
記住我

In total, 2720 TB HCWs were included in the final analysis, 1270 from PHC sectors at community level and 1450 from PHC sectors at village level (Table 1). More than half of HCWs attended junior medical college in communities and technical secondary school or below in villages. The majority of both community and village HCWs had medical education backgrounds (89.8% and 84.1%, respectively). The income of community HCWs was higher than that of village HCWs. Moreover, most HCWs had low professional titles, 84.6% and 94.1% of community and village HCWs had non/junior titles respectively. A larger proportion of village HCWs were undertaking more than 5 BPHS programs compared with community HCWs (75.4% vs 29.1%), and a greater proportion of village HCWs had longer working years than community HCWs. As for working satisfaction and willingness, less than 50% of both community and village HCWs were satisfied with TCP implementation, and more community HCWs had low working willingness (40.0%) than village HCWs (25%). Eventually, 20 interviewees participated in the in-depth interviews. This included 7 TB HCWs (3 from community areas and 4 from village areas), 4 TB patients (2 with DS-TB and 2 with DR-TB), and 9 health care leaders (6 from CDC and 3 from the Health Commission). The demographic characteristics of the interviewed HCWs matched those of the surveyed HCWs. All four interviewed TB patients had completed treatment. Of the nine health care leaders interviewed, five held a deputy senior title, and all had at least three years of administrative working experience in TB-related fields.
Table 1 Demographic and working characteristics of TB HCWs in PHC sectors in West China, n (%)Training and TB knowledge of TCP among HCWs in PHC sectorsTraining for TCP implementation was carried out among HCWs in PHC sectors (Table 2). The majority of both community HCWs (48.0%) and village HCWs (34.6%) had received training less than once half-year. They mainly obtained training through offline lectures/meetings or a combination of offline and online methods. More than 80% community and village HCWs preferred to have training content on TB knowledge, skills of treatment management for TB patients, referring suspicious TB patients, health education on TB knowledge, and close contacts screening and tracing. Though around 90% HCWs in PHC sectors were satisfied with training, knowledge about TCP implementation among both community and village HCWs were low (Table 2), with an overall score of 12.945 and 12.185 respectively, less than half of the total score of 30.
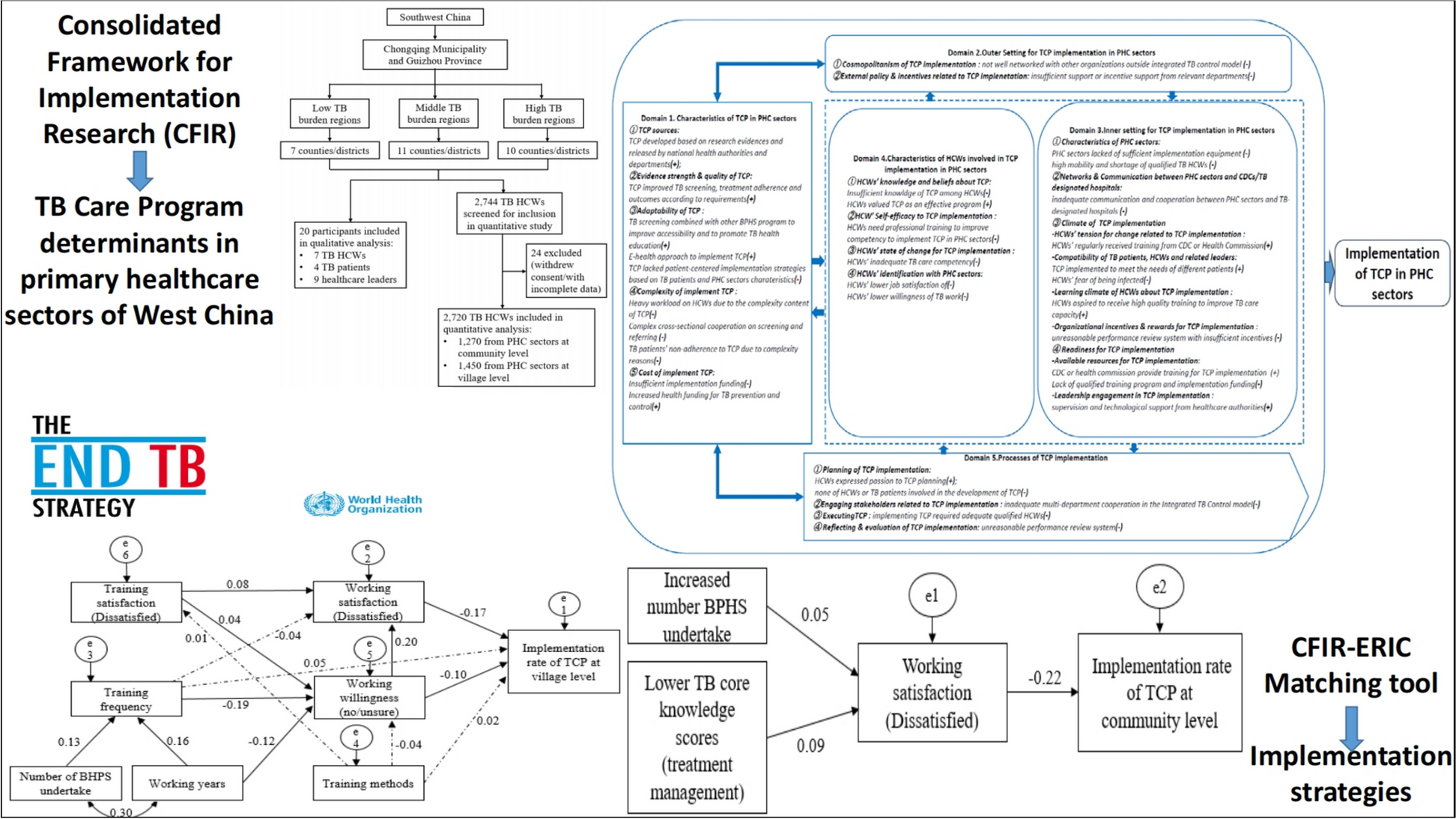
Table 2 Training and knowledge about TCP among TB HCWs in PHC sectors in West China, n (%)TCP implementation in PHC sectors and associated factorsDespite the higher implementation rate of TCP in urban regions (84.4%) than in rural areas (79.3%), the implementation status of 10 categories in TCP was similar in both settings (Table 3). Six categories showed a relatively better implementation status: TB prevention services for the publics, TB care services during the first-time follow-up visit for patients, health education for TB patients, follow-up evaluation and intervention for TB patients, case closed assessment for TB patients, and TB prevention services for patients’ family members. Conversely, four categories had a relatively low implementation rate: TB prevention services for high-risk populations, referred suspicious TB patients, treatment management for TB patients, and other services for TB patients. At the community level, regarding the path analysis of TCP implementation, 12 variables were determined after controlling demographics variables, including number of BPHS undertake, training frequency, working satisfaction, working years, training methods, training satisfaction, and TB core knowledge total scores. The fitting result of the path model concerning the implementation of TCP at both community and village levels indicated a good degree of fit (Table 4). The fitting result of the model is: χ2 = 5.068, P = 0.167, df = 3, χ2/df = 1.689 < 3, NFI = 0.936 > 0.9, RFI = 0.901 > 0.9, IFI = 0.973 > 0.9, TLI = 0.944 > 0.9, CFI = 0.972 > 0.9, RMSEA = 0.024 < 0.05. As shown in Fig. 3, low job satisfaction (-0.22) is a barrier for the implementation of TCP; increasing number BPHS undertake (-0.05) and lower TB core knowledge scores (treatment management) (-0.09) are indirect barriers for the implementation of TCP at community level.
Table 3 Implementation rate of TCP among TB HCWs in urban and rural settings in West China, n (%)Table 4 Fitting results of path analysis in TCP implementation at community and village levels in West ChinaFig. 3
Path model of TCP implementation in PHC sectors at community level. Note: the solid line represents the path coefficient P < 0.05, and the dashed line represents the path coefficient P ≥ 0.05. BPHS Basic public health service; TB Tuberculosis; TCP Tuberculosis Control Program; PHC Primary healthcare; HCWs Healthcare workers
At village level, after controlling for demographic variables, based on the results of multiple regression analysis and correlation analysis, 14 variables were identified in the path analysis of village TCP implementation, including number of BHPS undertake, working years, training frequency, training methods, training satisfaction, working satisfaction, working willingness, and TB core knowledge scores. The fitting result of the path model is: χ2 = 15.570, indicating that the model is well adapted to the actual observation data, P = 0.212 > 0.05 indicating that the model has good adaptability, df = 12, χ2/df = 1.297 < 3, NFI = 0.967 > 0.9, RFI = 0.923 > 0.9, IFI = 0.992 > 0.9, TLI = 0.981 > 0.9, CFI = 0.992 > 0.9, RMSEA = 0.014 < 0.05. As shown in Fig. 4, in terms of direct effects, low working satisfaction (-0.17) and low working willingness (-0.10) are barriers for the implementation of TCP at village level. As for the indirect effects, increased training frequency and working years are enablers for the implementation of TCP at village level, while low training satisfaction (dissatisfaction) is a barrier.
Fig. 4
Path model of TCP implementation in PHC sectors at village level. Note: the solid line represents the path coefficient P < 0.05, and the dashed line represents the path coefficient P ≥ 0.05. TCP Tuberculosis Control Program; PHC Primary healthcare
The path analysis indicated major barriers including low job satisfaction, TB core knowledge, working satisfaction and working willingness need urgent interventions to address.
Qualitative results on factors of TCP implementation in PHC sectorsFactors of TCP implementation in PHC sectors included the following five domains (Table 5).
Table 5 Barriers and enablers in TCP implementation identified in interviews using the CFIR framework in West ChinaDomain 1: Characteristics of TCP in PHC sectorsThis domain included 5 constructs: TCP sources, evidence strength & quality of TCP, adaptability of TCP, TB Patient needs & resources, complexity of implement TCP and cost of implement TCP. TCP was developed by the government in China, was evidence-based and cost-effective, significantly promoted TB control, and demonstrated a certain degree of adaptability, which are the key enablers. However, TCP lacked patient-centered delivery approaches and was weak in adaptability to community context, had complexity content and insufficient implementation funding, which were main barriers.
Domain 2: Outer setting for TCP implementation in PHC sectorsTwo constructs mainly including cosmopolitanism of TCP implementation (network between PHC sectors and external organizations outside of the integrated TB control model) and external policy & incentives related to TCP implementation (outside of the integrated TB control model) were taken into the domain of outer setting for TCP implementation in PHC sectors. Interviews revealed that PHC sectors was not well networked with external organizations, such as insufficient support from private clinics or other sectors outside the integrated TB control model and private clinics retaining suspected TB patients without referring to TB-designated hospitals, which were barriers for TCP implementation. It was difficult to implement TCP in PHC sectors without incentive policy or support from education, financial or public security departments.
Domain 3: Inner setting for TCP implementation in PHC sectorsIn this study, inner settings for TCP widely included characteristics of PHC sectors, networks & communication between PHC sectors and CDCs/TB designated hospital, climate of TCP implementation (HCWs’ tension for change related to TCP implementation, compatibility of TB patients, HCWs and related leaders and organizational incentives & rewards for TCP implementation) and readiness for TCP implementation (available resources for TCP implementation and leadership engagement in TCP implementation and access to information and knowledge). Barriers of inner setting for TCP implementation included the lack of sufficient equipment, funding, adequate training programs, adequate communication and cooperation with TB-designated hospitals, qualified TB HCWs, and scientific performance assessment with appropriate incentives. On the other hand, a high demand for high-quality training to strengthen HCWs’ TB care capacity, regular supervision and technological support in PHC sectors from superior healthcare departments were considered as key enablers in this domain.
Domain 4: Characteristics of HCWs involved in TCP implementation in PHC sectorsThis study included HCWs’ knowledge and beliefs about TCP, HCWs’ self-efficacy to TCP implementation, HCWs’ state of change for TCP implementation and HCWs’ identification with PHC sectors as constructs in this domain. HCWs’ values of TCP as an effective program were enablers in this domain. TB patients’ lack of better understanding of TCP, insufficient awareness on TB and health literacy, severe side effects and financial difficulties of TB patients led to their dissatisfaction towards TCP implementation which could also had a negative impact on HCWs’ willingness of TB work, HCWs’ inadequate professional knowledge and skills in TCP implementation, were barriers to TCP implementation.
Domain 5: Processes of TCP implementationPlanning of TCP implementation (the development of TCP implementation strategies in PHC sectors under the guideline of BPHS), engaging stakeholders related to TCP implementation, executing TCP (according to the requirement instructions in the guideline of BPHS) and reflecting & evaluation of TCP implementation were main constructs in this domain. Results disclosed that HCWs’ and TB patients’ none involvement in planning of TCP implementation led to the inadequate understanding of their needs and local contexts, insufficient cooperation within the integrated TB control model, difficulties to implement TCP, and the inappropriate performance assessment were barriers in TCP implementation process. HCWs’ passions of participating in TCP planning were enablers in this domain.
Identified factors of TCP implementation in PHC sectors from mixed-method resultsCombining the results of both questionnaire surveys and in-depth interviews, we identified that 19 CFIR (Fig. 5) constructs on factors of the TCP implementation, covering 5 CFIR domains. Of these constructs, 22 were barriers, 12 were enablers.
Fig. 5
Barriers and enablers identified in TCP implementation using CFIR framework in PHC sectors. CFIR Consolidated Framework for Implementation Research; CDC Centers for Disease Control; TCP Tuberculosis Control Program; PHC Primary healthcare; HCWs Healthcare workers
Barriers existed widely in 5 domains: (1) Characteristics of TCP in PHC sectors: lack of patient-centered implementation strategies, heavy workload on HCWs, complex cross-sectional cooperation on screening and referring, TB patients’ non-adherence to TCP, and insufficient implementation funding; (2) Outer Setting for TCP implementation in PHC sectors: not well networked with other organizations and insufficient support or incentive from relevant departments; (3) Inner setting for TCP implementation in PHC sectors: lack of sufficient implementation equipment, high mobility and shortage of qualified TB HCWs, inadequate communication and cooperation between PHC sectors and TB-designated hospitals, HCWs’ fear of being infected, unreasonable performance review system with insufficient incentives and lack of qualified training program and implementation funding; (4) Characteristics of HCWs involved in TCP implementation in PHC sectors: the need of professional training, HCWs’ inadequate TB care competency, HCWs’ low job satisfaction of and low willingness of TB work; (5) Processes of TCP implementation: none of HCWs or TB patients involved in the development of TCP, inadequate multi-department cooperation, lack of adequate qualified HCWs and unreasonable performance review system.
Enablers arouse from 4 domains including TCP developed based on research evidences and released by national health authorities and departments, improved TB screening, treatment adherence and outcomes, TB screening combined with other BPHS program to improve accessibility and to promote TB health education, e-health approach and increased health funding for TB prevention and control, regular training from CDC or Health Commission, TCP meeting the needs of different patients, HCWs’ aspiration to receive high quality training, supervision and technological support from healthcare authorities, HCWs’ view of TCP as an effective program, and HCWs’ passion towards TCP planning.
留言 (0)