
記住我

Ethical clearance was granted by the Medical Research Coordinating Committee of the National Institute for Medical Research, Tanzania (NIMR/HQ/R.8a/Vol. IX/2890). Meetings with district authorities and village leaders were conducted to obtain permission to conduct research activities in the community. Sensitization meetings were held in each village to explain the objectives and methodology of the study as well as to seek community consent. Questions were asked, and the study team provided explanations during these meetings. Informed consent and/or assent were obtained both orally and in writing from all individual participants and/or parents/guardians in the case of children. Confidentiality was maintained during and after the study.
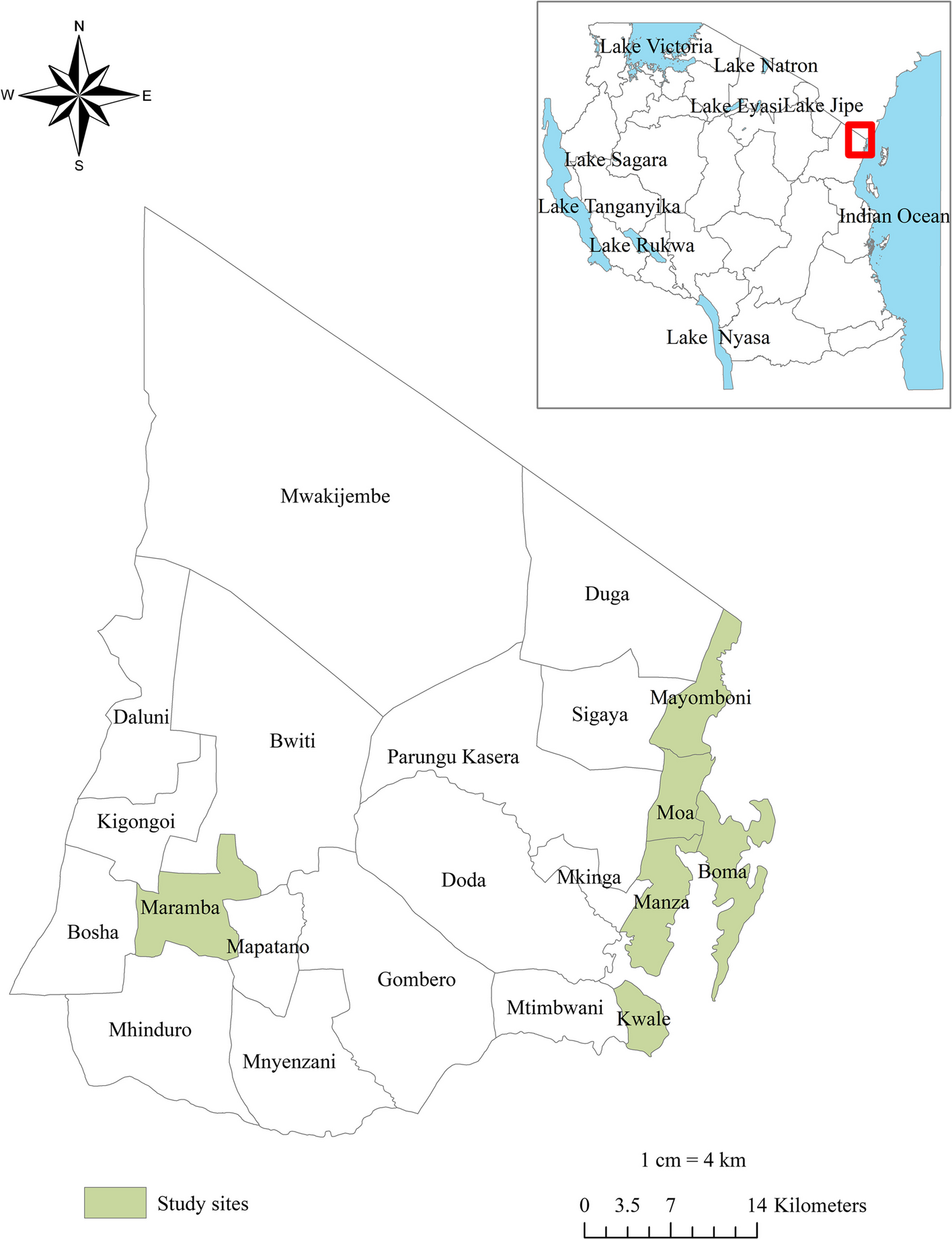
Study areaThe study was conducted in LF endemic communities of the Mkinga district, Tanga region, which is a target area for MDA by the Neglected Tropical Diseases Control Program (NTDCP) in Tanzania. The district is bordered by Muheza district and Tanga city to the South, the Indian Ocean to the East, Korogwe and Lushoto districts to the West and the Kenya border to the North. The district has two main rainy seasons annually (bimodal), the long rains from March to June and the less intensive short rains from November to December. Tanga is a warm and wet climate region with no significant variation of temperature at the coast due to the influence of the Indian Ocean. Humidity is high and often goes up to 100% maximum ranging from 65% to 70% minimum. There are health facilities in most villages in the district, and most of the population has access to a health facility within six kilometers. According to the national census conducted in 2022, the Mkinga district population was 146,802, with 49.8% (73,048) being males (14). The altitude ranges from 0 to 1506 m above sea level measured from the Nilo peak (15). The main economic activities in this district include fishing, subsistence farming, low-scale livestock keeping, and petty trading for the rest. Figure 1 depicts the location of the study sites.
Fig. 1
Map of the study site. In the top left corner, there is a map of Tanzania, situated in the eastern part of Africa. The red square highlights the Tanga region, where Mkinga district is located. The bottom left section displays a detailed map of the wards within the Mkinga district, indicating the villages that participated in this study. This study site map was created using ArcGIS software version 10.7.1 (Esri, California, USA)
Study design and populationThis prospective longitudinal efficacy study was nested in a larger community-based cross-sectional study conducted between November 2018 and January 2019 [16]. In brief, two weeks prior to MDA, a total of 4115 MDA-eligible individuals (49.7% males, 35.2% children) were screened for CFA across 15 villages. Those testing positive for CFA were further screened for microfilaremia. All eligible residents, regardless of their CFA or microfilariae status, received MDA following the WHO guidelines [2, 24]. All individuals who tested positive for CFA, including those who also tested positive for microfilariae before MDA, were enrolled and monitored for clearance of CFA and microfilariae following MDA. Pregnant women and children under five years old were excluded from the study due to contraindications for the medications used.
Treatment and follow-upIn Tanzania, residents in LF- endemic districts are eligible to receive annual MDA comprising IA combinations as preventive chemotherapy, without prior diagnosis following the WHO and national MDA program guidelines [2, 24]. Accordingly, all residents in our study area, including those who tested positive for CFA and microfilariae in our study, received single dose IA combinations as preventive chemotherapy through MDA campaign. The MDA was implemented by the National NTD control program through house-to-house visits, and the study team had no role in the planning or administration of the drugs. During the MDA campaign, residents were advised to take the medicine after food intake. Food intake was not considered in the study as it was observational and followed routine protocols established by the national MDA program.
After recording baseline sociodemographic, clinical, and medical history, including any comorbidities and concomitant medications, participants received a standard dose of ivermectin based on height (corresponding to 150–200 μg/kg) and albendazole 400 mg as recommended by the WHO [2, 24]. Ivermectin tablets were donated by Merck Sharpe and Dohme (MSD), Haarlem, The Netherlands. Albendazole was donated from GlaxoSmithKline (GSK), Brentford, UK.
On MDA Day, all MDA-eligible residents of the community, including those who were screened the diseases and those tested positive for CFA and microfilariae received a standard dose of IA as preventive chemotherapy under direct observed therapy. A longitudinal follow-up was conducted on a cohort of enrolled individuals who initially tested positive for CFA and microfilariae prior to MDA to monitor the changes in microfilariae and CFA positivity status after MDA. The clearance of microfilariae was assessed at both seven days and six months post-MDA, while the clearance of CFA was specifically evaluated at the six-month mark following MDA.
Assessment of circulating filarial antigenemiaAll individuals who tested positive for CFA before MDA underwent re-examination six months after receiving MDA to assess the efficacy of IA in clearing antigenemia. In brief, CFA detection test was performed on finger prick blood samples collected from study individuals using the rapid test for circulating filarial antigenemia (Filariasis Test Strip or FTS; Alere, Inc) as described previously [16]. Briefly, approximately 75 µl of blood was applied on Alere™ FTS (Alere©, Waltham, United States) using a special pipette with a 75 µl mark, and results were read at 10 min and recorded as CFA positive and negative. This test was done before MDA and was repeated at six months following MDA. FTS-positive tests were read by two independent study team members, and positives were retested.
Assessment of microfilaraemiaAll CFA-positive individuals were subsequently re-examined for microfilaraemia before and after receiving MDA using night blood smear microscopy. In brief, night blood sample collection from CFA-positive individuals was conducted between 21:00 and 1:00 to maximize the detection of microfilariae in the blood [25]. Finger prick blood samples were collected into 75 μl capillary tubes and transferred into a 1.8 ml cryotube containing 900 µl of 3% acetic acid, mixed thoroughly and transferred into Sedgwick-Rafter counting chamber. LF parasitemia was estimated by counting the number of microfilariae in the chamber using a compound light microscope set at 4 × magnification located at the National Institute for Medical Research (NIMR) laboratory in Tanga. Results were reported as number of microfilariae per 75 µl of blood. To ensure quality control, the readings for microfilariae for each night blood sample were done by two well-trained and experienced laboratory technicians, who discussed and agreed on the results. All positive tests were also reviewed by the study leader or designated scientist. Blood sampling was done at a village meeting point (health facility or village office building) in most cases. The door-to-door approach was also used under special circumstances, especially when individuals did not show up for blood sampling.
Determination of ivermectin plasma concentrationsTwo milliliters of venous blood were drawn at 0, 2, 4, and 6 h post-drug administration from the antecubital arm vein. The plasma levels of ivermectin were quantified using liquid-chromatography tandem mass spectrometry [26]. Population pharmacokinetic (PopPK) modeling of data was done using NONlinear Mixed Effects Modeling (NONMEM) as described previously [27]. Non-compartmental analysis (NCA) with linear trapezoidal rule was used to calculate maximum drug concentration (Cmax) in ng/ml and area under the curve (AUC0–6 h), in ng·h·ml−1. The Cmax and AUC were assessed for between-subject variability (coefficient of variation—CV%). Association of variability in ivermectin pharmacokinetic parameters with clearance of microfilariae and CFA after MDA was analyzed.
Data management and statistical analysisData was collected electronically using tablets and submitted to the central server daily at the National Institute for Medical Research, Tanga Medical Research Centre laboratory. The Open-source data kit (ODK, https://opendatakit.org/) software was used to create the database and data collection applications. The data manager ensured daily precision and consistency checks, resolving queries promptly. Continuous data cleaning and validation were conducted, with periodic reports generated. Descriptive statistics summarized sociodemographic and clinical characteristics. To assess the impact of MDA, the McNemar test was employed to compare the proportions of microfilarial positives before and after the intervention. Factors associated with CFA status at six months were analyzed using either the Chi-square or Fisher’s exact tests. Univariable and multivariable logistic regression analyses were conducted to control for potential confounders. Factors with a P-value of < 0.2 in the univariable analysis or with clinical relevance and previously reported associations were included in the multivariable model. All P-values in statistical tests were two-sided, with a significance level set at < 0.05. Data visualization and analysis were performed using GraphPad Prism version 10 (GraphPad Software, San Diego, California, USA).
留言 (0)