
記住我



Highlights
Protein kinase inhibitor therapies are associated with the risk of kidney injury. Entrectinib has an unusually high potential for adverse renal effects. In the diagnostical work-up of tubulointerstitial nephritis (TIN), kidney biopsy plays a cardinal role. In the case of enterctinib-induced TIN, steroid therapy might improve renal function.The use of protein kinase inhibitors as antitumor agents is increasingly gaining ground in the last few years. In 2022, 72 small-molecule protein kinase inhibitors were approved by the FDA (Food and Drug Administration)1. Furthermore, numerous new medications are currently under development and already in clinical phase trials. These drugs target one or more protein kinases, thus inhibiting signal pathways, which are essential for tumor proliferation and progression. Although they provide novel, personalized therapeutic possibilities and are usually better tolerated than traditional chemotherapies, a rapidly growing number of adverse events and side effects are being reported2.
Entrectinib is a novel protein kinase inhibitor, and it was approved in 2019 for the treatment of ROS1 (ROS proto-oncogene 1, receptor tyrosine kinase) fusion-positive non-small cell lung cancer (NSCLC). Multiple studies have confirmed its potent antitumor effect. It was specifically developed for targeting intracranial metastasis due to its blood–brain barrier penetrability. No severe safety concerns have been raised in connection with its use; however, there are data suggesting unusual potential renal toxicity2.
MethodsThis case report has been reported in line with the SCARE (Surgical CAse REport) Criteria3.
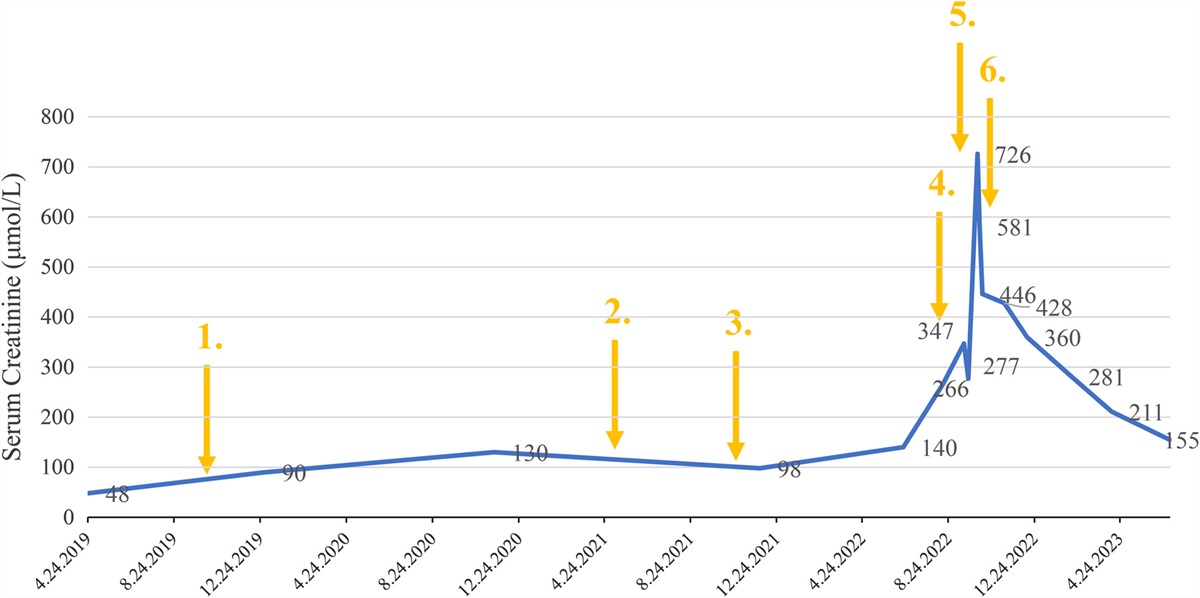
Case presentationHere we present a case of a 71-year-old Caucasian woman, who was diagnosed with lung cancer in April 2019 after seeking medical attention owing to progressive dyspnea. Upon pulmonological examination she underwent a chest-CT (computer tomography), which showed a 16 mm lower-lobe mass in the left lung. In May, a core biopsy was taken, and the histological evaluation revealed the presence of pulmonary adenocarcinoma. Further molecular tumor profiling of the sample confirmed 85% positivity of ROS1 translocation. As part of tumor staging, bone scintigraphy was ordered, which showed a unifocal bone metastasis in the eighth thoracic vertebra. In November 2019, crizotinib therapy was started, which continued till July 2021, when her follow-up brain MRI (magnetic resonance imaging) showed the presence of new multiplex cerebellar metastases. In September 2021, she received whole-brain radiotherapy (10×300 cGY) and was prescribed entrectinib. Having been treated with entrectinib for almost a year, in July 2022, an imaging examination confirmed regression in the intracranial metastases. In the middle of September 2022, she was admitted to our nephrology department because of acute-on chronic kidney failure. Figure 1 demonstrates serum creatinine levels throughout the course of the disease.
 Figure 1:
Figure 1: Changes in serum creatinine levels. Creatinine is shown in μmol/l. 1. Crizotinib therapy was started. 2. Crizotinib was stopped. 3. Entrectinib therapy was started. 4. Entrectinib was stopped. 5. Kidney biopsy. 6. Methylprednisolone therapy was started.
Upon admission, we ran further laboratory tests to evaluate our patient’s kidney function precisely and to find the culprit factor. We discontinued entrectinib for its possible negative renal effect. The patient had been on furosemide, rosuvastatin, iron supplementation, and perindopril therapy, and the latter was discontinued due to acute kidney impairment. She had no known allergies. Her electrolytes were in the normal range, and acute hemodialysis was not needed. Pathological but non-nephrotic proteinuria was seen (urinary protein–creatinine ratio was 199 mg/mmol, urinary albumin creatinine ratio was 16 mg/mmol), and serum protein electrophoresis and immunofixation were negative. Urine electrophoresis and immunofixation revealed polyclonal immunoglobulins. Abdominal ultrasound showed normal kidney sizes and structures; no postrenal anomaly was detected. Urine sediment analysis showed the presence of white blood cell casts (Fig. 2), while urinary culture was negative. Based on the clinical picture and laboratory findings, tubulointerstitial nephritis (TIN) appeared plausible. To make an accurate diagnosis, she was scheduled for renal biopsy, which was, however, postponed due to an ongoing SARS-CoV2 (severe acute respiratory syndrome coronavirus 2) infection. After sanitation of SARS-CoV2 infection, she presented with worsening laboratory parameters; retention markers were further increasing, and severe metabolic acidosis was also seen. Urine sediment was once again analyzed; this time, dark brown granular casts were present as well, indicating additional acute tubular necrosis (ATN). In October 2022, a renal biopsy was performed by an attendant nephrologist. The procedure was well tolerated by the patient and there were no complications.
 Figure 2:
Figure 2: Leukocyte-cast in the urine. Urinary sediment examination, magnification 400×.
The renal biopsy sample confirmed acute TIN (Fig. 3). In brief, it showed interstitial inflammatory cell infiltration, which dominantly consisted of lymphocytes and plasma cells along with scattered eosinophil granulocytes. Tubulitis was also found; in some tubular lumina, granular casts were visible. Further tubules displayed acute tubular necrosis with pronounced regenerative epithelial atypia. Interstitial fibrosis and tubular atrophy occupied 20–25% of the cortex. No significant arteriosclerosis was present. There was no immunocomplex deposition by immunofluorescence and electron microscopy.
 Figure 3:
Figure 3: Kidney biopsy. (A) Severe acute tubular necrosis with flattened proximal tubular epithelium. Preserved light microscopic glomerular structure. Formalin-fixed, paraffin-embedded tissue, hematoxylin and eosin, light microscopy, magnification 240×. (B) Acute tubular necrosis and lymphoplasmacytic infiltrate with scattered eosinophil granulocytes. Formalin-fixed, paraffin-embedded tissue, hematoxylin and eosin, light microscopy, magnification 400×.
After starting steroid therapy (methylprednisolone 32 mg orally), a significant improvement in renal function was observed and hemodialysis could be avoided, which improved the quality of life of the patient. Methylprednisolone therapy was tapered after 2 weeks and stopped in 10 weeks.
In the meantime, she underwent staging CT again, which showed unequivocal progression of the tumor: not only significant para jugular and mediastinal lymphadenomegaly were detected, but a new cerebral metastasis was also discovered.
Hemodialysis was evitable, and the patient’s renal function slowly improved (serum creatinine level was 155 μmol/l in July 2023). Based on the tumor board’s decision, oncological treatment was not available in her case, as the disease was progressive during protein kinase inhibitor therapy. The patient died of pulmonary complications in August 2023.
DiscussionAcute TIN is a common cause of acute kidney injury with an increasing prevalence; however, it is often not recognized4. The vagueness of the diagnosis is rooted in the frequent oligosymptomatic clinical picture and the need for invasive diagnostics. Numerous etiologies might cause TIN in susceptible persons, such as drugs, infections, systemic and autoimmune diseases, genetic predisposition, and idiopathic factors5. As pharmacological developments have brought up the availability of an immense amount of new medications, drug-induced TIN has become the leading cause of TIN6. The putative underlying pathomechanism is type IV hypersensitivity. Theoretically, any drug can induce TIN; proton pump inhibitors, antibiotics, and non-steroidal anti-inflammatory drugs are most associated with it7.
Typically, the presentation of symptoms and renal function decline occur days or weeks after the initiation of the new drug. Most symptoms are mild and nonspecific, such as nausea, malaise, and fever. Systematic manifestations, for instance, skin rashes and itching might draw attention to the causative role of the given medications. Urine analysis is essential for the diagnosis. Non-nephrotic proteinuria, sterile pyuria, hematuria, leukocyte casts, and sometimes eosinophiluria are the most common findings. Nevertheless, only a kidney biopsy can deliver a definitive diagnosis. Histological findings include dominantly interstitial lymphocytic infiltration, not rarely eosinophils, plasma cells, and polymorphonuclear cells can also be found8.
Entrectinib is a selective inhibitor of the proto-oncogene tyrosine-protein kinase ROS1, the anaplastic lymphoma kinase (ALK), and the tropomyosin receptor tyrosine kinases (TRKA/B/C)9. It was approved by the FDA in 2019 for the treatment of ROS1 fusion-positive NSCLC. Its central nervous system penetrability makes it particularly preferred for NSCLC patients with intracranial metastases. Most of its reported side effects are grade 1 or 2, and no significant safety issues were observed during the integrated analysis of three phase 1–2 trials10. However, ALK inhibitors have been brought into connection with adverse renal effects, such as acute tubular injury, podocytopathies, pseudo-acute kidney injury, cyst formation, electrolyte disturbances, peripheral edema, etc.11. In a case report from 2018, alectinib, a second-generation ALK inhibitor, was associated with progressive renal insufficiency by causing a combination of TIN and diffuse podocyte damage12. A recent study assessing acute kidney injury related to small protein kinase inhibitors found that entrectinib had the highest reporting odds ratio during disproportionality analysis2.
In our patient’s case, upon differential diagnosis, prerenal and renal components of kidney failure were both feasible. Since the significant deterioration of kidney function started in the summer, dehydration might have been one factor. Nonetheless diarrhea, as a possible side effect of entrectinib, could have also played a pivotal role as a prerenal cause. Nevertheless, serum urea and creatinine ratio did not indicate prerenal cause. Furthermore, having received parenteral fluid supplementation, no ground-breaking renal function improvement was observed, which supported the causative role of renal parenchymal etiology. The timeline of the renal function changes (Fig. 1) supports the causative effect of the protein kinase inhibitors: even the first administration of crizotinib was followed by a mild renal impairment, while the patient’s renal function was better again when no protein kinase inhibitor was administered. The kidney function loss was escalated after entrectinib was started. Other new medicines were not started during that period. Histological examination revealed inflammatory cell infiltration with dominantly lymphocytic cells, but plasma cells and eosinophil granulocytes were also present, which confirmed our primary diagnosis, the acute TIN (Fig. 3). Although, signs of acute tubular necrosis were visible, it is unlikely to be related to entrectinib: at first admission urinary sediment analysis showed only white blood cell casts (Fig. 2), while ATN casts appeared much later, 3 weeks after entrectinib was ceased. The examination of the urinary sediment is still a crucial tool in the diagnostics of acute kidney injury, as ATN can be easily recognized from the urinary sediment. The lack of red blood cell casts and acanthocytes in the urine can exclude proliferative glomerular diseases. Here, ATN might have been associated with the recent SARS-CoV2 infection, fever, or hypotension. The significant responsiveness to steroid therapy with the disappearance of white blood cell casts from the urine enhances the role of TIN behind the primary kidney function loss.
ConclusionsTo our knowledge, this is the first published case report of biopsy-confirmed entrectinib-induced TIN. Protein kinase inhibitors may cause kidney injury through different pathomechanisms. To be able to provide adequate treatment, it is crucial to differentiate between the underlying pathologies, and kidney biopsy should be considered. Our case report emphasizes the fact that in case of kidney function decline during entrectinib therapy, the possibility of TIN must be examined, as corticosteroid therapy may improve this condition.
Ethical approvalNot applicable.
ConsentWritten informed consent was obtained from the patient for the publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Sources of fundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Open access publication was supported by Semmelweis University, Budapest, Hungary.
Author contributionM.S. and N.L.: involved in the patient’s care and wrote the manuscript; D.D.: provided the histopathology report of the kidney sample. All authors read and approved the final manuscript.
Conflicts of interest disclosureThe authors declare that they have no conflicts of interest.
Research registration unique identifying number (UIN)Not applicable.
GuarantorNóra Ledó, corresponding author.
Provenance and peer reviewThe paper was not invited.
Data availability statementData sharing does not apply to this article as no datasets were generated or analyzed during the current study.
AcknowledgementsThe authors thank the patient and her family.
References 1. Roskoski R Jr. Properties of FDA-approved small molecule protein kinase inhibitors: a 2023 update. Pharmacol Res 2023;187:106552. 2. Fan Q, Ma J, Zhang B, et al. Assessment of acute kidney injury related to small-molecule protein kinase inhibitors using the FDA adverse event reporting system. Cancer Chemother Pharmacol 2020;86:655–662. 3. Agha RA, Franchi T, Sohrabi C, et al. The SCARE 2020 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int J Surg 2020;84:226–230. 4. Praga M, Sevillano A, Auñón P, et al. Changes in the aetiology, clinical presentation and management of acute interstitial nephritis, an increasingly common cause of acute kidney injury. Nephrol Dial Transplant 2015;30:1472–1479. 5. Joyce E, Glasner P, Ranganathan S, et al. Tubulointerstitial nephritis: diagnosis, treatment, and monitoring. Pediatr Nephrol 2017;32:577–587. 6. Sanchez-Alamo B, Cases-Corona C, Fernandez-Juarez G. Facing the challenge of drug-induced acute interstitial nephritis. Nephron 2022;147:78–90. 7. Gérard AO, Merino D, Laurain A, et al. Drug-induced tubulointerstitial nephritis: insights from the World Health Organization Safety Database. Kidney Int Rep 2022;7:1699–1702. 8. Paueksakon P, Fogo AB. Drug-induced nephropathies. Histopathology 2017;70:94–108. 9. Frampton JE. Entrectinib: a review in NTRK+ solid tumours and ROS1+ NSCLC. Drugs 2021;81:697–708. 10. Doebele RC, Drilon A, Paz-Ares L, et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: integrated analysis of three phase 1–2 trials. Lancet Oncol 2020;21:271–282. 11. Bonilla M, Jhaveri KD, Izzedine H. Anaplastic lymphoma kinase inhibitors and their effect on the kidney. Clin Kidney J 2022;15:1475–1482. 12. Nagai K, Ono H, Matsuura M, et al. Progressive renal insufficiency related to ALK inhibitor, alectinib. Oxf Med Case Reports 2018;2018:omy009.
留言 (0)