
記住我



Highlights
Neoadjuvant chemotherapy (NAC) is a standard treatment option in locally advanced BC patients. Pegylated liposomal doxorubicin has the same efficacy in NAC for HER2-negative BC. Pegylated liposomal doxorubicin is safe and reliable for NAC in BC patients.Breast cancer is currently the main incident of malignant tumors in women1,2, and its occurrence is increasing yearly, with an annual rate of 30 to 40/100 000 in general and 70/100 000 in women over the age of 60. Although the use of breast cancer chemotherapy has significantly improved the therapeutic impact over the disease since the 1970s, chemotherapy is a double-edged sword, and the associated side effects are significant reasons limiting its use. Anthracyclines are the first-line drugs of choice in breast cancer chemotherapy. Various clinical trials have confirmed their cornerstone status in breast cancer chemotherapy. However, their adverse reactions, especially the dose-dependent cardiotoxicity, limit the total amount of anthracyclines used3,4. For elderly patients or breast cancer patients with previous heart diseases, the use of anthracyclines has also been affected5,6. In an expert consensus on the prevention and treatment of anthracycline cardiotoxicity, it is recommended that novel dosage forms with reduced cardiotoxicity, such as pegylated liposomal doxorubicin (PLD), may be used to decrease the cardiotoxic effects of these drugs. Neoadjuvant chemotherapy (NAC) has become a standard treatment option in operable and locally advanced breast cancer patients7. After receiving NAC, patients achieve superior pathological complete response (pCR), and survival outcome improves considerably8,9. According to earlier research, PLD is most often used in advanced breast cancer treatment10. However, there are just a few reports in the field of NAC for breast cancer, particularly for HER2-negative disease. Considering this, the author analyzed 107 patients records with HER2-negative breast cancer who underwent TA (PLD 35 mg/m2, docetaxel 75 mg/m2) or TE (epirubicin 100 mg/m2, docetaxel 75 mg/m2) regimen NAC from January 2018 to December 2020.
Materials and methods PatientsA total of 107 patients with HER2-negative breast cancer undergoing NAC from Xingtai People’s Hospital in Hebei Province from January 2021 to December 2022 were treated with TA or TE regimens for 6 cycles, once every 3 weeks. From the total, 57 patients were treated with TA (PLD 35 mg/m2, docetaxel 75 mg/m2), and 50 patients treated with TE regimen (epirubicin 100 mg/m2, docetaxel 75 mg/m2). The inclusion criteria were as follows: (1) women aged 18–70 years; (2) primary BC (clinical stage IIa–IIIc and lymph node positivity) confifirmed via histological examination with a measurable tumor; (3) scheduled for NAC; (4) Karnofsky (KPS) score≧70; (5) provision of written informed consent.
The exclusion criteria included cardiac disease (New York Heart Association class II) and severe systemic infection. The patients were excluded if they were allergic, highly sensitive, or intolerant to PLD, epirubicin, or its excipients.
At screening, the researchers ensured that subjects met all inclusion criteria. Subjects were removed from the trial if their condition, including the laboratory results, had changed after screening and before administration of the first dose of the study drug.
Methods Basic informationThe clinicopathological characteristics of the patients were counted and recorded, and after the discrimination between the PLD and the epirubicin groups, they were compared. The work has been reported in line with the strengthening the reporting of cohort, cross-sectional, and case–control studies in surgery (STROCSS) criteria11. We have registered the study in www.researchregistry.com, and the Research Registry UIN is researchregistry9849 with a hyperlink to https://www.researchregistry.com/browse-the-registry#home/.
Clinical assessmentsPatients received a combination regimen with PLD (35 mg/m2) or epirubicin (100 mg/m2) every 3 weeks by 6 cycles of intravenous (iv) infusion. The chemotherapy regimen and intensity were selected based on the St. Gallen recurrence risk assessment. Dosage changes for either drug are permitted under this regimen for hand-foot syndrome, hematologic toxicity, and other grades 3 and 4 adverse events. NAC was discontinued when the tumor shrunk, reaching the goals of breast-conserving surgery or radical mastectomy. In addition, postoperative treatment strategies were developed according to the guidelines of the National Breast Cancer Network. Radiation therapy for breast-conserving and lymph node metastases; endocrine therapy for estrogen receptor/progesterone receptor (ER/PR) positive patients.
All patients underwent ultrasound and mammography for local disease assessment, and breast MRI as candidates for breast-conserving surgery. Core needle biopsies of all breast tumors and fine needle biopsies of enlarged lymph nodes were also performed. In addition, pathological evaluation included tumor histology and ER/PR/HER2/Ki67 IHC staining. ER/PR-positive tumors were defined as >1% expression, and HER2-positive was defined as amplification by IHC3+ or FISH detection. Tumor size and regional lymph nodes were assessed in each patient using ultrasound after every two cycles of chemotherapy. For patients planning breast-conserving surgery, MRI is performed every 3–4 cycles of chemotherapy. Clinical tumor response was evaluated using the Response Evaluation Criteria in Solid Tumors Criteria version 1.012,13. In addition, patients with no invasive or in situ carcinoma in breast specimens and no residual cancer were defined as complete pCR, regardless of axillary or regional lymph node status. During treatment, administer signs, performance status, adverse events, complete blood counts, and serum chemistry assessments weekly or more frequently as needed. Cardiac ultrasonography is performed before the initiation of NAC, when the patient develops heart-related symptoms, or every 2–3 chemotherapy cycles for the entire chemotherapy cycle, and every 3 months thereafter for at least half a year. All side effects were assessed according to WHO and American Society of Clinical Oncology criteria.
Ethical approvalThe present study was approved by the Ethics Committee of Xingtai people’s hospital (approval no. 2021[030]). The present study was conducted in accordance with the principles described in The Declaration of Helsinki.
Statistical analysisThis set of counting data was processed using the SPSS 23 statistical software package. The t-test was used for basic situation comparisons, and the logistic regression analysis was used for multifactorial analysis. The Crosstabs χ2 test accessed the chemotherapy effect and adverse reaction analysis. P-value <0.05 was considered statistically significant.
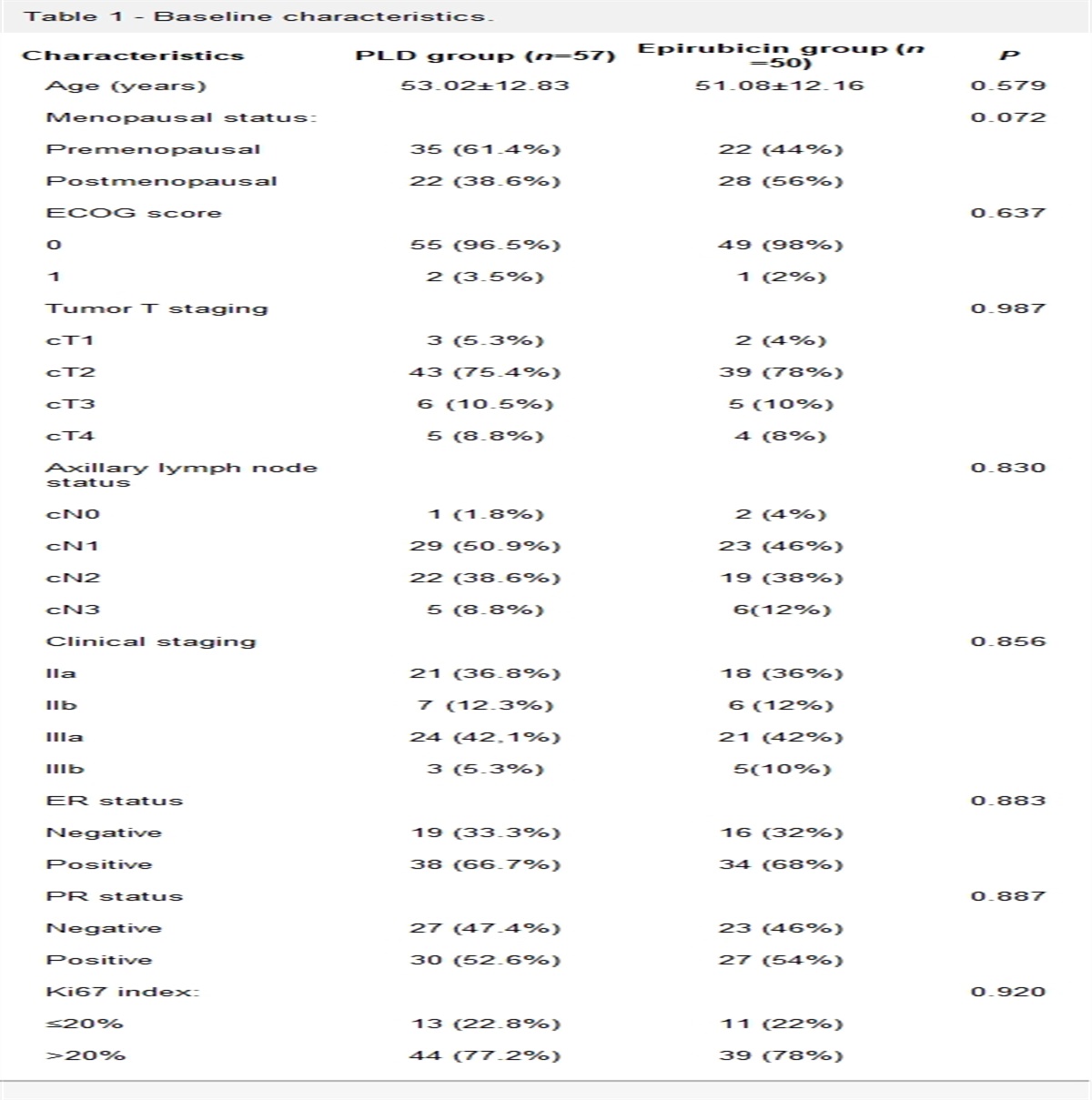
Results Patient characteristicsThe PLD and epirubicin groups were demographically including age, Eastern Cooperative Oncology Group score, menstrual status, ER/HER2/Ki67 status, molecular subtype, clinical T stage, preoperative chemotherapy cycle, histology, etc. and were comparable in disease characteristics (Table 1).
Table 1 - Baseline characteristics. Characteristics PLD group (n=57) Epirubicin group (n=50) P Age (years) 53.02±12.83 51.08±12.16 0.579 Menopausal status: 0.072 Premenopausal 35 (61.4%) 22 (44%) Postmenopausal 22 (38.6%) 28 (56%) ECOG score 0.637 0 55 (96.5%) 49 (98%) 1 2 (3.5%) 1 (2%) Tumor T staging 0.987 cT1 3 (5.3%) 2 (4%) cT2 43 (75.4%) 39 (78%) cT3 6 (10.5%) 5 (10%) cT4 5 (8.8%) 4 (8%) Axillary lymph node status 0.830 cN0 1 (1.8%) 2 (4%) cN1 29 (50.9%) 23 (46%) cN2 22 (38.6%) 19 (38%) cN3 5 (8.8%) 6(12%) Clinical staging 0.856 IIa 21 (36.8%) 18 (36%) IIb 7 (12.3%) 6 (12%) IIIa 24 (42,1%) 21 (42%) IIIb 3 (5.3%) 5(10%) ER status 0.883 Negative 19 (33.3%) 16 (32%) Positive 38 (66.7%) 34 (68%) PR status 0.887 Negative 27 (47.4%) 23 (46%) Positive 30 (52.6%) 27 (54%) Ki67 index: 0.920 ≤20% 13 (22.8%) 11 (22%) >20% 44 (77.2%) 39 (78%)The effects of chemotherapy in the PLD and epirubicin groups were similar, with RR reaching 82.5 and 78%, respectively, with a P-value of 0.563, which was not statistically significant (Table 2).
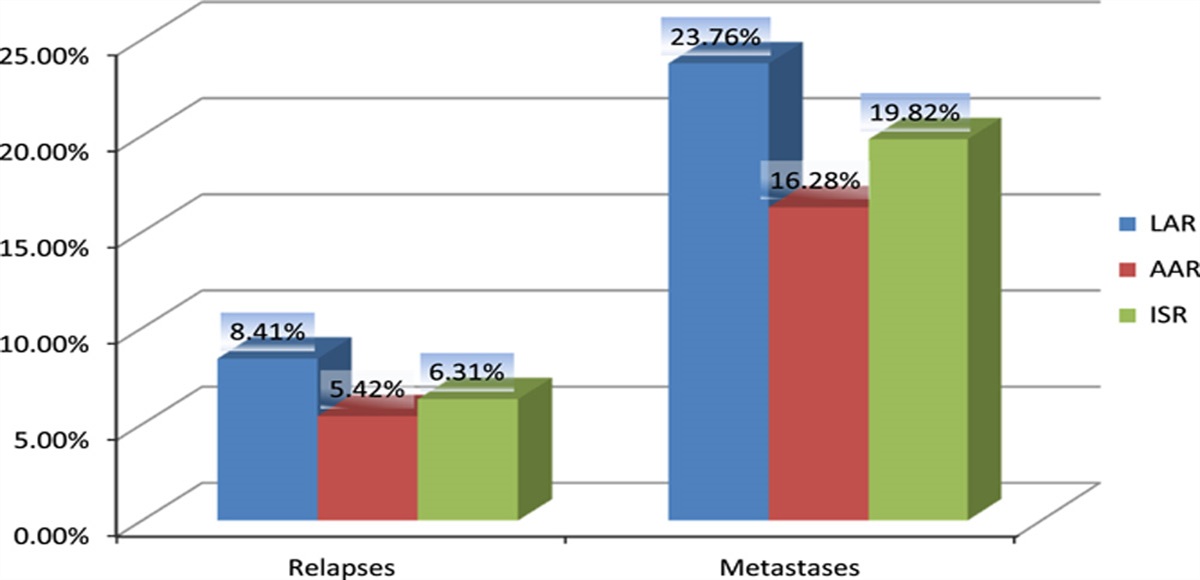
Table 2 - Clinical effect of neoadjuvant chemotherapy. PLD group (N=57) Epirubicin group (N=50) P Response to chemotherapy 0.868 cPR 37 (64.9%) 31 (62%) cCR 10 (17.4%) 8 (16%) cSD 8 (14.0%) 9 (18%) cPD 2 (3.5%) 2 (4%) Response rate (cPR +cCR) 47 (82.5%) 39 (78%) 0.563Eight (14.1%) of 57 patients in the PLD group and six (12%) of 50 patients in the epirubicin group had a pCR in breast and lymph node (ypT0/is, ypN0; P=0.756).
Analysis of adverse reactionsNausea, vomiting, alopecia, ventricular premature contractions, and decreased left ventricular ejection fraction in the PLD group were significantly lower compared to the epirubicin group. However, allergies and the hand-foot syndrome were significantly higher than the epirubicin group, as presented in Table 3.
Table 3 - Treatment-related toxicity. PLD group (n=57) Epirubicin group (n=50) Adverse events Grade 1–2 Grade 3–4 Grade 1–2 Grade 3–4 P Neutropenia 15 6 17 7 0.243 Alopecia 12 0 37 0 <0.001 Anemia 16 4 18 5 0.896 Nausea 17 0 29 0 0.003 Vomiting 11 3 17 5 0.034 Diarrhea 9 1 11 3 0.196 Hypersensitive 8 2 1 0 0.008 HFS 20 3 8 1 0.012 Cardiotoxicity PLD group (n=57) Epirubicin group (n=50) Ventricular premature beat 7 15 0.024 LVEF decline >10% 6 17 0.003Anthracyclines are cytotoxic antitumor drugs. Together with taxanes, they are currently the main drugs for breast cancer chemotherapy and are widely used to treat breast cancer. However, clinical application of anthracyclines is limited by drug-related adverse reactions, including hair loss, gastrointestinal reactions, bone marrow suppression, and cardiotoxicity. Anthracyclines can cause a variety of cardiotoxicities, including acute, chronic, and delayed cardiotoxicity14. In addition, anthracycline’s adverse reactions are dose-related, and the accumulation of the drug can cause diffuse cardiomyopathy and eventually congestive heart failure. Because of that, the use of anthracyclines is restricted in the elderly or patients with previous heart disease. In the expert consensus on the prevention and treatment of anthracyclines cardiotoxicity, it is proposed that drugs such as dextropropimine can be used to reduce the cardiotoxicity, and new strategies, like different dosages with less cardiotoxicity such as PLD, can be used. In previous studies on the rescue and treatment of metastatic breast cancer, it has been found PLD has a better curative performance and lower cardiac adverse reactions compared with traditional epirubicin therapy10. Therefore, the NCCN breast cancer treatment guidelines recommend the usage of PLD for advanced or recurrent metastatic breast cancer.
Liposomes are bimolecular small vesicles with a structure similar to biological membranes. They are vesicles with single or multiple phospholipid double-layer membranes. The main component is phospholipids. The phosphoric acid group-containing part of the phospholipid molecule has strong polarity (hydrophilic), and the hydrocarbon chain is non-polar (hydrophobic). Its advantages include the capacity of embedding and carrying drugs, having a longer half-life, and being targeted to reach the site of action, especially if the concentration of the drug distribution in the myocardium is reduced, which reduces the drug accumulation in myocardial cells15. As a new chemotherapeutic drug type with anticancer targeting features, PLD directly acts on the tumor site, increases the therapeutic effect, overcomes the defect of free doxorubicin drug cardiotoxicity, and retains the anticancer effect of doxorubicin16. Studies have shown that PLD mainly aggregates to tumor cells, maintaining a low concentration of healthy tissues and a faster aggregation rate to tumor cells than control tissues17. At the same time, the half-life of PLD is more prolonged than standard doxorubicin, and its antitumor effect is more robust18,19.
Previous studies have frequently reported the application of PLD in recurrent or metastatic breast cancer, while its application in breast cancer NAC is a novelty with very few sparse reports. The pCR rate after NAC for HER2-positive breast cancer is rising in response to the emergence of targeted drugs, but neoadjuvant therapy of HER2-negative breast cancer can only rely on chemotherapy, so the optimal choice of chemotherapy regimens are mandatory. Therefore, it is necessary to collect more data to demonstrate the role of PLD in NAC for breast cancer. In this study, the age, follow-up time, and clinicopathological characteristics of the PLD and epirubicin groups are consistent and have good comparability. The efficacy of PLD is also consistent with epirubicin. At the same time, the adverse effects of PLD chemotherapy, such as hair loss, gastrointestinal reactions, and cardiotoxicity, were significantly lower than epirubicin. Lu et al. also reported similar results20,21. In the current breast cancer chemotherapy recommendations, the combination of anthracyclines and taxanes is the traditional chemotherapy protocol, but the primary adverse reaction of taxanes is also the reduction of white blood cells. The incidence and degree of leukopenia in the PLD group are lower than the traditional approach, and the combination with taxanes can provide better safety. Hair loss is a common adverse reaction of chemotherapy. It will not affect the survival of patients, but it is significant to the patient’s psychological state. PLD therapy offers physical protection and also a comfort to the patient’s psychology, presenting better chemotherapy compliance. At the same time, the anthracycline-related cardiotoxicity is progressive and irreversible. Limiting the cumulative dose of anthracyclines can reduce the incidence of cardiotoxicity. With the low administration concentration of PLD, the drug distribution in the myocardium is reduced, and the cardiotoxicity is diminished.
In this study, due to the robust sensitization of PLD, especially the first use of patients, the common reactions were chest tightness, shortness of breath, and dyspnea. These reactions are also commonly found in previous reports of PLD use22,23. The allergic reaction can be alleviated by stopping drug infusion, starting oxygen inhalation, and antiallergic treatment, and it will not occur again when another round of PLD is restarted. At the same time, PLD treatment induces the hand-foot syndrome more significantly than epirubicin, which is consistent with previous reports. Patients mainly manifested as hand-foot rash or blisters, accompanied by erythema, swelling, and pain22,24. The PLD-induced mechanism leading to the hand-foot syndrome is credited to the longer half-life of PLD. Because fingertips and toes are rich in capillaries, the blood flow is high, and the capillaries are composed of a single layer of endothelial cells. After slight stimulation, the drug immediately penetrates through the capillary wall to the interstitial space25,26. An inflammatory state occurs into the skin’s stratum corneum, leading to vasodilation, increased vascular permeability, skin redness, heat, and swelling, which can be counterattacked by large doses of vitamin B6 and topical hormones for allergy medication for symptoms relief26.
In summary, the efficacy of PLD in NAC for breast cancer is the same as the traditional epirubicin. However, the side effects are significantly reduced, and safety is maintained, especially for the elderly or patients with previous heart disease. Additionally, more data and prospective studies are needed to corroborate the efficacy of PLD.
Ethical approvalThe present study was approved by the Ethics Committee of Xingtai People’s Hospital (No.2021[030]).
ConsentWritten informed consent was obtained from the patient for publication of this study.
Sources of fundingThe present study was supported by the Xingtai Municipal Science and Technology plan project (grant no.2021ZC148).
Author contributionL.X.Y. and S.Y.Z.: conducted the data acquisition, data analyses, and figure/table preparations; S.Y.Z., P.P.P., N.L.J., and X.W.L.: provided material input, data analysis, and assisted with revising the manuscript; L.X.Y.: supervised the experimental design and manuscript writing. All authors read and approved the final manuscript and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflicts of interest disclosuresThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Research registration unique identifying number (UIN)Our study is a retrospective study. Thank you.
GuarantorLixian Yang.
Provenance and peer reviewNot commissioned, externally peer-reviewed.
AcknowledgementsNot applicable.
References 1. Chen WQ, Zheng RS, Baade PD, et al. Cancer statistics in China. CA Cancer J Clin 2016;66:115–132. 2. Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021. CA Cancer J Clin 2021;71:7–33. 3. Abu-Khalaf MM, Harris L. Anthracycline-induced cardiotoxicity: risk assessment and management. Oncology (Williston Park) 2009;239:244–252. 4. Ryberg M, Nielsen D, Cortese G, et al. New insight into epirubicin cardiac toxicity: competing risks analysis of 1097 breast cancer patients. J Natl Cancer Inst 2008;100:1058–1067. 5. Gil-Gil MJ, Bellet M, Morales S, et al. Pegylated liposomal doxorubicin plus cyclophosphamide followed by paclitaxel as primary chemotherapy in elderly or cardiotoxicity-prone patients with high-risk breast cancer: results of the phase II CAPRICE study. BCR Treat 2015;151:597–606. 6. Xing M, Yan F, Yu S, et al. Efficacy and cardiotoxicity of liposomal doxorubicin-based chemotherapy in advanced breast cancer: a meta-analysis of ten randomized controlled trials. PLoS One 2012;167:1055–1057 7. Vito A, Daniele G, Thomas B, et al. International expert consensus on primary systemic therapy in the management of early breast cancer: highlights of the fifth symposium on primary systemic therapy in the management of operable breast cancer, Cremona, Italy (2013). J Natl Cancer Inst Monogr 2015;2015:90–96. 8. Von Minckwitz G, Untch M, Blohmer J-U. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol 2012;23:374–375. 9. Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 2014;384:164–72 10. Batist G, Harris L, Azarnia N, et al. Improved anti-tumor response rate with decreased cardiotoxicity of non-pegylated liposomal doxorubicin compared with conventional doxorubicin in first-line treatment of metastatic breast cancer in patients who had received prior adjuvant doxorubicin: results of a retrospective analysis. Anti-Cancer Drugs 2006;17:587–95. 11. Mathew G, Agha R; for the STROCSS Group. STROCSS 2021: strengthening the reporting of cohort, cross-sectional and case-control studies in surgery. Int J Surg 2021;96:106165. 12. Khokher S, Qureshi MU, Chaudhry NA. Comparison of WHO and RECIST criteria for evaluation of clinical response to chemotherapy in patients with advanced breast cancer. Asian Pac J Cancer Prev 2012;13:3213–8. 13. Nishino M, Jagannathan JP, Ramaiya NH, et al. Revised RECIST guideline version 1.1: what oncologists want to know and what radiologists need to know. AJR Am J Roentgenol 2010;195:281–289. 14. Torti FM, Bristow MM, Lum BL, et al. Cardiotoxicity of epirubicin and doxorubicin: assessment by endomyocardial biopsy. Cancer Res 1986;46:3722–3727. 15. Gabizon AA. Pegylated liposomal doxorubicin: metamorphosis of an old drug into a new form of chemotherapy. Cancer Invest 2001;19:424–436. 16. Rom J, Bechstein S, Domschke C, et al. Efficacy and toxicity profile of pegylated liposomal doxorubicin (Caelyx) in patients with advanced breast cancer. Anti-Cancer Drugs 2016;294:123–129. 17. Eckes J, Schmah O, Siebers JW, et al. Kinetic targeting of pegylated liposomal doxorubicin: a new approach to reduce toxicity during chemotherapy (CARL-trial). BMC Cancer 2011;11:337. 18. Ferrandina G, Corrado G, Licameli A, et al. Pegylated liposomal doxorubicin in the management of ovarian cancer. Ther Clin Risk Manag 2010;6:463–483. 19. Yao J, Pan S, Fan X, et al. Pegylated liposomal doxorubicin as neoadjuvant therapy for stage II–III locally advanced breast cancer. J Chemother 2020;32:1–6. 20. Lien MY, Liu LC, Wang HC, et al. Safety and efficacy of pegylated liposomal doxorubicin-based adjuvant chemotherapy in patients with stage I-III triple-negative breast cancer. Anti-Cancer Res 2014;34:7319–7326. 21. Lu YC, Ou-Yang FU, Hsieh CM, et al. Pegylated liposomal doxorubicin as adjuvant therapy for stage I-III operable. Breast Cancer 2016;30:159. 22. Fang Q, Qiu Y, Yang GJ. Clinical observation of pegylated liposomal doxorubicin in combined chemotherapy of advanced cancers. 2011;28:575–578. doi:10.1631/jzus.B1000135 23. Ingen-Housz-Oro S, Pham-Ledard A, Brice P, et al. Immediate hypersensitivity reaction to pegylated liposomal doxorubicin: management and outcome in four patients. Eur J Dermatol 2017;27:271–274. 24. Gavilá J, Oliveira M, Pascual T, et al. Safety, activity, and molecular heterogeneity following neoadjuvant non-pegylated liposomal doxorubicin, paclitaxel, trastuzumab, and pertuzumab in HER2-positive breast cancer (Opti-HER HEART): an open-label, single-group, multicenter, phase 2 trial. BMC Med 2019;17:8. 25. Martschick A, Sehouli J, Patzelt A, et al. The pathogenetic mechanism of anthracycline-induced palmar-plantar erythrodysesthesia. Anti-Cancer Res 2009;29:2307–2313. 26. Yokomichi N, Nagasawa T, Coler-Reilly A, et al. Pathogenesis of hand-foot syndrome induced by PEG-modified liposomal doxorubicin. Hum Cell 2013;26:8–18.
留言 (0)