
記住我



Highlights
The epidemiological trend and spatial distribution of female breast cancer mortality in Suzhou were analyzed in this paper. The crude mortality rate (CR) of female breast cancer in Suzhou was on the rise in recent years, and there was obvious temporal and spatial aggregation. This report provides a scientific basis for the prevention and treatment of female breast cancer.Breast cancer is cancer with the highest incidence of women in the world1. According to the latest China Cancer Registry Annual Report, female breast cancer ranks first in the female cancer incidence spectrum and fifth in the female cancer death spectrum2. And the direct medical cost of breast cancer continues to rise in China3. Therefore, breast cancer is an important disease that affects women’s health and increases the burden of the disease. At present, most domestic tumor epidemiological studies use general characterization, but space-time characteristic analysis is rare. In recent years, with the rapid development of geographic information system technology, it can not only process attribute information such as words and numbers but also analyze graphics-based spatial information, so as to provide a powerful auxiliary role for disease prevention and control research. Therefore, this article used geographic information system to study the temporal and spatial changes of female breast cancer deaths in Suzhou and found areas with high and low incidences, which provided a localized scientific basis for the prevention and treatment of breast cancer in our city.
Materials and methods Data sourcesSuzhou is located in the Yangtze River Delta of China, covering an area of 8657 km2. It is composed of 10 districts, with a permanent resident population of about 12 million in 2020. Breast cancer mortality data from 2006 to 2020 sourced from the Resident Death Registration System. The relevant International Classification of Diseases, 10th Revision (ICD-10) code for breast cancer was C50. All data with C50 as the root cause of death in Suzhou are included in the statistics. The data of this study is from the disease surveillance system of the whole population and does not contain with any studies with human participants or animals performed, thus it is not necessary to obtain ethical approval. Population data were obtained from the Suzhou Statistics Bureau, including the population number of townships by sex. Electronic maps by townships of Suzhou were derived from the national database of basic geographical information. This research’s registration unique identifying number (UIN) is researchregistry8680 (https://www.researchregistry.com/register-now#user-researchregistry/registerresearchdetails/63ec65876461fb002845aa81/).
Quality controlThe cause of death registrations shall be borne by the community health centers and secondary or higher medical institutions within its jurisdiction. And the online reports are required within 14 days from the issuance date of death certificate, then audited by the Center for Disease Control and Prevention (CDC) within 7 days, followed by the periodical inspections by Suzhou CDC. CDCs at all levels should provide regular business-training among grassroots staff, on-site guidance at monitoring sites, as well as data comparisons with those from civil administration, public safety, or maternal and children healthcare, guarantying the accuracy and completeness of all data. The underreporting surveys covering the whole city are triennially conducted, with an underreporting rate of less than 5%.
MethodsThe spatial autocorrelation analysis was conducted in the statistical software GeoDa. Moran’s I method was used to analyze the global spatial autocorrelation of age-standardized mortality rate (ASMR) in breast cancer. Based on the global spatial autocorrelation coefficients being statistically different, further local spatial correlation analysis was carried out to produce local spatial autocorrelation aggregation plots.
We computed ASMR per 100 000 population using the world standard population. Trend analysis was expressed using annual percentage change (APC), APC=(eβ−1)×100%, β denoted regression coefficient. The curve estimation exponential distribution regression model was used to obtain the β value, and t-test was used to the APC4. A P-value less than 0.05 was considered to be statistically significant. And the work has been reported in line with the STROCSS criteria5.
Results Annual epidemic trendThe average annual breast cancer CR was 8.54 per 100 000 from 2006 to 2020 in Suzhou, and the ASMR was 7.38 per 100 000. The CR increased from 7.32 per 100 000 in 2006 to 9.26 per 100 000 in 2020, up 26.53% in the past nearly 15 years; trend analysis showed that the APC of the CR was 1.98% (1.30–2.66%) in the past nearly 15 years, and the difference was statistically significant (P<0.001), indicating the CR presented an overall trend to increase. Standardizing the breast cancer mortality in women, it presented that the rate decreased slightly and APC was −0.95% (−1.75% to −0.15%), and the difference was statistically significant (P=0.04) (Table 1).
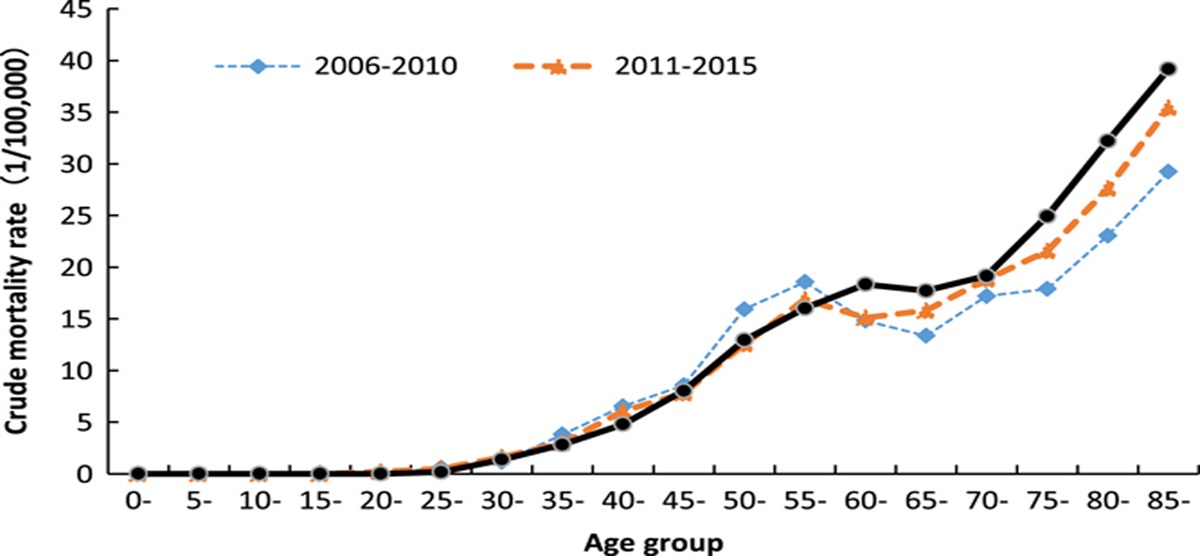
Table 1 - Annual change of female breast cancer mortality rate (one per 100 000) in Suzhou from 2006 to 2020 Year Crude mortality rate Age-standardized mortality rate 2006 7.32 9.03 2007 7.31 7.95 2008 8.23 8.28 2009 8.23 8.01 2010 7.36 7.02 2011 7.52 7.04 2012 8.25 7.27 2013 8.56 7.32 2014 8.91 7.48 2015 9.05 7.49 2016 8.49 6.79 2017 10.08 8.02 2018 9.89 7.88 2019 9.00 7.04 2020 9.26 7.03 APC (%) 1.98 −0.95 95% CI 1.30–2.66 −1.75 to −0.15 P 0.0001 0.04There were two peaks in the age-specific mortality of female breast cancer in Suzhou. The trend of the mortality rate was that it was at a low level before 35 years old, increased gradually after 35 years old, reached the first peak (17.14 per 100 000) between 55 and 59 years old, then decreased slightly, and increased remarkably from 70 years old, exceeded the first peak. Finally reached the highest level at 85 years old and the CR was as high as 35.69 per 100 000. Dividing these 15 years into three periods from 2006 to 2010, from 2011 to 2015, and from 2016 to 2020. The difference was that the first peak in the first two periods was in the 55- to 59-year age group, but the first peak in the period from 2016 to 2020 was in the 60- to 64-year age group, which was later than the first two periods. In all three periods, the mortality rate exceeded the first death peak at the age of 70 and reached the peak at the age of 85 (Fig. 1).
 Figure 1:
Figure 1: Age distribution of female breast cancer mortality rate (one per 100 000) in Suzhou from 2006 to 2020.
Analysis of aggregation in areas with high and low incidence of deathThe ASMR of female breast cancer in Suzhou was analyzed by spatial analysis, and the results of global spatial correlation analysis showed that the spatial autocorrelation coefficient (Moran’s I) was 0.32 (P<0.001), the difference was statistically significant, indicating that there was a certain degree of spatial aggregation of breast cancer death in Suzhou.
Further making the spatial aggregation map, there were 15 townships in Gusu Area in the high-high positive correlation represented by red, suggesting that these area were an area with a high incidence of breast cancer death. There were eight townships in low-low positive correlation represented by blue, scattered in Fuqiao Town, Shuangfeng Town, and Chengxiang Town and so on. The low-high areas represented by light blue were Hengtang Street and Shishan Street of High-tech Zone and so on, indicating that this low-incidence town was surrounded by surrounding high-incidence towns. The high-low areas represented by pink were Shengze Town in Wujiang District and Weitang Town in Xiangcheng District, indicating that the two high-incidence towns were surrounded by low-incidence towns (Fig. 2).
 Figure 2:
Figure 2: Local spatial autocorrelation clustering map of age-standardized mortality rate (1/100 000) of breast cancer in Suzhou from 2006 to 2020.
DiscussionIn 2020, about 685 000 of global breast cancer deaths accounted for 15.5% of female deaths. The global mortality rate of breast cancer is 17.7 per 100 000, and ASMR is 13.6 per 100 000. The difference of ASMR among countries around the world is nearly seven times. The highest ASMR is 41.0 per 100 000 in Fiji and the lowest is 6.4 per 100 000 in South Korea6. China’s breast cancer ASMR is 9.5/10 million, which is at a low level worldwide. However, the total number of breast cancer deaths in China is higher than that in other countries, accounting for 17.1% of the total breast cancer deaths worldwide. The female breast cancer ASMR in Suzhou was 7.03 per100 000 in 2020, which were both below the Chinese and the global average.
ASMR in breast cancer all over the world increases with age. Most countries reach their peak when they reach the age of 707. But there were two peaks in the age-specific mortality of female breast cancer in Suzhou, which was also showed in another equally developed city Guangzhou city8. The 55- to 59-year-old group of women with breast cancer was the first peak, and then it declined slightly and then increased rapidly after 70 years of age. The mortality rate increased rapidly with the increase of age when people older than 70. It was found that compared with 2006–2015, the first death age peak in our city in 2016–2020 was delayed by 5 years through analysis. For a long time, the media has paid more attention to the issue of cancer younger. As shown in the results, the age of female breast cancer death in Suzhou was not advanced but delayed. Studies in China show that the mortality rate of female breast cancer in China’s less than 60 years age group in 2017 is lower than that in 1990, and the mortality rate in 20- to 24-year age group is the largest decreased (62.96%), while mortality rate of the age group 60 years old and above was higher than that in 19908. The peak death rate of breast cancer in Suzhou has been postponed for 5 years, which may be related to the increase of life expectancy and prolongation of survival time of breast cancer patients in Suzhou.
This article found that the CR of female breast cancer in Suzhou has increased significantly in the past 15 years, with an annual growth rate of 1.98% (P<0.001). After excluding the influence of age composition, ASMR decreased slightly (APC=−0.90%, P=0.04). The change trend of female breast cancer in China was different from that in Suzhou. From 2005 to 2017, the CR and ASMR of female breast cancer were both showed upward trend9. Like Suzhou, the CR increased significantly in Feicheng, Shandong Province (APC=3.05%)10. The trend of breast cancer deaths among women in the USA and EU countries were opposite to that in China. Since 2010, the breast cancer mortality rate of women aged 40–79 has been continuously decreasing at a rate of 1.2−2.2% per year (P<0.001) in the USA11. Since 2001, female breast cancer mortality was observed to be down trending in 21 EU countries and the UK. Among them, Denmark had the highest change in ASMR and the highest estimated annual percentage change of −3.2%12. Suzhou is an economically developed city. The proportion of people over 65 years old has increased from 12.04% in 2006 rise to 19.87% in 2020. The high density of the population and serious aging of population may lead to the increase of crude death rate of female breast cancer in Suzhou. It can be seen that the CR of breast cancer in Suzhou was still showing an increasing trend, but it was mostly attributed to the impact of population aging. Although the trend of female breast cancer death in Suzhou was still flat compared with China, but compared with the USA, more needs to be done. To continuously improve the survival rate of breast cancer and continuously reduce its mortality, more attention should be paid to the early screening and diagnosis of female breast cancer, and early and standardized treatment.
Different from the traditional descriptive epidemiological methods, the spatial analysis of cancer death based on geographic information technology can more intuitively and accurately reflect the spatial distribution and aggregation analysis of cancer in Suzhou. Spatial analysis of breast cancer had also been carried out in the USA13, Peru14, Iran15, and Brazil16, which identifying the local high-incidence areas and providing data support for further tumor screening. In this article, the geographic information system was used to draw a map of the death distribution of female breast cancer in Suzhou, which was a rare study on the subdivision of the map to the township level in China. The results suggested that there were great differences in mortality among different villages and towns in Suzhou, in which the high-incidence map of death is concentrated in Gusu District. Gusu District is the ancient urban area of Suzhou, and it is also the gathering area of grade A hospitals in Suzhou. The convenience of medical treatment, the high economic level of residents and the serious aging of the population may be the influencing factors leading to the high incidence of breast cancer death in this areas. Studies had shown that genetic factors, environmental factors, and behavioral lifestyle factors were the main risk factors of breast cancer. Increasing age, advanced maternal, or nonpregnant women, family history of breast cancer, dense breast gland, hormone therapy, smoking and/or drinking alcohol, and high-calorie food intake were risk factors for breast cancer17,18. However, breastfeeding, regular work and rest, regular physical exercise, intake of fruits, vegetables, whole grains, and dietary fiber were protective factors that can appropriately reduce the risk of breast cancer19–21. It was suggested that we should strengthen breast cancer health promotion for the ancient city of Suzhou, advocate breastfeeding, healthy diet, and regular exercise, and increase the publicity of female breast cancer screening, especially focusing on the screening participation of high-risk groups.
There are some limitations in this paper, which are mainly manifested in the fact that there are only mortality-related data and there is no residents information such as diet, living habits, living environment, and family history cannot be further compared with explore possible risk factors. Therefore, investigation and research will be carried out on the above issues to scientifically determine the potential risk factors of breast cancer among female in Suzhou.
ConclusionsThis study showed that the CR of female breast cancer in Suzhou was on the rise in recent years, and there was obvious temporal and spatial aggregation, which laid the foundation for future research on the cause of breast cancer. In the next step, epidemiological surveys on genetics and lifestyle should be carried out in areas with high and low incidence, to find out the main causes of spatial aggregation, so as to take targeted intervention measures. At the same time, it is suggested that the areas with a high incidence of breast cancer should further increase the participation rate of female breast cancer screening by establishing targeted publicity, education, and physical examination reminders for high-risk groups according to the local actual situation, and intervene as soon as possible through the detection of early cancer, so as to improve the quality of life and reduce the risk of cancer death.
Ethical approvalThe data of this study is from the disease surveillance system of the whole population and does not contain with any studies with human participants or animals performed, thus it is not necessary to obtain ethical approval.
Sources of fundingThe present study was supported by the Research on key technologies for the prevention and control of major diseases and infectious diseases in Suzhou (grant no. GWZX201901) and Gusu Health Talent Training Project (no.: gsws2021054).
Author contributionAll the authors approved the final version of the manuscript.
Conflicts of interest disclosureThe authors declare that they have no financial conflict of interest with regard to the content of this report.
Research registration unique identifying number (UIN)researchregistry8680 (https://www.researchregistry.com/register-now#user researchregistry/registerresearchdetails/63ec65876461fb002845aa81/).
GuarantorYan Lu.
Data availability statementThe datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
AcknowledgementsThe project team would like to express their gratitude to all the staff engaged in the cause of death monitoring work in Suzhou.
References 1. Global Burden of Disease Cancer Collaboration, Fitzmaurice C, Abate D, Abbasi N, et al. Global, Regional, and National Cancer Mortality, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: a systematic analysis for the Global Burden of Disease Study. JAMA Oncol 2019;5:1749–1768. 2. Hao J, Wei WQ. 2019 China Cancer Registry Annual Report [in Chinese]. People’s Medical Publishing House; 2021:156–160. 3. Wang L, Zhang Y, Shi JF, et al. Disease burden of female breast cancer in China [in Chinese]. Zhonghua Liu Xing Bing Xue Za Zhi 2016;37:970–976. 4. Chen YS, Zhu J, Wang J, et al. Epidemic characteristics of stomach cancer mortality in Qidong during 1972–2016 [article in Chinese]. Zhonghua Zhong Liu Za Zhi 2022;44:99–103. 5. Mathew G, Agha R. for the STROCSS Group. STROCSS 2021: Strengthening the Reporting of cohort, cross-sectional and case-control studies in Surgery. Int J Surg 2021;96:106165. 6. Hyuna S, Jacques F, Rebecca LS, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–249. 7. Azadeh N, Juan Luis GM, Kevin EK, et al. Breast cancer mortality as a function of age. Aging 2022;14:1186–1199. 8. Luo A, Dong H, Lin X, et al. Time trends of major cancers incidence and mortality in Guangzhou, China 2004-2015: a joinpoint and age-period-cohort analysis. Cancer Med 2021;10:2865–2876. 9. Liu W, Wang LJ, Qi JL, et al. Disease burden of breast cancer in women in China, 1990-2017 [article in Chinese]. Zhonghua Liu Xing Bing Xue Za Zhi 2021;42:1225–1230. 10. Jia Y, Li Z, Nan Z, et al. Cancer death and potential years of life lost in Feicheng City, China: Trends from 2013 to 2018. Medicine 2021;100:e2737. 11. Hendrick RE, Helvie MA, Monticciolo DL. Breast cancer mortality rates have stopped declining in US women younger than 40 years. Radiology 2021;299:143–149. 12. Chinmay J, Ingrid S, Arashdeep R, et al. Trends in breast cancer mortality between 2001 and 2017: an observational study in the European Union and the United Kingdom. JCO Glob Oncol 2021;7:1682–1693. 13. Lia CS, Tzy-Mey K, Dora I, et al. Geo-spatial analysis of multiple cancers in individuals in the US, 2004-2014. Ann Cancer Epidemiol 2021;5:2–6. 14. Torres-Roman JS, Martinez-Herrera JF, Carioli G, et al. Breast cancer mortality trends in Peruvian women. BMC Cancer 2020;20:1173–1176. 15. Ebrahim B, Gholamreza R, Meysam O, et al. Geo-epidemiological reporting and spatial clustering of the 10 most prevalent cancers in Iran. Geospat Health 2021;16:94–97. 16. Silva JDDE, Rosseto de Oliveira R, da Silva MT. Breast cancer mortality in young women in Brazil. Front Oncol 2021;10:569933. 17. Jessica AT, Emma RM, Paul RW. Lifestyle interventions through participatory research: a mixed-methods systematic review of alcohol and other breast cancer behavioural risk factors. Int J Environ Res Public Health 2022;19:980. 18. Wang YC, Lin CH, Huang SP, et al. Risk factors for female breast cancer: a population cohort study. Cancers (Basel) 2022;14:788. 19. Qiu RB, Zhong YJ, Hu MM, et al. Breastfeeding and reduced risk of breast cancer: a systematic review and meta-analysis. Comput Math Methods Med 2022;2022:1–9. 20. Adair KM, Alpa VP, DF W, et al. Proportion of cancer cases attributable to physical inactivity by US State, 2013-2016. Med Sci Sports Exerc 2022;54:417–423. 21. Cody ZW, Julie AS, Yashvee D, et al. Risk of cancer in regular and low meat-eaters, fish-eaters, and vegetarians: a prospective analysis of UK Biobank participants. BMC Med 2022;20:73.
留言 (0)