Study design
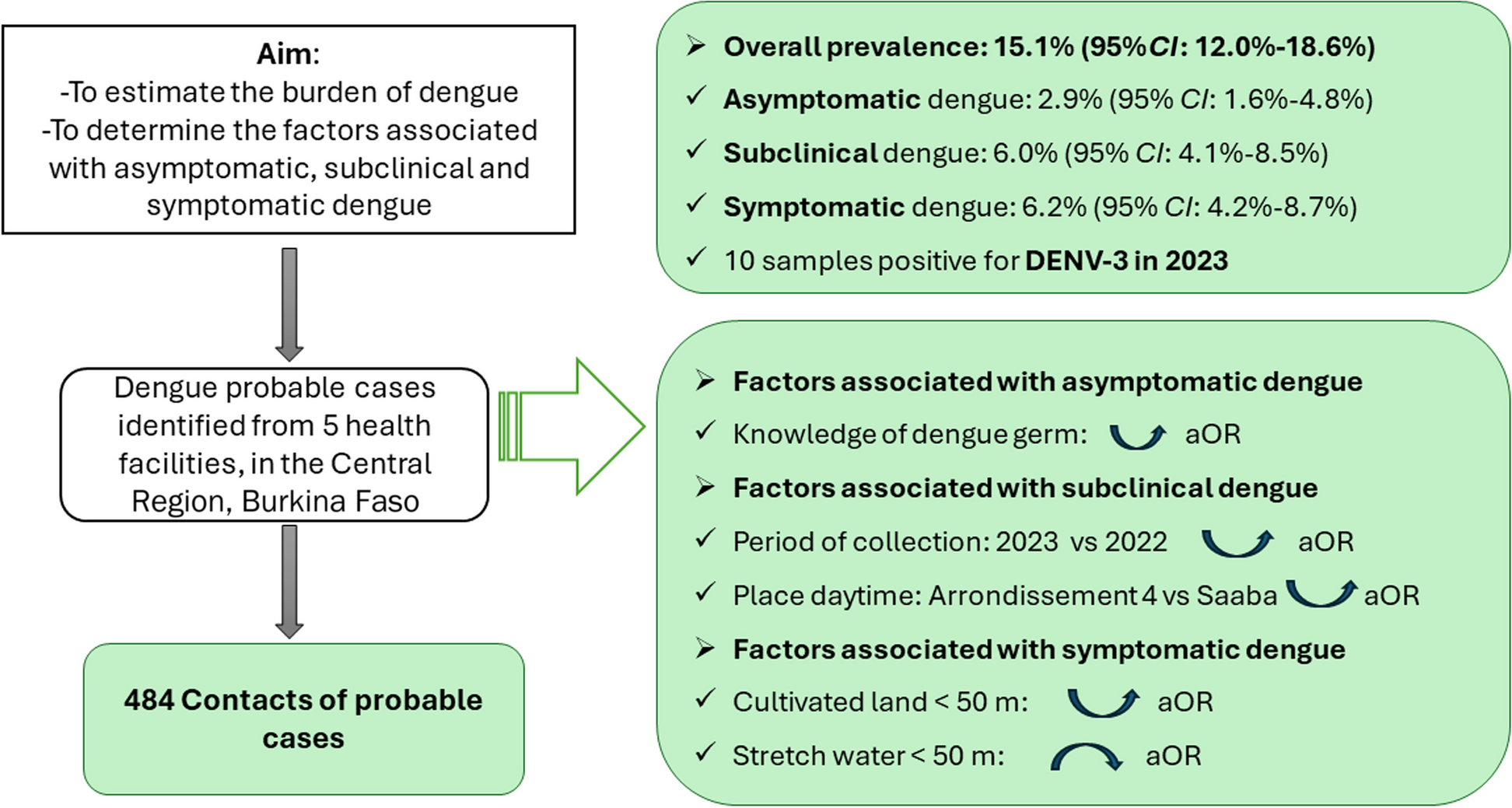
This study is part of an overall research aiming to estimate the prevalence of symptomatic and asymptomatic dengue among adults in Burkina Faso in 2022 and 2023 [22]. The overall study included two populations, dengue suspected cases from selected health facilities and the contacts of those turning probable cases. Within this research, we conducted cluster sampling through household-based data collection, systematically targeting contacts of dengue probable index cases. Data were collected from September to November 2022 and September to November 2023, at the end of the rainy season when malaria and dengue cases peak.
Study setting
This study was conducted in Burkina Faso. It targeted the Central Region with the Capitale City of Ouagadougou surrounded by the six rural municipalities of Koubri, Saaba, Pabré, Komsilga, Komki-Ipala, and Tanghin-Dassouri [23]. Ouagadougou is structured into 12 arrondissements and 55 sectors, with 2,415,266 inhabitants in 2019 [24]. According to the same population and housing census, the Central Region had a population of 3,032,668 inhabitants, with 62.4% of adults [25].
The regional health system includes 5 health districts, which are Bogodogo, Baskuy, Boulmiougou, Sig-Nonghin and Nongr Massom health districts.
Sample size estimation
We determined the minimum sample size using the formula for estimating a single proportion [26]:
$$\text\ge \frac_^ X p(1-p)}^}$$
-p: anticipated prevalence of asymptomatic dengue fever;
-Z1-α/2: percentage standard deviation corresponding to the two-sided significance level. For α = 5%, Z1-α/2 = 1.96.
-e: precision of 1.75% (half of 3.5%, the prevalence of immunoglobulin M in Africa).
We assumed that the contacts would be surveyed late, so the prevalence of immunoglobulin M was used to calculate the sample size. It was pooled at 3.5% (95% CI: 0.8–7.8%) among apparently healthy people in Africa [18]. The required sample size was estimated at 424, then adjusted to 472, considering an adjustment of 10% non-response rate with the formula (n = \(\frac_}_}\)).
Participants characteristics
The study considered individuals aged 16 years and older, family contacts of dengue probable cases, regardless of the presence of fever or other symptoms. Mentally debilitated individuals were excluded from the study. Participants were further classified as follows based on clinical and serological characteristics:
Dengue fever suspected case: fever (≥ 38.5 °C) in the last five days with at least 2 of the following symptoms (headache, retro-orbital pain, myalgias, arthralgias, skin rash, bleeding manifestations, or shock syndrome) [27].
Probable dengue fever: a suspected case with a positive rapid diagnostic test (RDT) for dengue non-structural 1 protein antigen (AgNS1) and/or immunoglobulins (Ig)M and/or IgG. Probable cases identified from the health facilities were the index cases. Probable cases identified among the contacts of index cases were referred to as symptomatic cases. These symptomatic cases are undiagnosed infection [17] that did not seek care for the ongoing episode in a health facility. Without antibody titers, we did not consider distinguishing primary and secondary infections.
Subclinical dengue case: presenting a fever and/or other symptoms but not fitting the definition of a suspected case. It is sometimes referred to as mild infection, as considered in some studies.
Asymptomatic dengue case: participants turning positive for dengue RDTs with positive AgNS1 and/or IgM markers without any fever or symptom, fitting clinically undetectable infections [17].
Dengue contacts of an index case: participant sharing the same household, house, or compound (Celibateriums in French) with an index case.
Data collection
We conducted face-to-face interviews with a structured questionnaire and RDTs, using the Kobo Toolbox. The questionnaire included participants-level factors (sociodemographic characteristics and knowledge of dengue) and household-level factors (environmental characteristics).
Index cases were identified through a three-stage sampling [22]. These symptomatic participants who were at least positive for AgNS1 and/or IgM were followed home. Then, all people residing in the same household or compound as the dengue probable case were asked to participate in the study. Participants were tested for malaria and dengue using RDTs. The SD Bioline Malaria Ag P.f kit (SD Standard Diagnostics, INC., Republic of Korea) and the Standards Q Malaria P.f Ag kit (SD Biosensor, Inc., Republic of Korea) were used to test for malaria by Plasmodium falciparum. The WONDFO Dengue NS1/IgG/IgM kit (Guangzhou Wondfo Biotech Co., Ltd, China) was used to test for the infection with the dengue virus. The tests followed the manufacturers procedures. Participants at least positive for AgNS1 and/or IgM were sampled for serotyping.
Participants positive for dengue RDT without presenting any symptom or sign were contacted up to the following 10 days to confirm they were not presymptomatic.
Characterization of dengue viruses serotypesExtraction of dengue viral RNA
Dengue virus RNA extraction was performed using the QIAamp Viral RNA Mini Kit (Qiagen, Germany), according to the manufacturer protocol. The extract was stored at -80 °C for molecular testing.
Serotyping of dengue viruses
Identification of the dengue virus genotypes was performed using Sacace PCR kit for detection (Sacace Biotechnologies, Italy). Differentiation of Dengue virus genotypes 1, 2, 3 and 4 in clinical material Dengue Real-™ Genotype (Sacace, Como, Italy) and the PCR steps followed the manufacturer instructions. This resulted in a total reaction volume of 25 µl for each PCR. To guarantee the quality of the results, three controls, which are negative control of extraction (NCE), positive control of amplification (C +) and negative control of amplification (NCA) were used.
The PCR reaction mixtures contained in sterile 0.2 ml microtubes were introduced onto the SaCycler-96 Real-Time PCR v.7.3 plate (Sacace Biotechnology, Italy) for amplification. The amplification program consisted of one cycle of 50 °C for 30 min, 95 ˚C for 15 min, followed by five cycles of 95 ˚C for 10 s, 56 ˚C for 40 s, and 72 ˚C for 20 s, and finally 40 cycles of 95 ˚C for 10 s, 54 ˚C for 40 s, and 72 ˚C for 20 s.
The results were interpreted using the RealTime_PCR software v7.9 (Dna -Technology LLC, Moscow, Russia) by the crossing or not crossing of the threshold line by the fluorescence curve. The genotypes were then identified following the manufacturer’s protocol.
Statistical analyses
The software STATA/IC 16.1 (StataCorp LLC, College Station, Texas 77,845 USA) was used for analyses.
The prevalence of asymptomatic, subclinical, and symptomatic dengue fever was estimated with 95% confidence intervals. They were presented for the overall sample, symptomatic cases, subclinical cases, and asymptomatic cases. Independent variables were presented with mean ± standard deviation (SD) or median [interquartile range (IQR)] for the quantitative variables. Qualitative variables were presented with frequency and percentage.
Further, a binary logistic regression was done to identify the determinants of asymptomatic, subclinical, and symptomatic dengue among contacts of probable dengue cases. A univariate binary logistic regression was first done to identify the sociodemographic and environmental factors associated with asymptomatic, subclinical, and symptomatic dengue. Then, factors significant at 20% and those pertinent (like age and sex) even not significant in the univariate logistic regression were included in the multivariable analysis. The model with the lowest Akaike Information Criteria (AIC) and the narrowest intervals was retained for each dengue type.


留言 (0)