
記住我
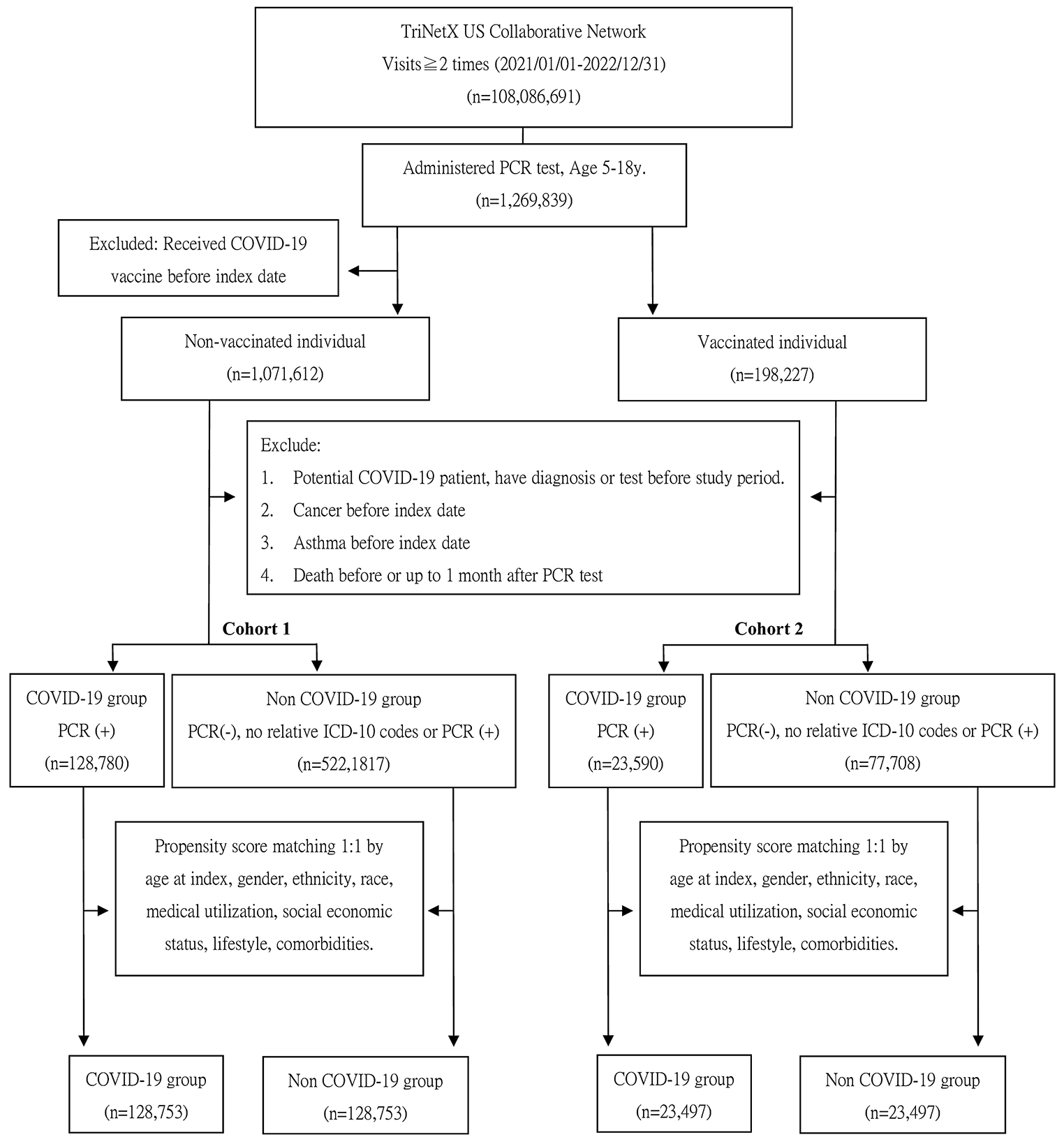

Of the 333 ICUs from 52 countries comprising the EUROBACT-2 cohort, 219 ICUs from 43 countries reported on at least one older adult (≥ 75 years old). Accordingly, a total of 2111 individuals hospitalized in ICU and diagnosed with HA-BSI were included in the current study (Fig. 1). Of these, 1577 (75%) were from 142 (65%) ICUs in countries located within the WHO European Region. The median HDI of participating countries was 0.85 (IQR 0.76, 0.93), and a total of 1183 (56%) individuals were reported from ICUs in countries with an HDI of the higher median (Supplementary Table S1).
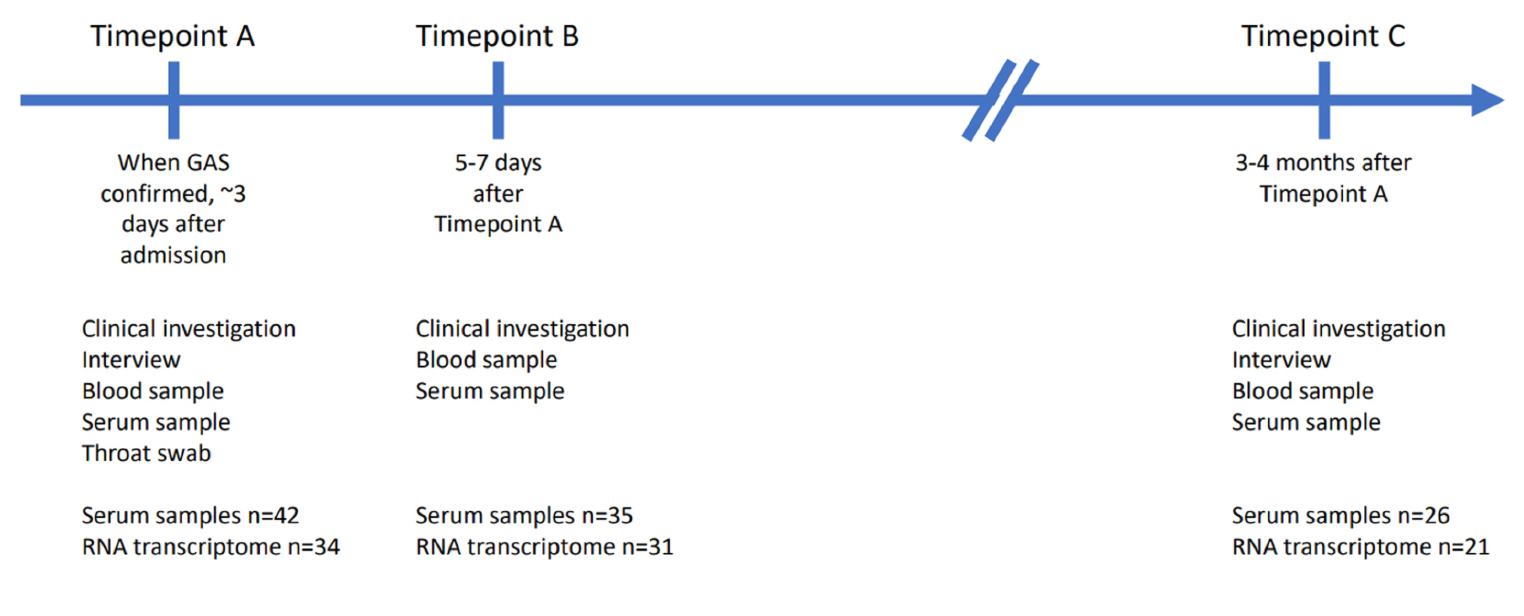
Fig. 1
Study flow diagram. DNR do not resuscitate, ICUs intensive care units, y/o years old
Of the total cohort, 563 (27%) were older adults (≥ 75 years old).
Comorbidities and functional statusOlder adults had higher Charlson comorbidity index (median 2 [IQR 1.4] vs 1 [IQR 0.4], p < 0.001) and generally more comorbidities, however non-elderly individuals had higher proportions of severe liver disease (4% vs 1%, p = 0.003), hematological malignancy (7% vs 4%, p = 0.020), and transplant recipients (4% vs 0.2%, p = 0.002). Older adults exhibited higher proportions of baseline functional limitation, and only 28% of whom were completely independent compared to 45% of the non-elderly individuals (p < 0.001). Younger individuals had slightly higher average BMI (median 26.2 [IQR 23.5, 30.2] vs 26.2 [23.5, 29.7], mean 27.5 [SD 7.4] vs 26.7 [5.4], p = 0.015).
Altogether, 278 (13%) of the cohort were admitted due to COVID-19, with similar proportions between both age groups (13% vs 14%, p = 0.319). (Table 1).
Table 1 Characteristics of 2111 individuals diagnosed with HA-BSI, according to age category, adjusted for centerPatient characteristics at bloodstream infection diagnosisThe source of HA-BSI slightly differed between the sub-populations (p = 0.021). Older adults had lower proportions of catheter-related BSI (22% vs 28%, p = 0.005). Additionally, older adults tended to have higher proportions of respiratory (28% vs 25%, p = 0.180) or urinary (9% vs 7%, p = 0.082) source, and primary bacteremia (20% vs 17%, p = 0.099). Younger individuals tended to have higher proportions of intra-abdominal source (16% vs 14%, p = 0.314). Older adults had lower maximal heart rate (median 110 [IQR 94, 126] vs 113 [97, 130] beats per minute, p = 0.019), minimal mean arterial pressure (median 65 [IQR 56, 74] vs 66 [58, 75] mmHg, p = 0.012) and maximal body temperature (median 37.6 [IQR 36.9, 38.4] vs 38.1 [37.2, 38.8] °C, p < 0.001), though SOFA scores, blood parameters and ventilatory requirement were non-significantly different. However, a higher proportion of older adults were presented with non-sedative coma (17% vs 14%, p = 0.038).
The causative pathogens and resistance patterns were similar between the two sub-populations (Table 1).
Management of bloodstream infectionImaging was performed similarly for both groups, except for MRI that was performed less frequently among older adults (1.6% vs 3.2%, p = 0.049). The latter were also less likely to receive adequate antibiotic treatment within 24 h, although this finding did not reach statistical significance (49% vs 53%, p = 0.051).
Among older patients, source control was less often indicated (44% vs 53%, p < 0.001), and, when attempted, was less frequently effective (77% vs 83%, p = 0.017). Additionally, Extracorporeal membrane oxygenation (ECMO) was also significantly less used among older adults (0.2% vs 1.9%, p = 0.020) (Table 2).
Table 2 Management of HA-BSI among 2111 individuals, according to age category, adjustments for centerOutcomesOlder adults had higher all-cause mortality at 28-days (50% vs 34% among non-elderly individuals, respectively, p < 0.001), and lower discharge rate at 28-days (12% vs 20%, p < 0.001). Following exclusion of those whose death was preceded by a decision to avoid life-sustaining treatment (77 (27%) older adults and 142 (27%) younger patients who died by day 28), all-cause mortality remained significantly higher among older adults (42% vs 27%, p < 0.001).
Sensitivity analysesFollowing the exclusion of 278 (13.2%) of the cohort who were admitted due to COVID-19, differences in BMI, diabetes mellitus and presentation with non-sedative coma became insignificant. Older adults appeared to have higher proportions of peptic ulcer disease (6% vs 3%, p = 0.019) and respiratory source for BSI (29% vs 23%, p = 0.014) (Supplementary Table S1).
While response to therapy at 7 days remained slightly better among younger individuals, the all-cause mortality rate at 7 days did not differ between the groups. Yet, age group-related differences in the all-cause mortality rates at 28 days remained unchanged (Supplementary Table S2).
A total of 1183/2111 (56%) patients in 142 (65%) ICUs were from countries with an HDI greater than the median of the cohort. By restricting the analysis to include only these individuals, age group-related disparities in a few baseline characteristics were identified. Moreover, this analysis revealed that among older adults hospitalized in the ICU with BSI, the proportion of admissions due to COVID-19 was lower (7% vs 12%, p = 0.025). They also had higher proportion of urinary source for their BSI (10% vs 6%, p = 0.028) (Supplementary Table S4). Nonetheless, all-cause mortality at 28 days and source control rates remained unchanged. Yet, all-cause mortality rates at 7 days and discharge rates at 28 days become statistically insignificant. However, as seen in the entire cohort, among older adults, source control less often indicated (49% vs 56%, p = 0.023) and, when attempted, was less frequently effective (78% vs 86%, p = 0.038) (Supplementary Table S5).
Analysis according to baseline physical status (any functional limitation vs none), regardless of age, revealed that individuals with functional limitation were more likely to undergo CT scan (43% vs 37%, p = 0.003). Moreover, among individuals with any limitation, source control was less often indicated (48% vs 54%, p = 0.011), pursued (92% vs 95%, p = 0.011) or successfully accomplished (79% vs 85%, p = 0.013). Individuals with physical limitation were more likely to receive corticosteroid therapy (28% vs 21%, p = 0.001) and renal replacement therapy (21% vs 16%, p = 0.006) for sepsis and were less likely to undergo ECMO (1% vs 3%, p = 0.002). Among older adults, no differences in management were observed between independent individuals and those with functional limitation, except for a higher proportion of corticosteroid therapy among non-independent patients (27% vs 18%, p = 0.021) (Supplementary Table S6).
留言 (0)