Chondrosarcoma is a relatively rare malignant bone tumor with an incidence of approximately 1–2 cases per million people per year in the general population. It originates from cartilage or chondrogenic connective tissue, and is characterized by their production of chondroid (cartilage-like) matrix [6, 7]. The World Health Organization categorizes chondrosarcoma into Grades I to III, depending on their histological characteristics, making it valuable not only as a prognostic indicator but also as a guideline for their management [8]. Chondrosarcoma exhibits low responsiveness to chemoradiotherapy, therefore, R0 resection with a guaranteed negative margin is the preferred treatment.
Costal chondrosarcoma is extremely rare and is mostly reported as individual cases. Only around 40 case reports were found by searching the PubMed and the vast majority of tumors reported were confined to the chest. Dantis et al. [9] reported a similar case with simultaneous involvement of the chest and abdominal wall and emphasized the unique advantages of 3D-composite mesh in reconstructing large-area defects of the chest and abdominal wall. However the clinical challenge was to prevent recurrence and to find better treatment options. Multi-disciplinary discussion, essential for personalized care, ensures a thorough approach to complex cases by facilitating detailed tumor evaluation, critical structure identification, tailored surgical planning, and improves decision-making, outcomes, and surgical safety.
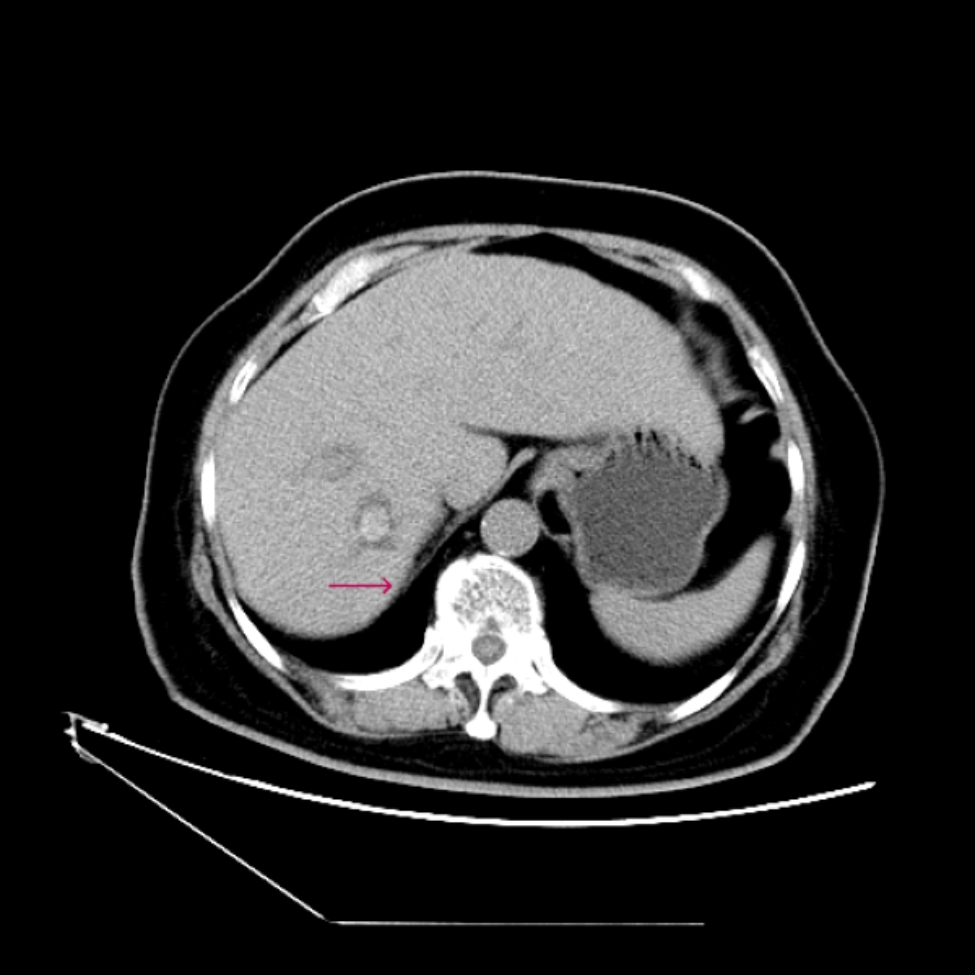
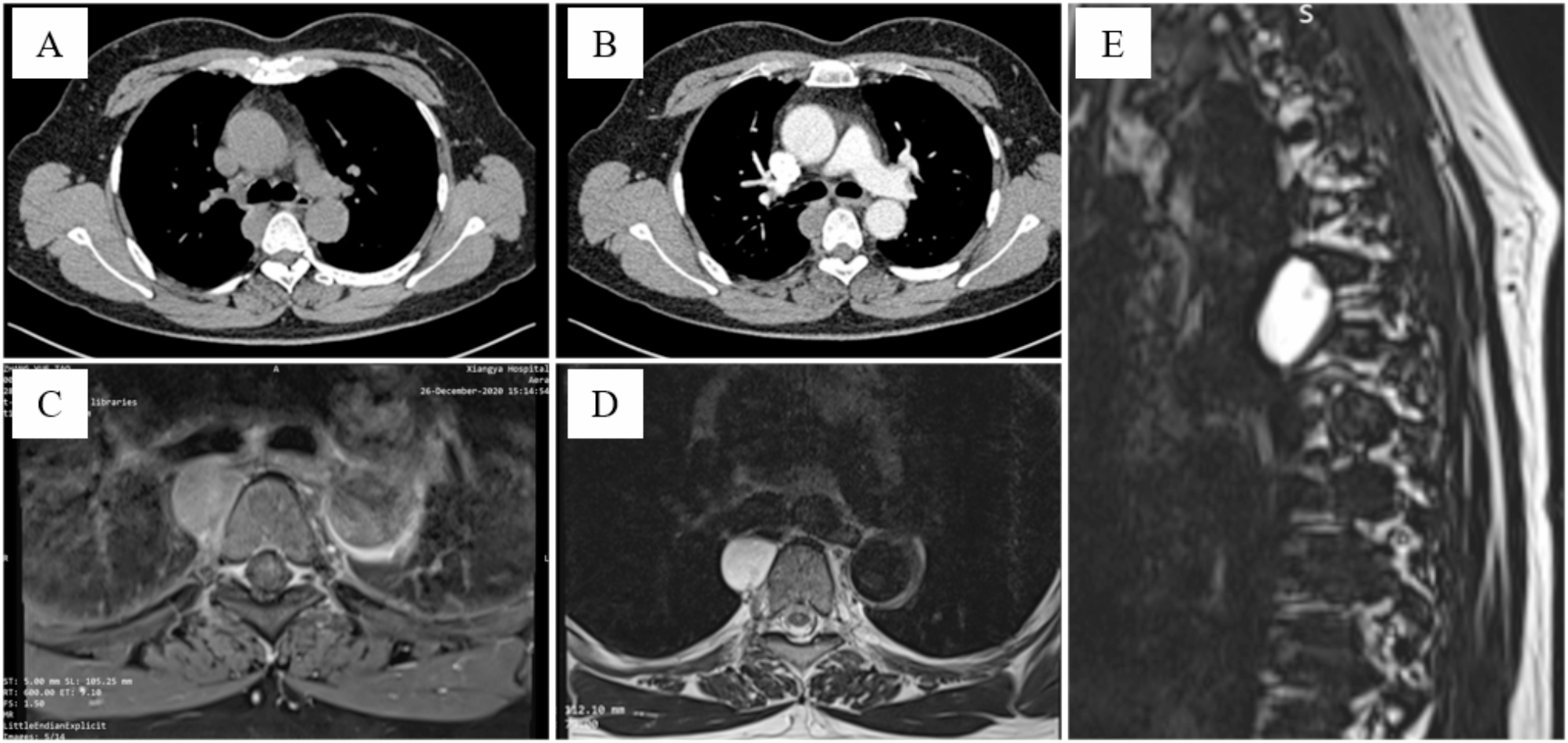
In our case, preoperative multi-disciplinary discussion revolved around diagnosis and detailed surgical planning was conducted. The pathological diagnosis of the tumor was crucial for formulating the surgical plan. Chondrosarcoma was both invasive and metastatic, with its invasiveness and metastatic potential increasing with higher grades. Therefore, surgery must achieve adequate margins and be prepared to excise any invaded tissues. As detailed in the case presentation, an ultrasound-guided biopsy revealed a diagnosis of chondrosarcoma Grade I. Pathologists generally believed that it was impossible to accurately distinguish between benign enchondroma and well-differentiated chondrosarcoma based solely on pathological morphology, whether through needle biopsy or surgical biopsy, because the two shared significant morphological similarities [10]. The differentiation between benign and malignant tumors largely depended on the tumor location, patient age, clinical symptoms, and imaging characteristics. Chondrogenic tumors occurring in long bones, flat bones, vertebrae, and craniofacial bones should be highly suspected of being chondrosarcoma, even in the absence of atypical chondrocytes, if they exhibit the following characteristics: (1) enlargement of the tumor after age 40; (2) pain at rest; (3) a maximum diameter exceeding 5 cm; (4) imaging evidence of bone cortex changes; and (5) MRI detection of periosteal or peritumoral edema [11]. After multi-disciplinary discussions, we unanimously concluded that the diagnosis of costal chondrosarcoma was established, and we speculated that the right kidney might simply be compressed by the tumor. The relationship between the liver and tumor was difficult to judge solely based on imaging data, therefore, collaborative surgery with hepatobiliary surgeons was a necessary condition to ensure complete tumor resection and the integrity of thoraco-abdominal wall reconstruction.
The main purpose of reconstruction is to restore the integrity and stability of the chest wall, to avoid chest wall softening and abnormal breathing, and to ensure the stability of respiratory circulation. Several techniques are commonly employed, each suited to different types of defects. Autologous tissue transplantation is one method used by surgeons to repair defects by utilizing the patient’s own tissues [12, 13]. This method provides a good blood supply to the graft, which reduces the risk of rejection and promotes healing. However, it can increase the risk of damage to the patient during the tissue harvesting process. In cases that require structural support, synthetic materials like titanium mesh or plates are frequently used [14]. These materials offer strong, durable support and possess good biocompatibility, thereby minimizing the risks of infection and displacement. Furthermore, advancements in 3D printing technology [15] have facilitated the creation of customized implants tailored to the patient’s anatomical structure. For more complex defects, a combination of autologous tissue and synthetic materials may be utilized [16]. This composite reconstruction approach balances the need for soft tissue coverage with the requirement for rigid structural support, making it particularly suitable for large or functionally significant defects. The choice of reconstruction technique depends on various factors, including the size and location of the defect, and the functional and aesthetic goals of the surgery. Literature emphasizes the importance of selecting the appropriate reconstruction method to achieve optimal outcomes [14].
In the present case, the 8th to 12th anterolateral ribs were removed, however, we believed that this patient was not suitable for reconstruction using any form of rigid structural support. Firstly, the 8th to 12th ribs were false ribs, the removed ribs had little impact on respiratory movement. Secondly, most of the defects were located on the abdominal wall. Finally, it was challenging to form a stable connection between the ribs, the support structure, and the diaphragm. Repeating friction might cause patient discomfort, displacement or dislodgement, and even damage to surrounding organs. So we sutured the diaphragm to the ribs and intercostal muscles at the resection margin, using a polypropylene mesh to reconstruct the defects. Although this may lead to a little reduction in the chest cavity volume and make the reconstructed area essentially become part of the abdominal wall, it nonetheless guarantees the stability of the chest wall and minimizes the likelihood of complications stemming from complex reconstruction. Moreover, the combination of the mesh and a relatively thick flap fully meets the reconstruction requirements of the“abdominal wall”. If resource constraints and cost-effectiveness are not considered, replacing polypropylene mesh with advanced ones would result in a more perfect reconstruction outcome.
The patient’s postoperative course was uneventful, and was discharged without any complications. Histopathological analysis confirmed the complete removal of the tumor with negative margins. We did not recommend any further treatment for this patient because, on the one hand, the tumor was of low malignancy grade, and on the other hand, we achieved complete R0 resection. According to guidelines [17] and literatures [7, 18,19,20], treatments such as radiotherapy, chemotherapy, checkpoint inhibitors, and targeted drugs are primarily used when tumors are inoperable, metastatic, or recurrent. However, there is still insufficient data to support their routine use as adjuvant therapy following surgery in cases of chondrosarcoma Grade I-II. However, we require the patient to undergo a chest X-ray or CT scan every six months for the first five years, and then annually thereafter.





留言 (0)