
記住我

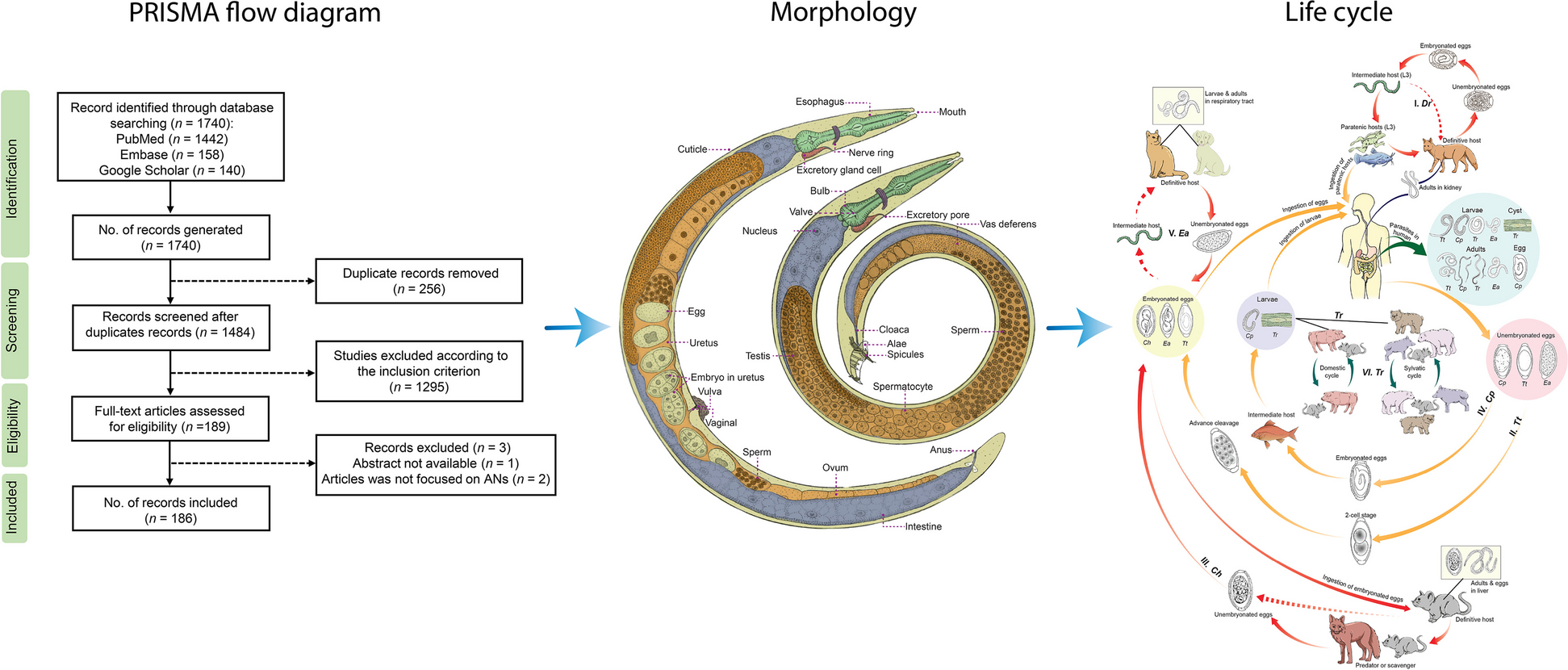
Based from the literature search, a total of 7074 articles were identified through database searching [PubMed (n = 1043), Web of Science (n = 4313), Google Scholar (n = 513), China National Knowledge Infrastructure (n = 577), and Wanfang (n = 628)]. After removal of duplicated records, 4814 articles were screened, 672 of which met the inclusion criteria. Following the full-text eligibility assessment, 470 articles were included in the review finally (Fig. 2). All literatures included were peer-reviewed articles. Moreover, Table 1 was created to exhibit the global distribution, temporal origins, and geographic origins of significant zoonotic digenetic trematodes in a more concise and organized manner.
Fig. 2
Flow diagram presenting the search process, including inclusion and exclusion criteria for articles screen
Table 1 The global distribution, temporal and geographic origins of significant zoonotic digenetic trematodesThe included studies were carried out in Asia (39.4%; n = 185), Africa (20.0%; n = 94), North America (9.8%; n = 46), South America (7.0%; n = 33), Europe (20.9%; n = 98), Oceania (3.0%; n = 14), and Antarctica (0.0%; n = 0).
Moreover, a comprehensive historical analysis of the published research has been conducted across distinct time periods: 1850–1900, 1901–1950, 1951–2000, and 2001–2023, encompassing 2, 10, 91, and 367 studies conducted in each respective era (Fig. 3).
Fig. 3
Total number of the research articles searching through PubMed, Web of Science, Google Scholar, CNKI and Wanfang databases
Global distribution and epidemiologySchistosoma Global distributionSchistosoma haematobium was first discovered in 1851 in Egypt by Bilharz during a necropsy [14, 15]. Subsequently, S. haematobium was found in Egypt and Iraq between 1901 and 1950 [16] (Additional file 3: Fig. S1a). Whereafter, S. haematobium was reported in Africa, the Middle East, and India from 1951 to 2000 [17] (Additional file 3: Fig. S1b). At present, S. haematobium is prevalent in Africa, the Middle East, and Europe [18]. Although Europe is not an endemic area, Schistosoma has been introduced through migration and travel [19]. In sub-Saharan Africa, S. haematobium is mostly distributed in Nigeria [20], Volta basin, Ghana, southwest Cameroun [21] and Mozambique [22]. Furthermore, it occurs in Portugal, Mauritius, Mesopotamia and Madagascar. A few cases have been reported in Mumbai and India (Additional file 3: Fig. S1c).
In 1902, Manson found eggs with lateral spine in the feces of an English patient [15]. Sambon proposed this new species named after Schistosoma mansoni in 1907 [15] (Additional file 3: Fig. S1a). From 1951 to 2000, S. mansoni was reported in the Middle East [23], Africa, Brazil, Venezuela, and the Caribbean [17] (Additional file 3: Fig. S1b). S. mansoni is primarily distributed in sub-Saharan Africa, the Middle East, some South American countries (Brazil, Venezuela, and Suriname), and the Caribbean islands [24], with sporadic reports in the Arabian Peninsula [23] and a few European countries [19]. In sub-Saharan African region, S. mansoni is mostly distributed in Ethiopia [25], Nigeria [20], Tanzania (Sengerema District, Nyamatongo Ward), north Ghana [21], Mozambique [22], Rwanda [26], and Democratic Republic of the Congo [27] (Additional file 3: Fig. S1c). Recently, a systematic review and meta-analysis in Ethiopia showed that the distribution area of S. mansoni exhibit environmental and ecological heterogeneities, where the soil’s silt and clay contents are higher than 22.0% [28].
In 1903, Kawanishi first discovered trematode eggs in stool examination of a patient. On May 30, 1904, Fujinami discovered a female parasite in the portal vein when performing an autopsy (Additional file 3: Fig. S1a). He designated it as a new species, Schistosoma japonicum [29]. From 1951 to 2000, cases of S. japonicum infection were reported in China, Japan, and the Philippines [30] (Additional file 3: Fig. S1b). S. japonicum used to be endemic in Japan, but was eliminated in 1996 [31]. Currently, it is mainly distributed in East Asia and Southeast Asia, including China, the Philippines [32], and a few regions of Indonesia such as Sulawesi [33, 34] (Additional file 3: Fig. S1c).
Schistosomiasis was initially reported in the Mekong River's Lower Basin region in 1957, specifically from the Laotian island of Khong to the Cambodian province of Kratie. At that time, S. japonicum was believed to be the cause, until a major revelation in 1978. This was when Neotricula aperta was discovered and Schistosoma mekongi, a unique species, was identified for the first time as the true cause of these cases [35,36,37] (Additional file 3: Fig. S1b). To date, S. mekongi is a restricted Schistosoma species found near the Mekong River, mainly in southern Lao PDR and northern Cambodia [38, 39] (Additional file 3: Fig. S1c).
EpidemiologyAccording to World Health Organization (WHO), an estimated 240 million people worldwide are infected with S. haematobium, while 90 million people are infected with S. mansoni, and 25 million people are infected with S. japonicum [40]. Approximately, 140,000 people are subject to the risk of infection by S. mekongi, with 80,000 found in Cambodia and a further 60,000 in Lao PDR [41]. Despite the number appearing small, continuous infection and re-infection contribute to the persistence of the disease within these susceptible populations. Notably, children are the most impacted due to their greater engagement with water [42]. Preventive measures for schistosomiasis include health education, improved water supply and sanitation, and mass drug administration of praziquantel, which is the recommended treatment for Schistosoma infection. Control and elimination programs for schistosomiasis are ongoing in many endemic countries.
Echinostoma and Isthmiophora Global distributionEchinostoma revolutum, the type species of the genus Echinostoma, was first reported by Froelich in Germany in 1802. However, the first reported human infection occurred in Taiwan province, China in 1929 [43] (Additional file 4: Fig. S2a). Between 1951 and 2000, E. revolutum was reported in China [44], Australia, New Zealand [45], USA [46], and Thailand [47] (Additional file 4: Fig. S2b). Currently, E. revolutum is the most widely distributed species among the known Echinostoma species and can be found in Asia (Bangladesh, China, India, Indonesia, Iran, Japan, Lao PDR, Malaysia, Republic of Korea, Thailand, and Vietnam), Oceania (New Zealand), Europe (Austria, Belarus, Bulgaria, Czech Republic, Finland, France, Germany, Greece, Hungary, Iceland, The Netherlands, Poland, Russia, Slovak Republic, UK, and Yugoslavia), and Americas (USA and Brazil), but rarely found in Africa [45, 46, 48,49,50,51]. However, reports in recent years show that outbreaks have been reported in North America after travellers returned from Eastern Africa including Kenya and Tanzania [52] (Additional file 4: Fig. S2c).
Another important species, Isthmiophora hortensis, was first reported by Asada in Japan in 1926 (Additional file 4: Fig. S2a). In 1964, I. hortensis was reported in Republic of Korea [53] (Additional file 4: Fig. S2b). The current global distribution of I. hortensis is primarily localized to East Asia, especially in China, Republic of Korea, and Japan [54] (Additional file 4: Fig. S2c).
EpidemiologyIn 2004, the WHO estimated the number of human infection for I. hortensis was approximately 50,000 [40]. The prevalence of E. revolutum among people in Taiwan province, China was estimated to be 2.8–6.5% [6]. Infection rates of E. revolutum were found to range from 7.5% to 22.4% among schoolchildren in Pursat Province, Cambodia [6]. However, the number of individuals currently infected or at risk of echinostomiasis remains unclear [55], highlighting the need for further research in this area.
Echinostoma are commonly found among birds and mammals in fresh water habitats, contributing to their ubiquitous presence. Echinostomiasis tend to be foci of infection in places where raw or undercooked intermediate hosts are eaten, so the most effective measure to prevent human infection is to eliminate the consumption of raw or undercooked freshwater snails, clams, fishes, or amphibians [5].
Echinochasmus Global distributionEchinochasmus japonicus was first reported in the experimental infection of dogs, cats, rats, mice and birds in Japan in 1926 [5] (Additional file 5: Fig. S3a). Natural infections of E. japonicus were reported in China [56] and Republic of Korea [57] from 1951 to 2000 (Additional file 5: Fig. S3b). Human infection of E. japonicus is mostly restricted in Asia. It has been reported in Japan, China, Republic of Korea, Kuwait, Lao PDR, Russia, Thailand, and Vietnam [6] (Additional file 5: Fig. S3c).
Echinochasmus perfoliatus was first identified in dogs in Romania by Motas and Straulescus in 1902 and was found in cats and dogs in Hungary by Ratz in 1908 (Additional file 5: Fig. S3a). In 1998, it was discovered in the Far East of Russia [58] (Additional file 5: Fig. S3b). Moreover, the natural and experimental infection in human was first found in Japan [59]. The epidemiology of E. perfoliatus infection is not only restricted in Asian area including China, Japan, Thailand, Republic of Korea, India, Vietnam, and the Philippines [5]. Cases or studies concerning the prevalence in the intermediate or definitive hosts were also reported from European countries like Denmark, England, Hungary, Russia, Poland, Ukraine, and Italy [5]. An infection of E. perfoliatus in gastrointestinal tract has been reported in Egypt on white ibis recently [60]. And similar finding was shown in Denmark on red foxes, another common reservoir host of E. perfoliatus [61] (Additional file 5: Fig. S3c).
EpidemiologyAs for E. japonicus, a larger-scale remote study conducted in Fujian and Guangdong province, China reported the prevalence rates in people, dogs and cats as 4.9%, 39.7% and 9.5%, respectively [59]. Furthermore, a study conducted in Lao PDR reported an overall infection rate in human was 3.1% [62]. Additionally, research has been conducted on the infection of E. japonicus in stray cats in various countries including Kuwait (1.6%) [63], and Republic of Korea (2.6% along the Geumgang river) [64]. Furthermore, a prevalence rate of 1.8% was reported for E. perfoliatus among individuals residing in the Guangdong, Fujian, Anhui, and Hubei provinces of China [6].
Like other reservoir hosts, including dogs, cats, ducks, and birds, humans are infected by eating the insufficiently cooked aquatic animals with encysted metacercariae. Hence, proper cooking of fish and improved sanitation and hygiene practices are essential to avoid the infection. Praziquantel is recognized as the first-line drug while albendazole as an alternative treatment option.
Paragonimus Global distributionParagonimus westermani is the most prominent species among the genus Paragonimus [65]. The first report on P. westermani could date back to 1877, when Kerbert detected it in the lungs of a Bengal tiger [66]. Between 1951 and 2000, P. westermani was reported in Japan, China, Republic of Korea, the Philippines, peninsular Malaysia, and Thailand [67] (Additional file 6: Fig. S4a). Currently, paragonimiasis (lung fluke disease), which is caused by the parasitic flatworm, is endemic to several parts of Asia, Africa, South America, and North America, but occurs primarily in China, the Philippines, Japan, Vietnam, Republic of Korea, Thailand, Malaysia, North Sumatra, and Indonesia [65, 67,68,69,70,71,72,73] (Additional file 6: Fig. S4b).
The first identified specimens of Paragonimus skrjabini were obtained from the lungs of a viverrid, Paguma larvata, located in Guangzhou city, Guangdong Province, China in 1959 [74] (Additional file 6: Fig. S4a). Initially, the species was classified as Paragonimus szechuanensis when the first report of infection occurred in Sichuan Province, China. Subsequently, further research revealed that P. szechuanensis was synonymous with P. skrjabini [75]. It is commonly found in Asia (China, India, Indonesia, Iran, Japan, Lao PDR, Malaysia, Republic of Korea, and Vietnam), Europe (Austria, Russia, and UK) and Americas [76,77,78] (Additional file 6: Fig. S4b).
EpidemiologyAn estimated 293.8 million individuals worldwide are at risk of Paragonimus infection, with China being the most heavily affected country, accounting for 195 million cases. Notably, P. westermani has been identified in multiple provincial-level administrative divisions across China, including Guangdong, Fujian, Yunnan, Guangxi, Guizhou, Hubei, Jiangxi, Hunan, Henan, Shaanxi, Gansu, Zhejiang, Sichuan, Hunan, Hainan, and Shanxi [78].
In certain endemic areas, the prevalence of paragonimiasis can be as high as 10% or more. To prevent the disease, it is recommended to cook crabs thoroughly and improve sanitation and hygiene practices. Praziquantel or triclabendazole are typically used as treatment for paragonimiasis.
Opisthorchiidae Global distributionClonorchis sinensis is the third most prevalent human fluke globally. The first reports of C. sinensis were made in 1874, nearly at the same time by MacConnell in India and MacGregor in Mauritius [79]. Between 1901 and 1950, reports of C. sinensis were documented in China and Japan [79] (Additional file 7: Fig. S5a). Furthermore, C. sinensis was reported in Republic of Korea, Vietnam, and the Far East of Russia between 1951 and 2000 [80] (Additional file 7: Fig. S5b). Nowadays, the endemic areas are mainly located in the Far East and East Asia, such as China, Republic of Korea, Vietnam, Russia, excluding Japan [6] (Additional file 7: Fig. S5c).
Opisthorchis felineus was first reported in the liver of cats, and human infection was first reported by Winogradoff in Tomsk, Siberia in 1892 [1, 81]. Between 1951 and 2000, it was reported in Kazakhstan, Italy, Albania, Greece, Switzerland, Holland, Germany, Poland, Ukraine, Bielorussia, Turkey, and Siberia [80] (Additional file 7: Fig. S5b). Eggs of O. felineus were found in fecal fossils of human and dog in Russia [82]. Nowadays, it’s worldwid
留言 (0)