
記住我
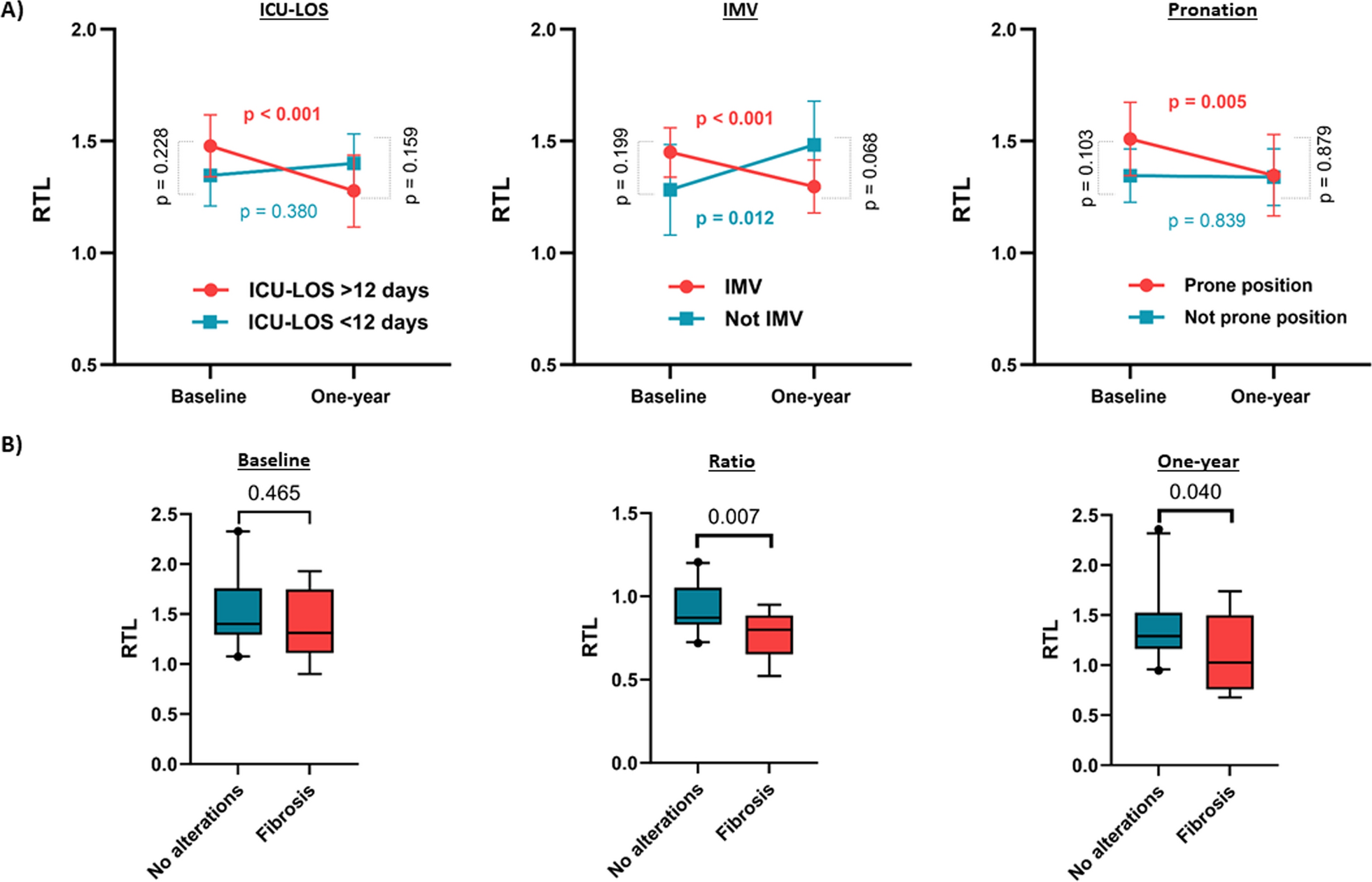

5 key-points are essential in the EMS treatment of patients with (central) stab wounds. They can be remembered by the STAB-5 mnemonic (Fig. 1).
Fig. 1 Scene safety
Scene safetyTraditionally, EMS crews are trained to follow a classic approach to scene safety, accessing scene only when deemed safe by the police [3]. In the evolving landscape of emergency response, a shift towards the concept of dynamic risk assessment is emerging worldwide. This approach emphasises the importance of scene assessment by EMS personnel and their ability to swiftly adapt to evolving situations to prevent a therapeutic vacuum.
TriageImmediately after arrival, crews should establish the location and the severity of the injuries sustained. This should be done succinctly to prevent attention being drawn towards the most obvious injury whilst other sources of significant bleeding or injury are neglected. Clothing should be cut-off to facilitate a quick full-body examination, especially of often neglected areas such as axillae, groin, gluteal cleft and perineum, whilstcare should be taken to maintain dignity to the patient when performing these examinations.
Assertive scene & patient managementAn early request for critical care teams capable of performing advanced interventions such as blood transfusion or resuscitative thoracotomy should be made, but crews should NOT wait on scene for their arrival. Focus should be on advancing towards the nearest Major Trauma Center (MTC) unless the patient is peri-arrest (agonal breathing, barely recordable pulses), where diverting to the nearest (trauma) hospital is appropriate. If available and deemed necessary (depending on distance from hospital and the patient’s condition), a Rendezvous Point (RVP) with a criticalcare team can be established en route to hospital. Early communication with dispatch regarding the destination hospital and planned rendez-vous points are key in these instances.
Bleeding controlDirect pressure, wound packing and tourniquet application are the mainstem of bleeding control. In catastrophic extremity bleeding, a tourniquet should be applied immediately and tightened sufficiently to stem arterial bleeding. A second tourniquet may be required if the bleeding continues. Some wounds require packing in addition to direct pressure. The bleeding vessel should be located within the wound, and hemostatic gauze applied directly to the source of the bleed, packing tightly until the wound is filled to provide sufficient pressure. A pressure bandage can then be applied over the top of the haemostatic gauze. For neck wounds direct pressure should be maintained and the need for (early) airway interventions should be considered.
5-min scene timeEMS focus should be to provide immediate life-saving interventions and leave scene towards definite care within 5 min. Patients should be assisted to walk to the ambulance where possible or rapidly extricated by carry-chair or stretcher if necessary. All emphasis should be upon leaving scene with a shared understanding that most intervention can be performed en route to hospital. If vascular (IV/IO) access cannot be gained immediately, additional attempts can be made on route if safe to do so. Tranexamic Acid (IV or IM if no access can be obtained), analgesia and basic monitoring can all be managed en route to hospital and if no reliable blood pressure readings are generated, the patient’s volume status should be assessed and described by peripheral pulses, colour, diaphoresis and respiratory status.
留言 (0)