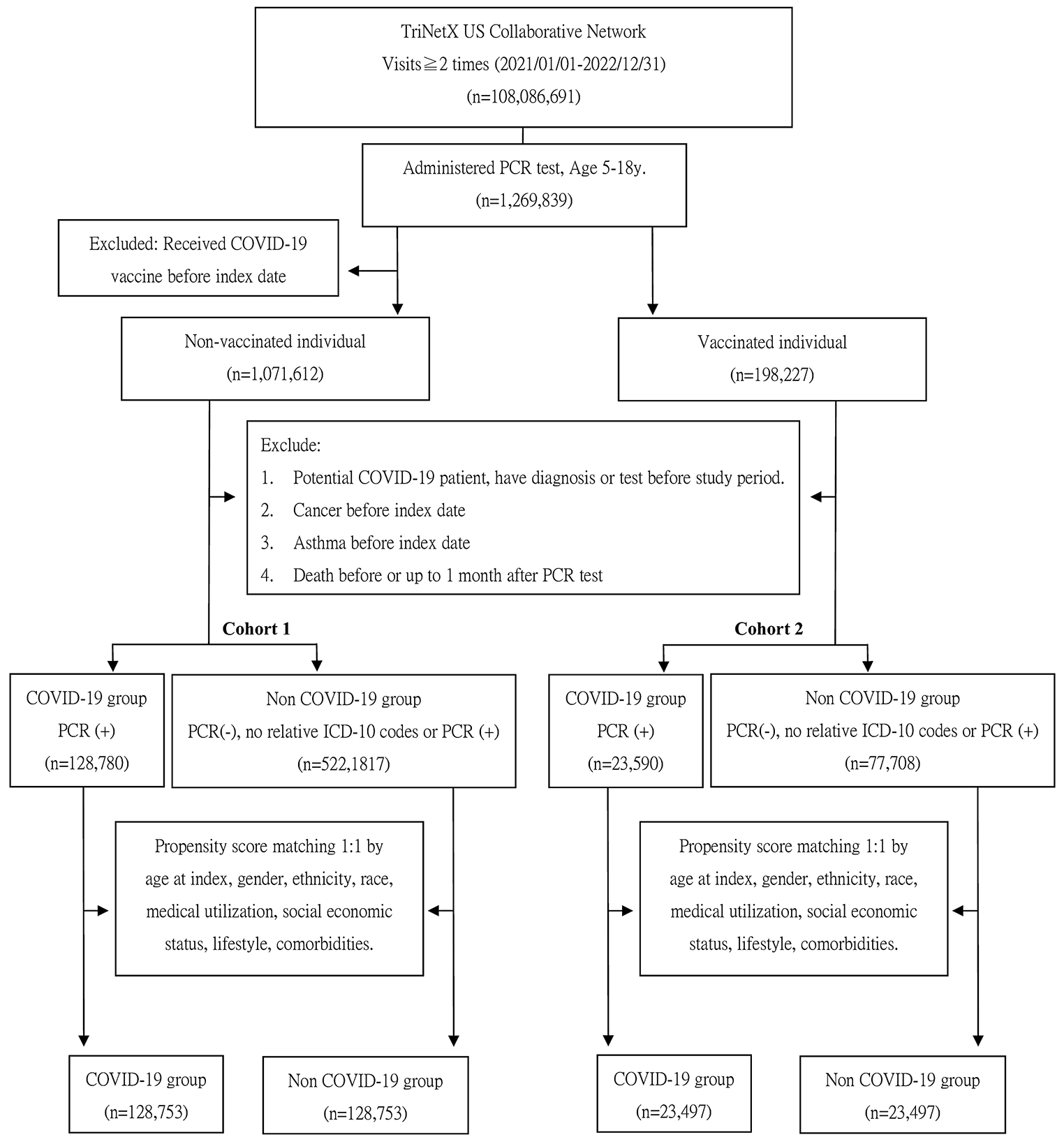
This large retrospective cohort study utilized TriNetX, a real-world database, to evaluate the impact of COVID-19 infection and vaccination on the incidence of new-onset asthma in children. Regardless of vaccination status, groups infected with COVID-19 exhibited a significantly increased incidence of new-onset asthma, anti-asthmatic drug use and composite outcomes compared to those not infected, from the 30th to the 365th day following the index date, over a period of 11 months. The subgroup analysis was consistent across gender, age, and racial groups.
The link between viral infections and asthma exacerbation is well-established, but the association with new-onset asthma, particularly in the context of COVID-19, is a relatively novel area of research. Our findings support the increasing evidence that COVID-19 may trigger asthma development. This corresponds to findings from research on other respiratory viruses, such as rhinovirus (RV) and respiratory syncytial virus (RSV), which are recognized for triggering asthma in individuals with a genetic predisposition. In a Finnish study, rhinoviruses were also identified as significant inducers of wheezing [15]. A systematic review of 28 articles revealed an increased risk of asthma following hospitalization for RSV in infancy and childhood [16]. Also, the findings of a meta-analysis suggested that experiencing wheezing illness caused by RV during the first 3 years of life was linked to the later development of wheezing or asthma [17]. Rhinoviruses infection promotes the secretion of cytokines from epithelial cells, such as IL-6, IL-8, IL-11, and GM-CSF, which may trigger the onset of asthma [18,19,20,21]. In a large, population-based, birth cohort study (INSPIRE), not being infected with RSV in the first year of life was associated with a 26% lower risk of asthma at age 5 compared to those who were infected with RSV (adjusted RR = 0.74, 95% CI = 0.58–0.94, p = 0.014).22 Furthermore, RSV infection in infants has been shown to affect T-cell memory responses and airway epithelium development [23]. The interaction of viral virulence factors, individual genetic susceptibilities, and environmental factors—such as exposure to the airway microbiome—plays a significant role in the aggravation of wheezing illnesses and the increased risk of asthma development [24, 25].
Some literature has indicated the impact of COVID-19 on individuals with asthma following infection. The interaction of the virus with the ACE2 receptor, which is variably expressed in asthma patients, may influence the severity of COVID-19 and could potentially exacerbate asthma symptoms [26]. One study highlighted the importance of host factors in both asthma and COVID-19, discovering shared genetic and molecular pathways in the two conditions through the analysis of bronchoalveolar lavage fluid, suggests that COVID-19 may contribute to the exacerbation or onset of asthma in affected patients [27].
To date, there are few studies that explore the issue of new-onset asthma caused by COVID-19 infection. A nationwide, population-based cohort study emphasized that adults who were infected with COVID-19 had a higher incidence of new-onset asthma compared to those uninfected [5]. This suggests a potential risk factor for developing asthma following COVID-19 infection. However, earlier research has been limited by smaller sample sizes and relatively brief observation periods.
A review article found that many viruses, particularly single-stranded RNA viruses, can cause asthma [28]. SARS-CoV, also a single-stranded RNA virus, may have similar effects or mechanism. Research shows that certain viruses can cause epithelial cells to produce pro-Th2 cytokines such as IL-25 and IL-33, activating ILC2s, DCs, and Th2 cells, thereby promoting allergic inflammation [29, 30]. It has been reported that serum IL-33 levels are elevated in COVID-19 patients. This cytokine increases neutrophil activity via the IL-33/ST2 pathway and inhibits IFN-I secretion by pDCs. Additionally, IL-33 disrupts the Th17/Treg balance in the lungs, leading to cytokine storms and immune damage. IL-33 also causes hyperactivation of ILC2s, differentiation of M2 macrophages, and secretion of TGF-β and IL-13 [31]. Common coronavirus infections in children trigger host responses similar to those induced by other viruses, such as increased expression of IL6 and ACE2 [32]. COVID-19 infection can also trigger an imbalanced immune response, characterized by a cytokine storm and overproduction of pro-inflammatory cytokines [33,34,35]. Additionally, the infection may impair mucociliary clearance, a vital respiratory defense, leading to mucus and pathogen accumulation in the airways [33]. In COVID-19 patients, there’s a marked increase in IL-4 expression and a rise in M2 macrophages, suggesting a significant Th2 immune response and anti-inflammatory activity that potentially leads to airway remodeling [36]. Unlike the limited Th1/Th17 response, the strong Th2 response in SARS-CoV-2 induced lung injury suggests a mechanism that favors airway remodeling [36].
In the United States, the Pfizer-BioNTech COVID-19 vaccine was authorized for those 16 and older on December 11, 2020, and approved by the FDA on August 23, 2021. Its use expanded to 12–15 year-olds on May 10, 2021, and to children 5–11 on October 29, 2021. By July 6, 2022, CDC data showed 37% of 5–11 year-olds and 70% of 12–17 year-olds had received at least one vaccine dose. Two case reports have indicated that the SARS-CoV-2 vaccine could potentially exacerbate asthma, suggesting that repeated vaccinations might be a risk factor for severe asthma flare-ups. This association is thought to involve inflammatory and immunological responses [37, 38].
To date, there have been several cohort studies that have linked COVID-19 infection in both adults and children. Kim utilized the Korean National Health Insurance claim-based database to design three cohorts for adults and found that 1.6% of the COVID-19 group and 0.7% of the non-infected group developed asthma during the 6-month observation period. The COVID-19 cohort faced a higher risk of new-onset asthma (aHR 2.14; 95% CI 1.88–2.45) than matched controls, aligning with our findings. Kim noted that vaccinated infected individuals had a lower asthma risk compared to their unvaccinated counterparts (aHR 0.82; 95% CI 0.76–0.89). However, vaccination did not reduce asthma risk in those uninfected by COVID-19 (aHR 0.95; 95% CI 0.87–1.04) [6]. A study with cohorts from South Korea, Japan, and the UK shows a significant rise in allergic diseases like asthma and allergic rhinitis after COVID-19, persisting over six months and worsening with disease severity. Vaccination with at least two COVID-19 doses provided protection [7]. As for children, there is limited and inconclusive literature on the risk of asthma following COVID-19 infection in children. A small sample size retrospective chart review revealed that most children diagnosed with COVID-19 had normal spirometry and plethysmography results [39]. Furthermore, a retrospective cohort study using EHR data from a single institution within the Children’s Hospital of Philadelphia Care Network found no association between SARS-CoV-2 PCR positivity and new asthma diagnoses in children aged 1–16 over an 18-month follow-up period (HR: 0.96; P = 0.79).8 Interestingly, another study indicated that an asthma diagnosis was negatively associated with COVID-19-related hospitalization in children [9]. To date, no strong evidence has been published in the literature to suggest a positive or negative association between COVID-19 and new-onset asthma in children.
However, our study reveals contrasting results, indicating that children vaccinated against COVID-19 who contracted the virus had an increased risk of developing new-onset asthma (HR = 2.745, 95% CI = 2.521, 2.99). This could be attributed to various factors, including immune response to the vaccine, the interaction between the vaccine and the virus, or other unrelated environmental or genetic factors.
Our subgroup analysis identified higher risks among younger age groups and Black or African American individuals. Following COVID-19 infection, infants developed a strong mucosal immune response marked by inflammatory cytokines, IFN-α, and Th-17 and neutrophil markers like IL-17, IL-8, and CXCL1 [40]. This response led to further respiratory inflammation and associated symptoms, which may explain why younger age groups have a higher risk of developing asthma. Regarding ethnicity, a large database analysis of adults across three national cohorts (UK, South Korea, Japan) found consistent results, indicating that post-COVID-19 effects on allergic diseases are not influenced by race [7]. However, the above study focused on adults and mainly included data from Asian countries. For children, we speculate that the immune response of Black individuals after COVID-19 infection may be influenced by genetics, socioeconomic status, and health disparities, but more research is needed to confirm this.
The strengths of our study include its use of a large, nationwide, population-based cohort and rigorous statistical analyses, including propensity score matching, to reduce selection bias. Moreover, our research provides valuable insights into the association between COVID-19 vaccination/infection and the incidence of new-onset asthma in children, an area currently seldom explored.
Our retrospective cohort analysis faced several limitations. The generalizability of our findings is affected by regional bias and variations in healthcare systems within the TriNetX database, which primarily includes U.S. data. This limits the applicability of our results to regions with different healthcare systems and demographics. Additionally, missing data is an issue, as some asthmatic patients, particularly children, may not have sought care from HCOs in the TriNetX network. Confounding bias is another concern; although we used Propensity Score Matching (PSM) to control for biases, unmeasured confounders such as family history of asthma and environmental exposures may still influence the results. Misclassification bias was mitigated by restricting COVID-19 diagnoses to PCR-positive cases. However, relying solely on ICD-10 codes without pulmonary function tests can reduce diagnostic accuracy. Using asthma medications as a secondary outcome helped enhance diagnostic precision. The study also overlooked the impact of COVID-19 variants and vaccination timing or type, which could significantly affect immune responses and asthma risk. Despite these efforts, the observational nature of our study limits the ability to confirm causality.

留言 (0)