advantages over traditional methods. The right thoracic approach offers superior exposure of the anterior mediastinum, facilitating thorough resection of thymic tumors and mediastinal fat by avoiding obstruction from the aortic arch and its branches, thereby enhancing operative visibility and precision. This technique is less invasive than median sternotomy, resulting in reduced postoperative pain, shorter hospital stays, and faster recovery with favorable cosmetic outcomes due to smaller incisions. The standardized approach simplifies the procedure, making it easier for surgeons to master. Our data demonstrate that the mean operation time, intraoperative blood loss, and postoperative hospital stay are significantly reduced compared to traditional methods, underscoring the operational efficiency of this technique. Additionally, this method allows for complete removal of thymic tumors and mediastinal fat, which is essential for preventing recurrence and metastasis. The comprehensive nature of this resection is vital for long-term patient outcomes, minimizing the risk of recurrence and ensuring thorough tumor removal. By combining the benefits of minimally invasive surgery with improved exposure and operational efficiency, this approach stands out as a superior alternative to traditional thymectomy techniques. Future studies and long-term follow-up will further validate the efficacy and safety of this technique, potentially establishing it as the gold standard for thymic tumor resection.
To achieve the above results, we used the following management strategies: (1) Consuming more than 300 g of beef per day starting on the first day after the operation can provide a large number of nutrients to promote wound healing and help reduce wound exudation. (2) Patients were instructed to practice coughing and expectoration before the operation, and medical staff and family members helped patients to cough and expectorate after the operation to actively prevent pulmonary complications. (3) Getting out of bed early after the operation: some patients can move their lower limbs on their own in bed for 6 h after the operation, alternating the movement of both lower limbs and strengthening the exercise of getting out of bed on the second day after the operation. For the elderly, they can be accompanied by medical staff and family members. This method can better prevent thrombotic diseases [28]. According to the standardized method for the prevention of postoperative complications, satisfactory results were obtained. We summarized it as “eat well, cough well, exercise well, everyone is satisfied” and referred to it as “three well and one satisfaction” for minimally invasive thoracic surgery and non-esophageal surgery in the perioperative period. We adopted a standardized scheme for operation and perioperative management, optimized the operation process, shortened the operation time, chest tube extraction time, and postoperative hospital stay, and further improved postoperative rehabilitation training. Satisfactory results were achieved.





留言 (0)