
記住我




In our study, 7 were males and 5 were females, aged 25–75 years (53.0 ± 17.0 years), and 5 were older than 65 years. The mean Body Mass Index(BMI) was 20.5 ± 3.0 kg/m2, and 11 (91.7%) patients had a BMI of less than 25 kg/m2. A history of breast tumor surgery in 1 patient, and all the other patients were healthy.
Lung surgery was performed on all 12 patients. The indication for surgery was pulmonary nodules detected by physical examination in 11 patients (91.7%), and the diameter of pulmonary nodules ranged from 6.0 to 41.0 mm(22.3 ± 12.7 mm); The indication for surgery was pulmonary bullae in 1 patient(8.3%)(radical resection of esophageal cancer was performed at the same time as resection of pulmonary bullae in this patient). 6 patients underwent lobectomy, 4 patients underwent segmentectomy, 1 patient underwent wedge resection, 1 patient underwent wedge resection, 1 patient underwent radical resection of esophageal carcinoma combined with resection of pulmonary bullae.
The pathological findings were pulmonary malignancy in 9 patients(75.0%), and benign disease in 3 patients(25.0%). Carcinoma in situ with microinfiltration was found in 3 patients; Squamous cell carcinoma in 3 patients, among them, stage IA, IIB and IIIA were in 1 patient respectively; Adenocarcinoma in 3 patients, among them, stage IA, IIA and IIIA were in 1 patient respectively. In 3 patients with benign pulmonary disease, 1 patient underwent radical resection of esophageal carcinoma and resection of pulmonary bullae at the same time.
Diagnosis of PAL after pulmonary surgeryAll the 12 patients were observed with newly emerging symptoms of cough, sputum, fever, and dyspnea, as well as abnormal channel or increased gas in the pleural cavity or the new liquid-gas level on chest CT, and were diagnosed with PAL after pulmonary surgery with the help of bronchoscopy. The bronchopleural fistula were found in 7 patients under bronchoscopy, of which the location of fistula orifices were determined indirectly by Chartis system, continuous continuous balloon occlusion and stain in 3, 2 and 2 patients, respectively; And 1 of these patient was diagnosed with the fistula of bronchi, pleural cavity and stomach by bronchoscopy and gastroscopy. The fistula orifice were found in 5 patients under bronchoscopy directly with the diameter of 4.0–12.0 mm(7.2 ± 3.6 mm), of which fistula orifice was located above the tracheal carina in 1 patient, and the fistula orifices were located at the surgical stump in 4 patients (Table 2).
Table 2 Diagnosis, therapy, and prognosis of patients with PALTherapy of PAL after pulmonary surgery(1)Therapy of complications: (i) Chest tube drainage combined with negative pressure suction: Of the 12 patients, 9 patients were performed chest tube drainage, and 3 patients were not performed chest tube drainage; In patients undergoing chest tube drainage, chest tubes (size of chest tube: 18f(french)-26f) were performed in 8 patients when PAL were identified immediately, and chest tube was performed 1 patient (size of chest tube: 8f) during the respiratory endoscopy intervention; According to the Cerfolio criteria, the severity of air leakage was all grade 4 in patients with chest tube drainage. (ii) Medical thoracoscopy with chest tube as a path: At least once medical thoracoscopy(with chest tube as a path) was performed in 7 patients with large diameter of chest tubes (Table 2).
(2)Therapy of fistula orifice (Fig. 4a-f): Among the 7 patients with bronchopleural fistula, 1 patient received C + D, 1 patient received A + B + C, 1 patient received the A + C + D, 4 patients received A + B + C + D; Among the 5 patients with fistula orifice, 2 patients received C + D, 2 patients received A + B + D, 1 patient received A + C + D (Table 2). The course of therapy is shown below in this special patient who underwent radical resection of esophageal cancer combined with resection of pulmonary bullae (Fig. 5a-f).
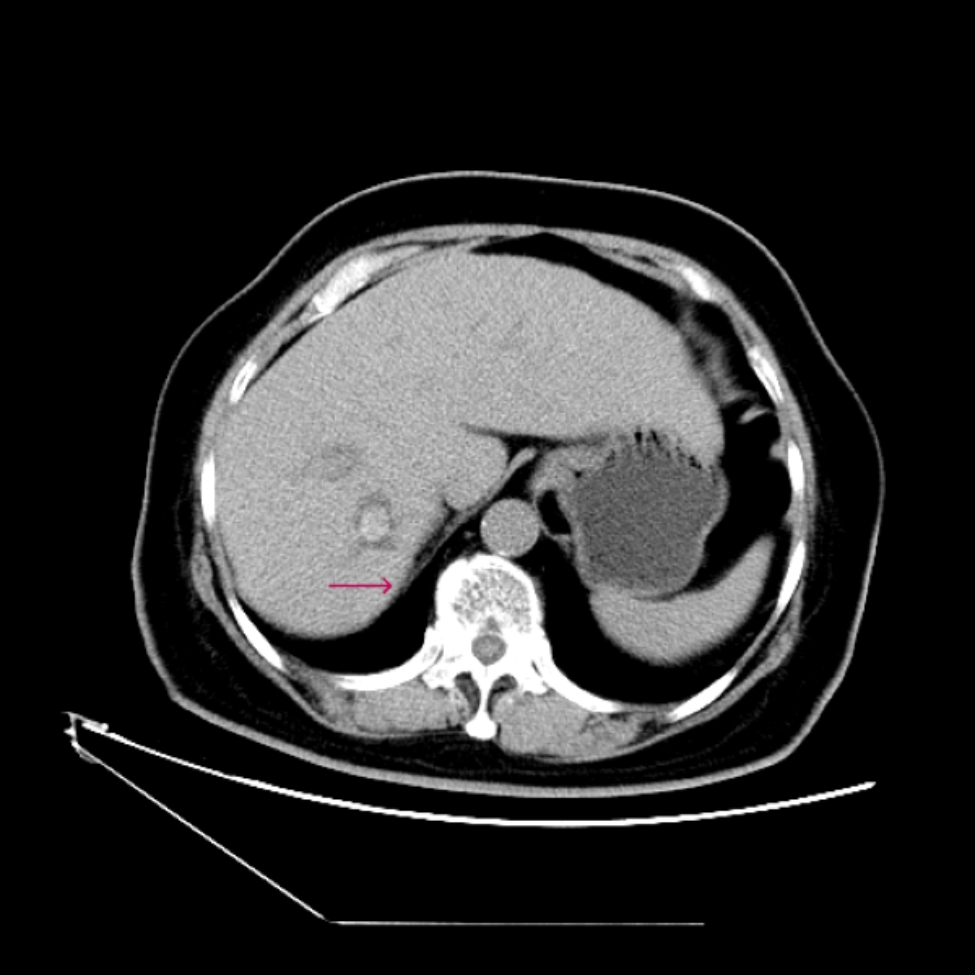
Fig. 5
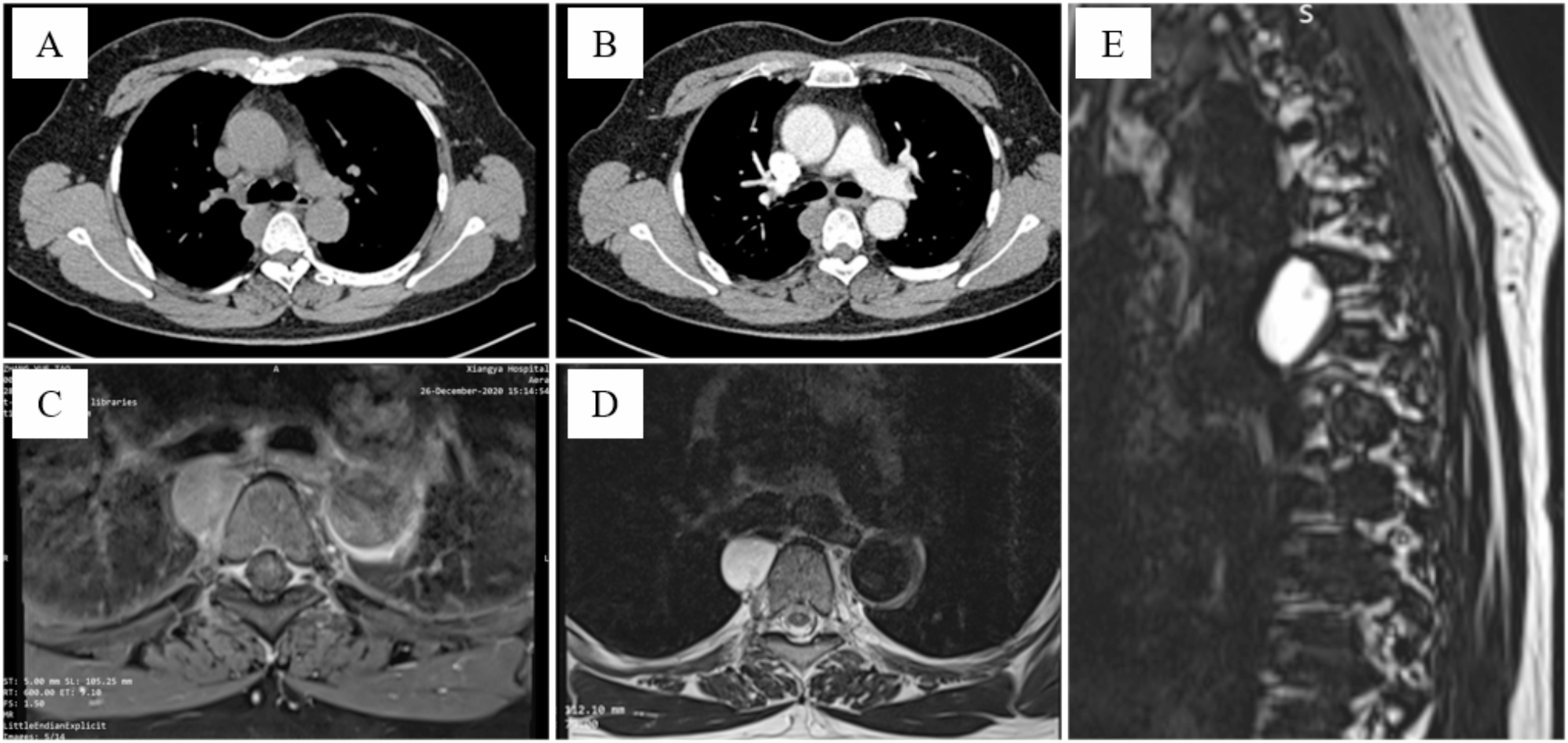
The course of therapy of the patient with the fistula of bronchi, pleural and stomach after radical resection of esophageal cancer and resection of pulmonary bullae. (a) An abnormal channel of bronchi, pleural cavity and stomach in the lung window of chest CT; (b) An abnormal channel of bronchi, pleural cavity and stomach in the mediastinum mediastinum window of chest CT; (c) A gap in the stomach can be seen under gastroscopy and stain was released through the gap under gastroscopy; (d) The outflow of staining from the apical and anterior segments of the upper lobe of the right lung was observed under bronchoscopy; (e, f) Inverse EBV valves were retrofitted into the apical and anterior segments of the right upper lobe, respectively, and successful blocking of the fistula orifice was confirmed under combined bronchoscopic and gastroscopic examination
(3)Empirical anti-infective therapy or anti-infective therapy was based on the results of sputum culture and pleural effusion culture.
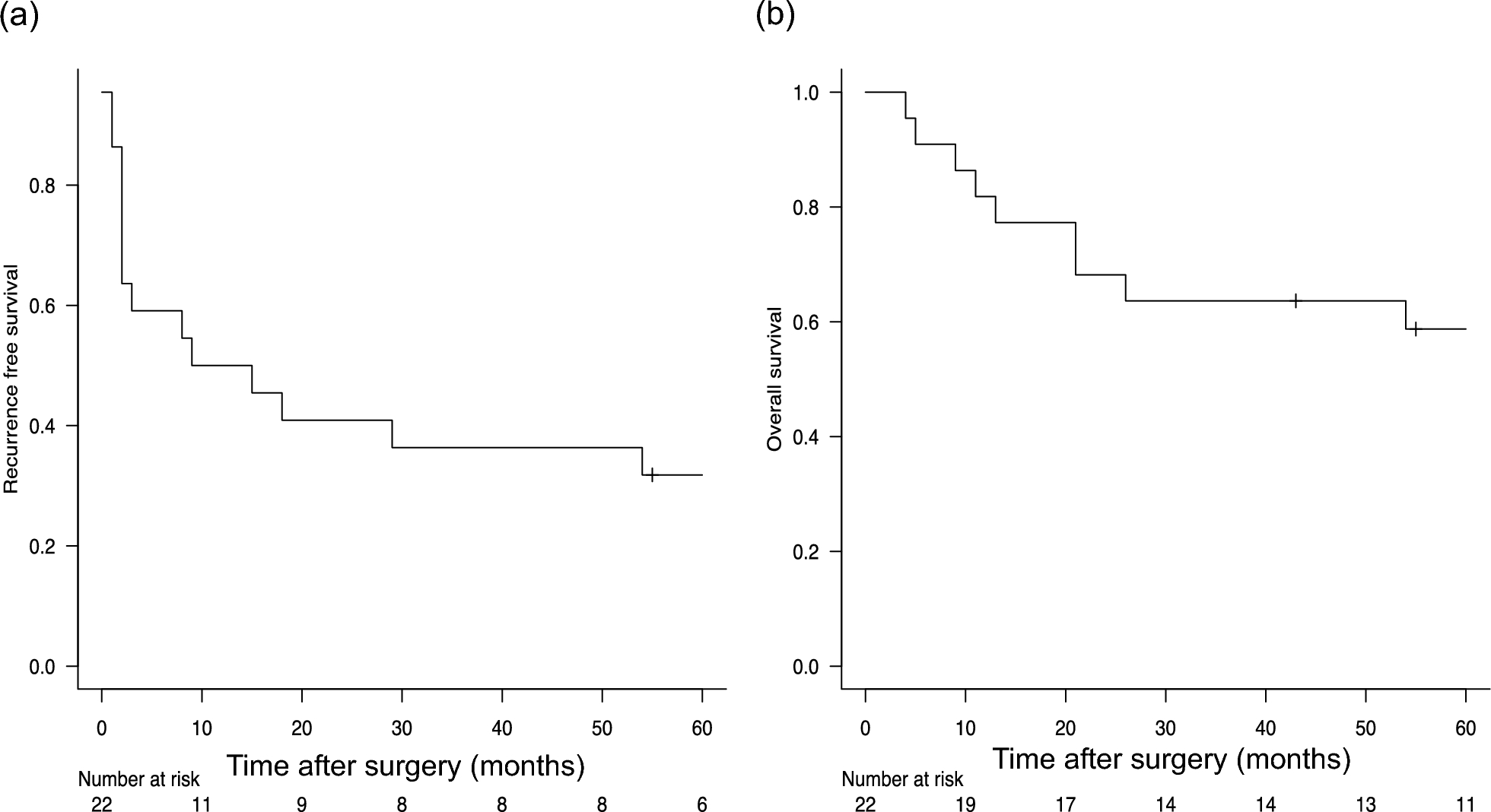
Effect of therapy(1)From the time of last respiratory endoscopy intervention to 8 April 2024, the 3 patients without chest tube drainage were followed up for 9.4 months, 11.4 months and 0.9 months, respectively; In addition, gradual resorption or blocking of the fistula orifice under endoscope or gradual absorption of the residual dead space under examination of imaging were observed in these 3 patients. 9 patients who underwent chest tube drainage were successfully extubed, the retention time of the chest tubes was 10–173 days, with a median (interquartile distance) of 94 (72,124) days, and the follow-up was 7.6-37.4months after extubation; Among these 9 patients, only 1 patient relapsed after receiving programmed cell death protein 1(PD-1), and gradual absorption or vanish of the residual dead space under examination of imaging were observed in remaining 8 patients during the follow-up (Table 2).
(2)Chest tube drainage were performed in 8 patients when PAL were identified at once, and the median (interquartile distance) retention time of chest tubes before and after our protocol of respiratory endoscopy intervention were respectively 73.5(50.5,106.25) days and 29(22,38.75) days, p < 0.05 (Fig. 6).
Fig. 6
Comparison of the retention time of chest tubes before and after respiratory endoscopy intervention(*: p < 0.05)
留言 (0)