Participants
The study was performed in 1050 children participating in the Primary Oral Insulin Trial (POInT). POInT investigates whether daily intake of oral insulin reduces the incidence of islet autoimmunity and/or type 1 diabetes in children with an increased risk of type 1 diabetes [15]. Children were eligible if they had an increased risk for developing islet autoimmunity of > 10% by the age of 6.0 years, defined by a genetic risk score [16] (Supplementary Table S1). Enrollment commenced in February 2018 and ended in March 2021. Children were enrolled at the age of 4.0–7.0 months, and followed at 2, 4, and 8 months after study enrollment, at 1.5 years of age, and then every 6 months. Daily treatment with oral insulin or placebo continued until age 3 years. The study was conducted in seven clinical research centers including three in Germany (Dresden, Hanover, and Munich), one in Sweden (Malmö), one in Poland (Warsaw), one in Belgium (Leuven), and one in the UK (Oxford). Adverse events were recorded at each clinical study visit until 6 months after end of treatment. For the current analysis, reported infections until 02/28/2023 were included. A detailed description of the study protocol has been published previously [15].
Assessment of exposure to infections
At each scheduled clinic visit, adverse events were collected by study personnel and recorded in the clinical trial database. For each event, illness description, date of onset and end date was recorded. Adverse events were categorized using the Medical Dictionary for Regulatory Activities (MedDRA). Classification of infections was performed as previously described [17] (Supplementary Table S2). In brief, the first infection episode category was created from MedDRA Lowest Level Terms (LLT) as respiratory infection. If terms belonging to this category were reported within one week, they were regarded as one respiratory infection episode. Gastrointestinal symptoms are considered to occur frequently in young children with a respiratory infection and therefore gastrointestinal symptoms co-occurring with respiratory infections were considered as part of the respiratory infection episode. The second infection episode category was created from MedDRA LLT as gastrointestinal infections. If terms belonging to this category were reported within the same week, they were regarded as one gastrointestinal infection episode. The third category was defined as “other types of infections”, and the fourth category was unknown febrile episodes. Each LLT within this category is treated as a distinct infection episode. The date of all episodes was the date of the first LLT. A separate category was given to infections associated with Coxsackie virus (Supplementary Table S2). In the present study, follow-up data up to 40 months of age were evaluated.
Islet autoimmunity outcome
Islet autoantibodies were measured centrally at two independent GPPAD Core laboratories, located at the Institute of Diabetes Research, Helmholtz Munich, Germany, and at the University of Bristol Medical School, Diabetes and Metabolism, Learning and Research, Southmead Hospital, Bristol, United Kingdom (for confirmation of results). Serum samples from each visit were analyzed for autoantibodies to insulin, GAD65, IA-2 and ZnT8 (ZnT8RA and ZnT8WA) as previously described [18]. A child was classified as islet autoantibody positive if 2 consecutive samples tested positive at both laboratories. A child was classified as multiple islet autoantibody positive if tested positive for 2 or more autoantibodies in both laboratories. The islet autoimmunity outcome was defined as either development of multiple islet autoantibodies or the development of one or more islet autoantibodies followed by type 1 diabetes. Maternally transferred islet autoantibodies were excluded and identified if the child was positive at the first sample, had declining antibody titers on follow-up, and subsequently became islet autoantibody-negative. For children classified as islet autoantibody-positive, the first positive sample was taken as the age at seroconversion.
Study approval
Ethical approval for the POInT study was obtained from local ethical committees and regulatory authorities of the Technische Universität München, Medical Faculty (326/17 Af), the Medical University of Warsaw (Institute of Mother and Child) (199/2017), the UK Health Research Authority (18/SC/0019), Onderzoek UZ/KU Leuven (S60711) and the Regionala etikprövningsnämnden i Lund (2017/918). The parents or legal representatives of each participant provided written informed consent, and further agreed to biobank storage of material that was used in this study.
Statistical analysis
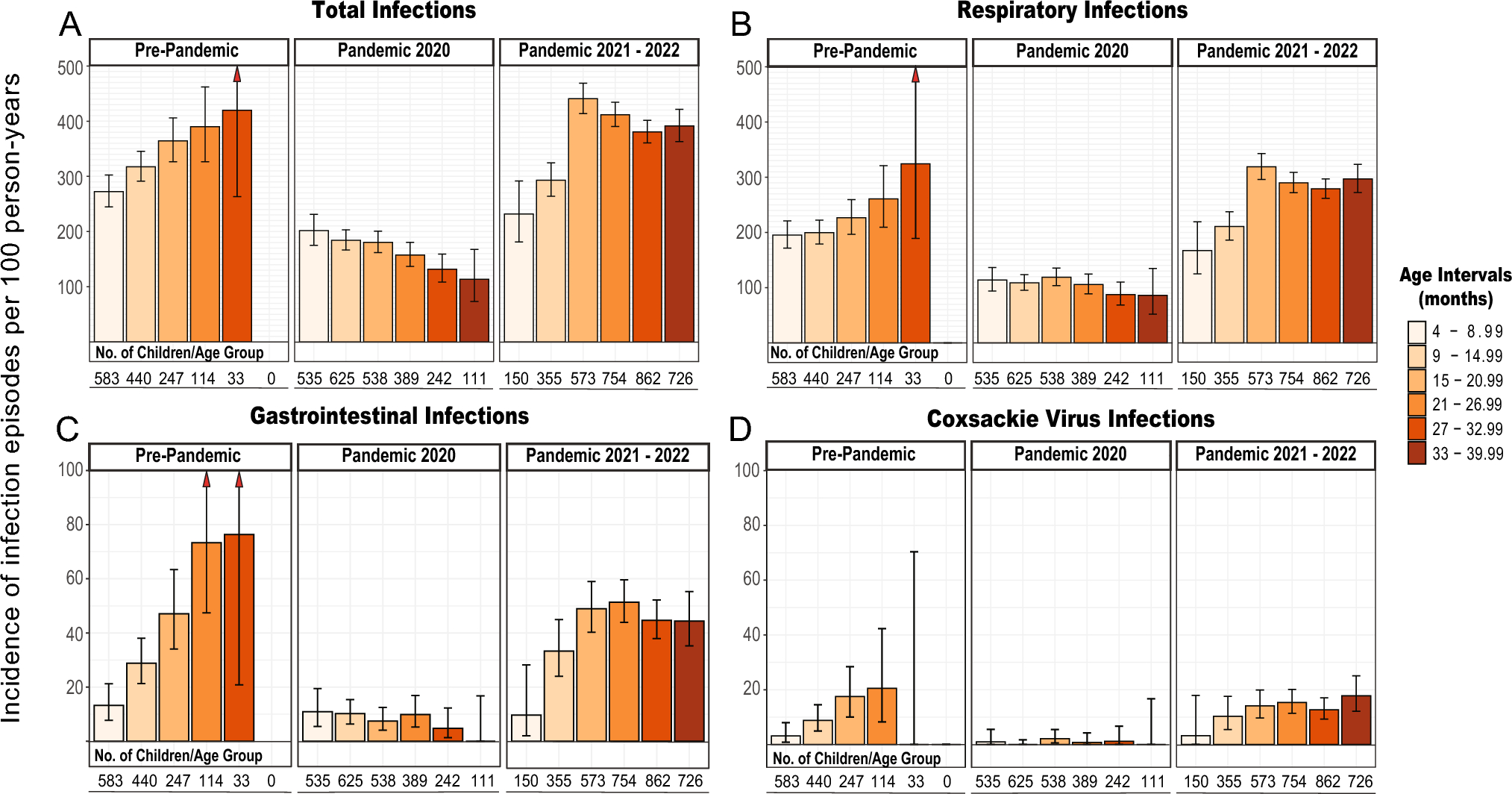
Age- and stage-specific counts of infection episodes were calculated across distinct age intervals: 4–8.99 months, 9–14.99 months, 15–20.99 months, 21–26.99 months, 27–32.99 months, and 33–39.99 months. Infection episode counts were also segmented into pre-pandemic (2018–02-07 to 2020–02-29), pandemic 2020 (2020–03-01 to 2021–02-28), and pandemic 2021–2022 (2021–03-01 to 2023–02-28) periods. Infection episodes for each group combination were expressed as infection rates per 100 person-years.
Multivariable Poisson regressions incorporating sex, HLA risk group, GP/FDR status, country, age group and pandemic stage as covariates were applied to model the various infection rates over a maximum 36-month period. The significance of each categorical variable was assessed using Wald tests, comparing each category against its respective reference. Results were expressed as rate ratios (with 95% confidence intervals) or as a percentage change in the rate.
To facilitate specific pairwise comparisons among age groups and stages of the pandemic, contrast matrices were developed and employed. Given that these pairwise comparisons entailed conducting multiple tests, the Bonferroni adjustment was applied to account for this multiplicity.
In the study of islet autoantibody incidence, rate ratios were calculated as the ratio derived from the calculated incidences across different groups. To assess the statistical significance of differences between these rate ratios a proportion test was performed based on the chi-squared statistic.
Throughout the study, statistical significance was determined based on p-values being less than 0.05. Graphs were generated using the ggplot2 package (version 3.4.4), and all statistical analyses were conducted using R software (version 4.3.2, https://www.R-project.org/).


留言 (0)