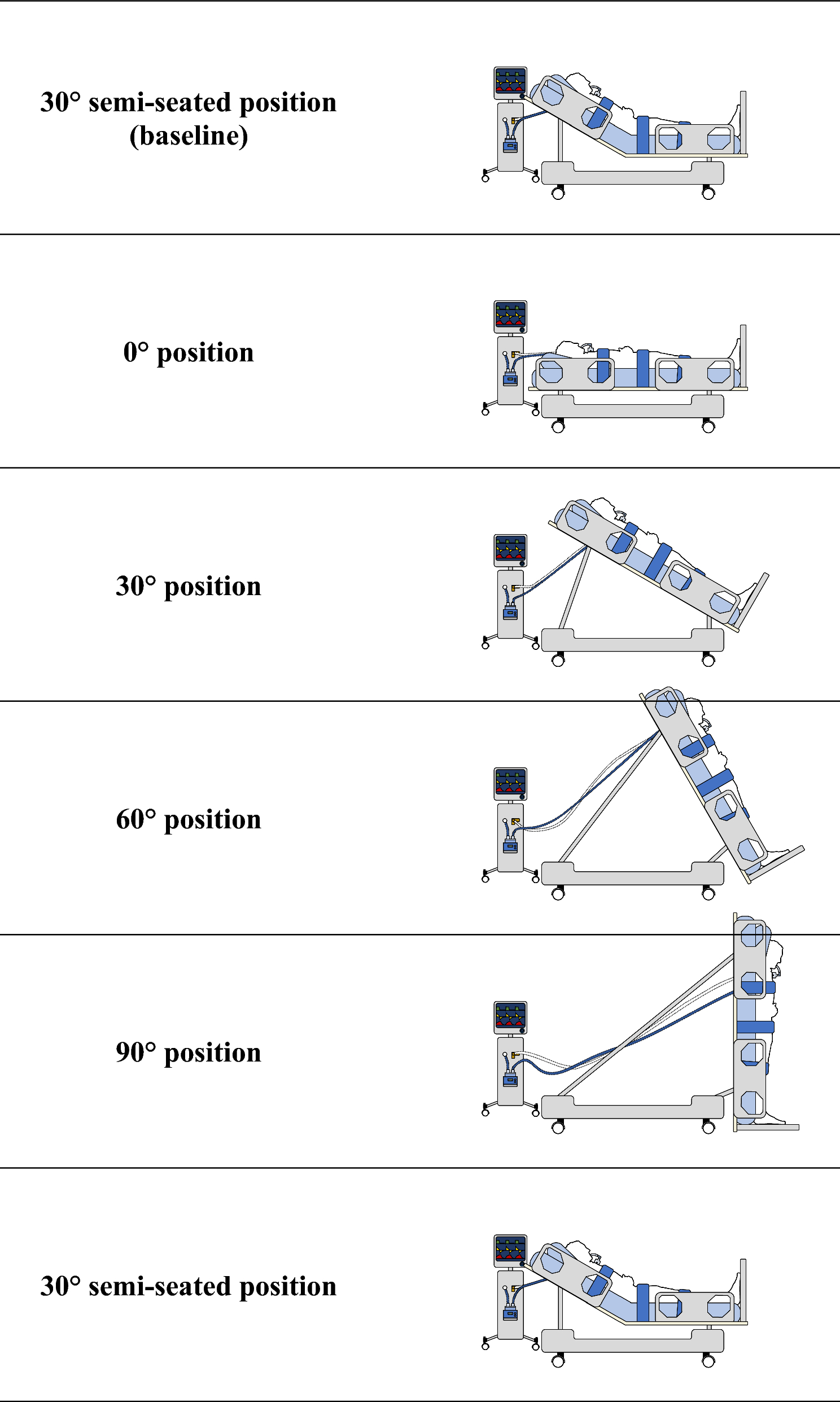
In this study, verticalizing the bed from a flat 0° position to a fully vertical 90° position resulted in several notable respiratory and hemodynamic effects. The primary findings indicated that verticalization from 0° to 60° increased ΔPL and EELV, decreased CCW and increased both PaCO2 and the PaO2/FiO2 ratio. Additionally, verticalization led to decrease in cardiac output with several serious hemodynamic event. However, it is important to note that these effects did not change significantly with further verticalization beyond 60°.
This pioneering study provides new insights into the direct influence of progressive verticalization on respiratory mechanics, oxygenation, and, fundamentally, on hemodynamic changes. The results underscore the necessity of balancing improved oxygenation with potential adverse effects on respiratory mechanics and hemodynamics when determining the optimal angle of bed inclination for patients.
Effects of verticalization on pulmonary mechanics (0 to 90°)
Studies have shown that shifting from a semi-recumbent to a supine-flat position in ARDS patients under mechanical ventilation significantly affects respiratory mechanics. Marrazzo et al. demonstrated that changing trunk inclination from 0° to 40° increased driving and transpulmonary pressure while decreasing both CL and CCW in two studies on 20 COVID-19-associated ARDS [1, 2]. Mezidi et al. found that moving from a supine-flat to a 30° semi-recumbent position significantly reduced EL and ECW in ARDS patients [20]. These results are consistent with our study, where progressive verticalization deteriorated pulmonary mechanics with or without hip flexion [1, 2, 10, 20].
At 0°, the kinetic energy from the ventilator was mainly directed to the lungs, but with significant redistribution to the chest wall during verticalization (Supplementary Material 1: Appendix Figures E7). Mechanical power increased without changes in PEEP, VT, respiratory rate, or resistance, correlating with EL/ERS and ECW/ERS ratios between 30° and 60° (Pearson coefficient = 0.5, P < 0.05). These findings suggest that verticalization increases intra-abdominal pressure, affecting ventilatory mechanics. Literature indicates that the increase in ECW may result from thoracic compression due to abdominal organ displacement [6,7,8,9]. The thoracic support strap used for patient safety may also have decreased CCW.
PEEP may have influenced the observed changes. In our study, PEEP was set at 30° semi-seated baseline position and not modified. At 0°, lung collapse areas may appear, while with verticalization, alveolar overdistension areas may develop [20]. Verticalization combined with optimized PEEP, could mitigate these effects by operating within a more favorable range of pressure–volume curves, reducing lung stress and strain.
Effects of verticalization on EELV (0 to 90°)
Bed verticalization from 0° to 30° and from 30° to 60° significantly improves EELV, with no further improvement from 60° to 90°. Strain decreases significantly only from 0° to 60°. This may be due to regional lung volume redistribution caused by gravity, enhancing dependent lung region expansion and alveolar recruitment. However, increased ΔPL suggests possible associated overdistension, supported by other parameters we observed, such as increase in PaCO2 from 30° to 60°.
These findings align with literature indicating that EELV and oxygenation improvements during trunk inclination in certain responsive ARDS patients can be accompanied by overdistension [3, 4] [5].
Effects of verticalization on oxygenation and shunt (0 to 90°)
As in the studies by Richard et al. and Dellamonica et al., oxygenation improved significantly with verticalization [3, 4] from 0° to 30°, accompanied by a comparable improvement in pulmonary shunt for the same inclinations. Aligning with EELV increase from 0° to 30°, this may reflect alveolar recruitment combined with pulmonary blood flow redistribution during verticalization. This supports the observations by Gattinoni et al. who studied the effects of PEEP and showed that its increase improves oxygenation by reducing shunt, partly through blood flow redistribution to better-ventilated areas [21]. The reduction in pulmonary shunt can also be attributed to the decreased cardiac output observed up to 90°. Indeed, Dantzker and Lynch demonstrated that reducing cardiac output decreases pulmonary shunt by reducing perfusion in low V/Q areas, thus improving oxygenation [22, 23].
Conversely, we did not observe additional benefits in terms of oxygenation and shunt beyond 30°, suggesting diminishing or compensating effects. Beyond this angle, the increase in EELV may reflect overdistension, reducing regional pulmonary blood flow through capillary compression, and thus decreasing oxygenation efficiency. Pulmonary blood flow redistribution might lead to a V/Q mismatch if well-ventilated areas are not adequately perfused [24, 25]. Additionally, these phenomena can be exacerbated by decreased venous return and cardiac output during verticalization, which can reduce pulmonary perfusion and counteract the benefits of alveolar recruitment [26, 27].
Effects of verticalization on PaCO2 and ventilatory efficiency (0 to 90°)
The increase in PaCO2 observed from 0° to 60° can be attributed to a combination of overdistension and redistribution of pulmonary blood flow, as suggested by previous observations and literature [26, 27]. Additionally, the reduction in venous return and cardiac output can decrease the alveolar perfusion, thus altering CO2 elimination (VCO2). We did not observe an increase in the VD/VT ratio, but it is possible that the decrease in VCO2 and FeCO2 we observed, although not significant, mitigates this phenomenon. Indeed, according to the equation we used, neither the respiratory rate nor the VT has varied significantly. Furthermore, we are limited to an overall analysis of ventilatory efficiency, which results from a combination of regional phenomena of alveolar recruitment and overdistension, involving the reaeration of initially poorly ventilated areas and increased trapping in already well-ventilated areas.
Finally, the estimation of VD/VT with this formula requires homogeneous ventilation and perfusion, which is rarely the case in patients with ARDS. Additionally, variations in cardiac output, intrathoracic pressures, and pulmonary shunt can influence parameters such as PaCO2, VCO2 and FeCO2, making the estimation of VD/VT less precise, as demonstrated in studies by Dianti and Beitler. [28, 29].
Effects of verticalization on hemodynamics (0 to 90°)
Verticalization adversely affects hemodynamics, decreasing cardiac output and stroke volume at each stage. Reduction in venous return due to blood volume redistribution to lower body regions is a most apparent cause [30]. Norepinephrine increased from 30° to 90°, while MAP decreased between 0° and 60° despite following the study’s hemodynamic protocol, highlighting the potential challenges for hemodynamic management. Moreover, two patients exhibited hemodynamic instability at 90°, requiring experimental procedure interruption.
We also observed a decrease in RAP, PAP, and PAOP, along with an increase in PVR. First, the decrease in cardiac output may trigger autoregulatory mechanisms in the pulmonary circulation. The inverse correlation between the variation in CO and that of PVR that we observed from 0° to 30° (Pearson = 0.6), from 30° to 90° (Pearson = 0.8), and from 60° to 90° (Pearson = 0.6) (P < 0.05) (Table E7), strongly supports this hypothesis. As described by West and Dollery, the reduction in pulmonary blood flow is accompanied by an increase in PVR due to compensatory pulmonary capillary vasoconstriction, and a decrease in PAP if this mechanism is overwhelmed, especially in ARDS cases [31, 32]. Overdistension may also play a role by increasing the compression of small capillaries [33]. This idea is supported by the increase in ΔPL we observed, which could explain the increase in PVR and the decrease in PAOP, as proposed by Permutt et al., with a more pronounced effect when cardiac output is reduced [34]. Verticalization may also induce a decrease in PAP through reduced venous return due to blood volume redistribution [30], which appeared as a significant decrease in RAP up to 60° in our study. Lastly, the increase in thoracic pressure could also play a role. Although it does not seem to have a direct impact on PAP in spontaneous breathing according to a physiological study on horses [35], increased pleural pressure can cause mediastinal compression in mechanical ventilation, contributing to reduced venous return [32].
Finally, it is important to consider these hypotheses carefully, as the patients were not in a normal physiological state. The interaction of numerous mechanisms, such as verticalization, hemodynamic variations, and changes in pulmonary mechanics, along with the implications of ARDS, significantly complicates the interpretation of our results.
Limitations
First, the evaluation time per phase was relatively short, which may have limited the effects of patient positioning at each step. Second, the position sequences were not randomized, and patients were not returned to the initial position between each step, introducing a potential risk of a cumulative carryover effect, making the specific and independent effects of each position unclear. Third, the small sample size could limit the generalizability of the results. Fourth, the potential displacement of the esophageal probe during the verticalization could have led to loss of its initial calibration and measurement inaccuracies. Fifth, prior optimization of ventilation parameters and lung aeration, notably with PEEP titration following a standardized alveolar recruitment maneuver, might have minimized the current results. Finally, the majority of patients included in this study had COVID-19-associated ARDS, making it uncertain if these results are applicable to other ARDS populations.
Strengths
First, it is the first to investigate the effects of bed verticalization up to 90°, with legs extended, in patients with ARDS. Verticalization procedures have already been proposed but were limited to the 60° seated position [3, 4] and did not include evaluation of the transpulmonary driving pressure, pulmonary artery measurements, or pulmonary shunt fraction. Second, our study confirmed the simplicity and feasibility of verticalizing ICU patients, although such current hypothesis-generating results raise potential hemodynamic concerns.


留言 (0)