
記住我



Despite the progress in oncology in the 21st century, distal rectal cancer treatment results frequently fall short of expectations. Having said that, patients who had a complex treatment that included chemoradiation therapy (CRT) neoadjuvant therapy, surgery, and multi-agent adjuvant chemotherapy (MAC) have shown better results. However, while the local recurrence rates still range between 5 and 10%, the rate of disease progression toward distant metastases can be as high as 20–30%, which is currently the main reason for a low rate of 5-year survival1–3. A lack of significant improvement in oncological results, as well as the debatable benefits of adjuvant therapy, prompted clinicians to offer two strategies for the implementation of comprehensive neoadjuvant therapy for distal rectal cancer4,5. The surgery, which is the main stage of the treatment for distal rectal cancer with a focus on the total mesorectal excision (TME) approach according to Heald and Ryall6, usage of the modern equipment and tools for open, laparoscopic, or robotic sphincter-sparing procedures did not ensure adequate success in oncological results. Surgical intervention types, procedures, and stages are constantly being studied and improved. A substantial comparison between the effects of sphincter-sparing surgery and rectum extirpation demonstrated better results after organ-sparing interventions, which should be favored as those with a lower probability of local recurrence and improved long-term oncological results7–10.
The purpose of our study is to evaluate the short-term and long-term oncological results of various types of sphincter-sparing surgeries in the complex treatment of stages II–III mid-ampullary and lower ampullary rectal cancer.
Materials and methodsThis study started in 2019 focusing on two cohort groups, with a retrospective review of the data collected between 2016 and 2019 and then a prospective analysis of the period from 2020 to 2022. Short-term and long-term oncological results in patients with distal rectal cancer following various types of sphincter-sparing surgical interventions were studied. Between 2016 and 2022, 634 (46.92%) of 1351 patients who underwent surgical treatment for rectal cancer at the Abdominal Oncosurgery Department, which is a clinical site for the Oncology Department, at Kyiv City Clinical Oncology Center in Ukraine, were diagnosed with mid-ampullary and lower ampullary rectal tumors.
Four hundred seventy patients were enrolled in the study. The inclusion criteria were as follows: age at least 18; diagnosed distal rectum adenocarcinoma of varying differentiation grades; stages II–III disease (T3–4N0M0 and TanyN1–2M0); patients who received a full course of neoadjuvant chemoradiotherapy (CRT) – long-course radiation therapy (44–55 Gy) combined with capecitabine or infusion of 5-Fu; sphincter-sparing surgery performed within 6–8 weeks following the completion of radiation therapy. All surgical interventions met the principles of the total mesorectal excision and ligation of the inferior mesenteric artery (IMA) immediately after it branches off the aorta. Anastomoses were formed using suturing devices or a manual double-layer suture, and a preventive stoma was applied or not, depending on the type of surgical intervention; adjuvant chemotherapy included 4–6 courses of FOLFOX (folinic acid–5-fluorouracil–oxaliplatin) or CAPOX (capecitabine–oxaliplatin).
The exclusion criteria were as follows: multiple primary rectal cancers; cancer relapses; distant metastases diagnosed during restaging; implantation metastases or intra-abdominal suppurative destructive diseases detected intraoperatively; incomplete treatment in the prospective group according to the inclusion criteria, incomplete information about the patient.
Based on the performed sphincter-sparing surgery, the following parameters were evaluated: quality of R0 resection; 30-day postoperative complications according to the Clavien–Dindo classification; the frequency and time of local recurrences, distant metastases; recurrence-free and overall survival.
Statistical analysis was performed using Statistical Software EZR v. 1.54 (a graphical user interface for R statistical software version 4.0.3, R Foundation for Statistical Computing, Vienna, Austria)11. Quantitative results were summarized using mean±SD (if normally distributed) or median value and interquartile range (if non-normally distributed); analysis of variance or the Kruskal–Wallis test was performed for the comparison, respectively. The chi-square (χ2) test and Fisher’s exact test were applied to compare frequencies. The risk of disease progression was presented as a hazard ratio (HR) with corresponding 95% CIs. The rate of recurrence-free survival was defined as the period between the date of surgery and the date of the last check-up when the recurrence was detected or not detected (local recurrence and/or distant metastases). Local recurrence was defined as disease recurrence within the pelvic cavity; metastatic lesions to the liver, lungs, or peritoneal implant were considered distant metastases. The Kaplan–Meier method was used to compute recurrence-free survival, and survival curves were compared using the log-rank test. The result was considered statistically significant when the P value was less than 0.05.
The work has been reported in line with the STROCSS criteria: Mathew G and Agha R, for the STROCSS Group. STROCSS 2021: Strengthening the Reporting of cohort, cross-sectional and case–control studies in Surgery. International Journal of Surgery 2021;96:106165.
In accordance with the Declaration of Helsinki, the research registration number: researchregistry9006 https://www.researchregistry.com/browse-the-registry#home/registrationdetails/645cd508d8f3b70029f7299d/.
ResultsOut of 470 patients with mid-ampullary and lower ampullary rectal cancer who met the inclusion criteria, 213 (45.32%) underwent low anterior resection (LAR), 138 (29.36%) had abdomino-anal resection (LAR with an extracorporeal anastomosis) (AAR), and 119 (25.32%) underwent intersphincteric resection (ISR). Table 1 summarizes the clinical characteristics of patients.
Table 1 - Patient characteristics stratified by sphincter-sparing surgery type. Parameter Low anterior resection (LAR) (n=213) Abdomino-anal resection (AAR) (n=138) Intersphincteric resection (ISR) (n=119) P Gender, n (%) Male 99 (46.48) 71 (51.45) 55 (46.22) 0.605 Female 114 (53.52) 67 (48.55) 64 (53.78) Mean age±σ (min–max), years 65.09±5.4 (33–84) 62.19±5.6 (39–86) 60.89±5.3 (38–82) >0.05 Median BMI (min–max), kg/m2 24 (18.3–43.2) 27 (19.4–44.5) 26 (18.9–42.7) >0.05 Neoadjuvant chemoradiotherapy, n (%) 213 (100.0) 136 (98.55) 117 (98.32) 0.184 pTNM stage, n (%) II (рТ3–4N0М0) 151 (70.89) 91 (65.94) 74 (62.18) 0.250 III (рТ2–4N1–2М0) 62 (29.11) 47 (34.06) 45 (37.81) Tumor differentiation grade, n (%) G1, G2 192 (90.14) 122 (88.41) 108 (90.75) 0.803 G3+mucosal adenocarcinoma 21 (9.86) 16 (11.59) 11 (9.24)Notes: Values were compared using the χ2 test. The comparison of quantitative data was performed by analysis of variance (ANOVA) or a nonparametric test, and the Kruskal–Wallis test.
No statistically significant differences were seen between the groups in terms of the type of sphincter-sparing intervention. Although there are more female patients in the LAR and ISR groups and more male patients in the AAR group, the difference is not statistically significant (P=0.605). The patients’ median BMI ranged from 24 to 27, and their average age at the time of surgery was at least 60 years, making them senior patients. There was no statistically significant difference between the groups in terms of age (P>0.05). In the groups stratified by surgery type, stage II (pT3–4N0M0) and stage III (pTanyN1–2M0) were found in 1/3 and 2/3 of the patients, respectively, with no statistically significant difference (P=0.250). Every 10th patient had G3+mucus-producing adenocarcinoma according to the findings of the morphological study of the tumor grade, with no statistically significant difference between groups (P=0.803). Table 2 shows the characteristics of surgical treatment based on the type of sphincter-sparing surgery.
Table 2 - Characteristics of surgical treatment stratified based on the type of sphincter-sparing surgery. Parameter Low anterior resection (LAR) (n=213) Abdomino-anal resection (AAR) (n=136) Intersphincteric resection (ISR) (n=117) P Median surgery duration (min–max), min 158 (110–240) 183 (120–320) 175 (120–270) >0.05 Distance from the lower tumor’s pole to the dentate line (mm), n (%) ≤30 35 (16.43) 79 (58.09) 113 (96.58) <0.001 >30 to ≤60 99 (46.48) 55 (40.44) 4 (3.42) >60 to ≤90 79 (37.09) 2 (1.47) 0 Median number of lymph nodes examined (25% quartile:75% quartile) 12 (9:24) 15 (10:25) 18 (12:26) <0.05 Preventive stoma, n (%) 168 (78.87) 9 (6.62) 7 (5.98) <0.001 Incidence of postoperative complications (Clavien–Dindo), n (%) No complications 129 (60.6) 100 (73.5) 87 (74.4) І–ІІ (mild complications) 29 (13.6) 17 (12.5) 14 (12) ІІІа (moderate) 11 (5.2) 6 (4.4) 5 (4.3) ІІІb–IVa (severe) 36 (16.9) 11 (8.1) 9 (7.7) IVb (life-threatening) 3 (1.4) 0 (0) 0 (0) 0.680 V (death of a patient), n (%) 5 (2.3) 2 (1.5) 2 (1.7)Notes: Values were compared using the χ2 test. The comparison of quantitative data was performed by analysis of variance (ANOVA) or a nonparametric test, and the Kruskal–Wallis test.
Two patients from the ISR and AAR groups who did not complete neoadjuvant chemoradiotherapy were excluded from the prospective cohort since they did not meet the criteria. Although the median operation time did not differ substantially between groups, patients in the ISR and AAR groups had 25–30-min lengthier surgeries than those in the LAR group. While evaluating the relationship between the frequency of sphincter-sparing surgeries and the distance from the lower tumor edge to the dentate line (pectinate line), it was found that only 16.43% of patients underwent LAR when the tumor was located 30 mm or less from the dentate line, whereas AAR and ISR were used in 58.09 and 96.58% of patients, respectively. When the tumor was between 30 and 60 mm from the dentate line, the equivalent surgeries were conducted in 46.48% LAR, 40.44% AAR, and 3.42% ISR of cases, respectively; with the distance from the tumor to the dentate line between 60 and 90 mm, the surgeries were done in 37.09% LAR, 1.47% AAR, and 0.0% ISR of cases, respectively. The difference between groups was found to be statistically significant in terms of intervention-type selection based on the distance from the tumor to the dentate line (P<0.001). The frequency of preventive stoma formation varied according to surgery type: for example, a stoma was created following LAR in 78.87% of patients, but only in 5.9 and 6.62% of patients after ISR and AAR, respectively, which was statistically significant (P<0.001).
While comparing postoperative complications (according to the Clavien–Dindo classification), there was no statistically significant difference (P=0.680) between groups for qualitative signs according to the χ2 test. However, when among the complications there was singled out group IIIb–IVa (severe complications), which included typical of the studied surgeries conditions, such as anastomotic leakage, necrotized perineum colon, abscess of the small pelvis, etc., it was revealed that the risk of typical complications in the LAR group (18.2%) was statistically significantly higher than in the AAR group (8.1%, P=0.021, according to Fisher’s exact test and the Bonferroni correction) and the ISR group (7.7%, P=0.019, according to Fisher’s exact test and Bonferroni correction). The difference was statistically significant (P=0.003). The difference in postoperative mortality after the sphincter-sparing surgeries examined was not statistically significant.
Adjuvant chemotherapy was completed in 442 patients following two different protocols: FOLFOX and CAPOX. The prescription varied between the study groups; even though FOLFOX was used more frequently than CAPOX, the difference in the use of the two protocols was not statistically significant (P=0.014).
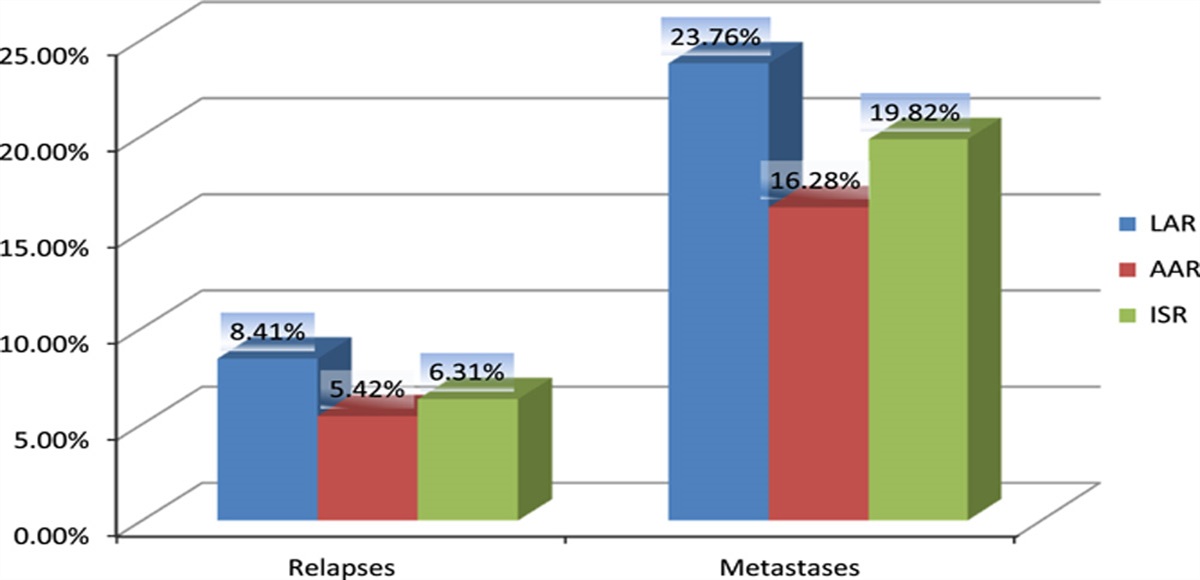
The bar chart shows the incidence of relapses and metastases in patients with mid-ampullary and lower ampullary rectal cancer who received comprehensive treatment while adhering to the specified inclusion and exclusion criteria. The final findings were evaluated in 202 patients who had LAR, 129 who had AAR, and 111 who underwent ISR. Local recurrences rates were 8.41%, 6.31%, and 5.42%, respectively, based on the type of surgery done, and metastases rates were 23.76%, 19.82%, and 16.28% (referring to Fig. 1). The difference was not statistically significant (P>0.05). The incidence of relapses and metastases is consistent, but it is incorrect to emphasize the presented findings because they are not censored and the associated risks depend on the duration of observation. The analysis will therefore be provided while presenting the disease-free survival plots.
 Figure 1:
Figure 1: The incidence of relapses and metastases based on the type of sphincter-sparing surgery. AAR, abdomino-anal resection; ISR, intersphincteric resection; LAR, low anterior resection.
When the obtained disease-free survival curves were analyzed based on the type of surgical intervention performed, a statistically significant difference (P=0.046 according to the log-rank test) was found, and the risk of the main disease progression turned out to be higher after LAR (P=0.02) than after AAR, with HR =1.7 (95% CI: 1.1–2.6) (referring to Fig. 2). Accordingly, 3-year recurrence-free survival rates were 68.8±3.3% after LAR, 77.1±4.0% after ISR, and 78.2±3.7% after AAR; 5-year recurrence-free survival rates were 65.4±3.6%, 71.7±4.6%, and 78.2±3.7%, respectively, with a statistically significant difference between the LAR group and the other two surgical groups (P=0.037) (referring to Table 3). Noteworthy is that, when standardized by patient age, the risk of primary disease progression in patients operated on with LAR was found to be higher (P<0.05) than in those operated on with AAR, HR =1.61 (95% CI: 1.03–2.52).
 Figure 2:
Figure 2: Disease-free survival based on sphincter-sparing surgery type. AAR, abdomino-anal resection; ISR, intersphincteric resection; LAR, low anterior resection.
Table 3 - 3-year and 5-year recurrence-free survival based on surgery type. Recurrence-free survival Abdomino-anal resection (AAR) Low anterior resection (LAR) Intersphincteric resection (ISR) 3-year survival 78.2±3.7% 68.8±3.3% 77.1±4.0% 5-year survival 78.2±3.7% 65.4±3.6% 71.7±4.6%The rates of 3-year recurrence-free survival, depending on the type of sphincter-sparing surgical treatment, were as follows: 68.8±3.3% after LAR, 77.1±4.0% after ISR, and 78.2±3.7% after AAR; the equivalent 5-year recurrence-free survival rates were 65.4±3.6%, 71.7±4.6%, and 78.2±3.7%, respectively (referring to Table 3). There was a statistically significant difference between the LAR group and the other two surgery groups (P=0.037). It should be mentioned that, when standardized by patient age, the risk of the main disease progression is higher (P<0.05) for patients operated on with the LAR method than for those operated on with the AAR method, HR =1.61 (95% CI: 1.03–2.52).
During the analysis, no statistically significant difference between the overall survival curves was found (P=0.320 according to the log-rank test) (referring to Fig. 3 and Table 4).
 Figure 3:
Figure 3: Overall survival based on the type of sphincter-sparing surgery performed. AAR, abdomino-anal resection; ISR, intersphincteric resection; LAR, low anterior resection.
Table 4 - Overall 3-year and 5-year survival based on the type of surgery. Overall survival Abdomino-anal resection (AAR) Low anterior resection (LAR) Intersphincteric resection (ISR) 3-year survival 86.6±3.0% 79.6±3.0% 87.1±3.3% 5-year survival 80.7±3.7% 72.1±3.6% 76.4±2.2%No statistically significant difference between the survival curves was found when standardizing by patient age.
There is a pressing need for ongoing debate among the oncological community and a search for treatment options due to the rising incidence of mid-ampullary and lower ampullary rectal cancer with unfavorable oncological results. It is now widely accepted that only thorough therapy can enhance the effects of treatment. Thus, according to the recommendations of NCCN (National Comprehensive Cancer Network) Version 1.20224, a strategy of total neoadjuvant therapy was adopted for this cancer localization; the search for improvement of the II stage of complex treatment, namely surgical treatment while taking into account a number of variables influencing the course of treatment. Considering one type of sphincter-sparing intervention – LAR, Bonjer et al12. compared types of access (laparoscopic vs. open) with a study of their influence on 30-day surgical complications and long-term oncological results of treatment of distal rectal cancer. Based on the results of the COLOR II study of 1044 patients from 30 hospitals who underwent surgery (699 in the laparoscopic surgery group and 345 in the open surgery group), after 3 years, the locoregional recurrence rate was 5.0% in both groups, and recurrence-free survival was 8% in the laparoscopic surgery group and 70.8% in the open surgery group. Overall survival was 86.7–83.6%, respectively.
In 2022, Japanese researchers also reported oncological results depending on the type of access (laparoscopic vs. open). They demonstrated that the frequency of anal sphincter preservation was higher in the laparoscopic group (60.0%) than in the open group (53.3%) (P=0.037). There was no statistically significant difference in the incidence of relapses, metastases, 3-year recurrence-free survival, or overall survival13,14. The authors addressed the issues related to the stages of surgery, specifically, high or low ligation of the inferior mesenteric artery and the level of lymph node dissection. They concluded that the degree of inferior mesenteric artery ligation had no effect on the incidence of anastomotic leakage and that there was no significant difference in oncological outcomes between low and high ligation15–18. However, a meta-analysis of 3119 patients from five cohorts has shown a significant overall survival benefit in patients with high versus low ligation of the inferior mesenteric artery19.
According to the NCCN guidelines, transanal tumor resection is recommended for effective total neoadjuvant therapy. The Norwegian authors, on the other hand, reported about 10 instances of local recurrence (9.5%) diagnosed in less than 11 months after transanal tumor resection, compared to 3.4% of local recurrences after conventional TME. The relapses differed from those seen following conventional TME in that the recurrent tumors were numerous and rapidly growing in the pelvic cavity and on the side walls20–22. As a result, transanal surgeries were halted awaiting the appointment of an audit.
By analyzing the short-term and long-term oncological outcomes after three types of sphincter-sparing surgeries, including LAR, ISR, and AAR, we presented the surgical experience of the complex treatment of mid-ampullary and lower ampullary rectal cancer. AAR, in our view, has been unjustly overlooked in modern literature. In this intervention, only the ideas of P. Kraske, G. Turner, and B. Black survive. This type of surgery can be adapted and adequately used due to advances in oncological science, thorough total mesorectomy (TME), the introduction of modern equipment and instruments, laparoscopic or robotic technologies, and improved stages of its implementation with the anal sphincter-sparing attitude. The reason that motivated to address AAR was the positive effect obtained from the neoadjuvant stage of treatment in male patients with a narrow pelvis, a fatty mesorectum, a high BMI, the anterior location of a large tumor, a distance from the tumor to the dentate line of less than 30 mm with no tumor involvement of the pelvic diaphragm or the external anal sphincter, and considerable post-radiation changes in the distal rectum.
We demonstrate the oncological outcomes of complex treatment for 442 patients with stages II–III mid-ampullary and lower ampullary rectal cancer who underwent three types of sphincter-sparing surgeries at the second stage of complex treatment. The results proved that each of the types has its specific indications and, with their adequate application, makes it possible to approach the surgical treatment of this category of patients in a personalized way.
The research showed the need to single out a group of postoperative complications that are typical for the types of surgery used, enabling them to be correctly assessed. Given that the incidence of recurrence and metastasis varied from 5.42 to 8.41% and 16.2 to 23.76%, respectively, improvement is required, but the patient category should be considered. In ~90% of cases, recurrences and metastases occurred within the first 2 years after surgery. After 3–6 months, every 10th patient whose detected relapses were unresponsive to complex treatment developed metastases and died within 9 months. Recurrences and metastases were found to be directly linked to recurrence-free survival, which, according to the study, stabilized only after 3 years, regardless of the type of surgery performed. In our research, we found no statistically significant effect of the type of sphincter-sparing surgery on overall survival.
ConclusionThe experience has shown that the surgeon’s arsenal should include several options for performing the sphincter-sparing surgical treatment, and advancements should be maintained by introducing contemporary technologies into the surgical technique. Under such circumstances, one can hope that the surgeon will select the type of surgery that will achieve the best results.
Ethical approvalThe clinical study was approved by the ethics commission of the National University of Health Care of Ukraine (protocol No. 14 dated 07.12.2020).
Sources of fundingNo particular funding was received for this review work.
Author contributionP.G. and M.G.: contributed to the planning and data collection of the review article; M.G.: wrote the original manuscript.
Conflicts of interest disclosureThe authors report no conflicts of interest.
Research registration unique identifying number (UIN) Name of the registry: Research Registry. Unique identifying number or registration ID: researchregistry9006. Hyperlink to your specific registration (must be publicly accessible and will be checked): https://www.researchregistry.com/browse-the-registry#home/registrationdetails/645cd508d8f3b70029f7299d/ GuarantorProkip Gordiichuk – MD, Dr.Sc. (Med), Professor, Head of the Department of Oncology, Shupyk National Healthcare University of Ukraine, Ministry of Health of Ukraine; Mykola Gordiichuk – MD, PhD student, Postgraduate of the Department of Oncology, Shupyk National Healthcare University of Ukraine.
References 1. Zaborowski A, Stakelum A, Winter DC. A systematic review of outcomes after total neoadjuvant therapy for locally advanced rectal cancer. Br J Surg 2019;106:979–987. 2. Bosset JF, Collette L, Calais G, et al. EORTC Radiotherapy Group Trial 22921. Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med 2006;355:1114–1123. 3. Sauer R, Liersch T, Merkel S, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol 2012;30:1926–1933. 4. National Comprehensive Cancer Network. NCCN Guidelines, Version 1.2022 Rectal Cancer. https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf 5. Gordiichuk P, Gordiichuk M. Оverview of discussions and decision-making on total neoadjuvant therapy of distal rectal cancer. Exp Oncol 2022;44:178–185. 6. Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1986;1:1479–1482. 7. Wang X-T, Li D-G, Li L, et al. Meta-analysis of oncological outcome after abdominoperineal resection or low anterior resection for lower rectal cancer. Pathol Oncol Res 2015;21:19–27. 8. Chambers W, Khan A, Waters R, et al. Examination of outcome following abdominoperineal resection for adenocarcinoma in Oxford. Color Dis 2010;12:1192–1197. 9. Campos-Lobato LF, Alves-Ferreira PC, Lavery IC, et al. Abdominoperineal resection does not decrease the quality of life in patients with low rectal cancer. Clinics (Sao Paulo) 2011;66:1035–1040. 10. Kim JC, Yu CS, Lim SB, et al. Abdominoperineal resection and low anterior resection: comparison of long-term oncologic outcome in matched patients with lower rectal cancer. Int J Color Dis 2013;28:493–501. 11. Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 2013;48:452–458. 12. Bonjer HJ, Deijen CL, Abis GA, et al. A randomized trial of laparoscopic versus open surgery for rectal cancer. N Engl J Med 2015;372:1324–1332. 13. Zhang C, Cui M, Xing J, et al. Oncological results in rectal cancer patients with a subcentimetre distal margin after laparoscopic-assisted sphincter-preserving surgery. ANZ J Surg 2022;92:1454–1460. 14. Hida K, Okamura R, Sakai Y, et al. Open versus laparoscopic surgery for advanced low rectal cancer: a large, multicenter, propensity score matched cohort study in Japan. Ann Surg 2018;268:318–324. 15. Luo Y, Li R, Wu D, et al. Long-term oncological outcomes of low anterior resection for rectal cancer with and without preservation of the left colic artery: a retrospective cohort study. BMC Cancer 2021;21:171. 16. Fujii S, Ishibe A, Ota M, et al. Short-term and long-term results of a randomized study comparing high tie and low tie inferior mesenteric artery ligation in laparoscopic rectal anterior resection: subanalysis of the HTLT (high tie vs. low tie) study. Surg Endosc 2019;33:1100–1110. 17. Yang X, Ma P, Zhang X, et al. Preservation versus non-preservation of a left colic artery in colorectal cancer surgery: an updated systematic review and meta-analysis. Medicine 2019;98:e13720. 18. Fan YC, Ning FL, Zhang CD, et al. Preservation versus non-preservation of the left colic artery in sigmoid and rectal cancer surgery: a meta-analysis. Int J Surg (London, England) 2018;52:269–277. 19. Singh D, Luo J, Liu XT, et al. The long-term survival benefits of high and low ligation of an inferior mesenteric artery in colorectal cancer surgery: a review and meta-analysis. Medicine 2017;96:e8520. 20. Peacock O, Chang GJ. Is the learning curve the Achilles heel of surgical innovation? —arguments against TaTME. Ann Laparosc Endosc Surg 2020;5:45. 21. Penna M, Hompes R, Arnold S, et al. International TaTME Registry Collaborative. Incidence and risk factors for anastomotic failure in 1594 patients treated by transanal total mesorectal excision: results from the International TaTME Registry. Ann Surg 2019;269:700–711. 22. Norwegian Colorectal Cancer Group. Nasjonalt handlingsprogram med retningslinjer for diagnostikk, behandling og oppfølging av kreft i tykktarm og endetarm. Helsedirektoratet; 2017.
留言 (0)