1. IntroductionMalocclusion, along with periodontal disease and caries, is ranked as one of the three major diseases of the oral cavity by the World Health Organization (WHO). Orthodontic treatments can correct dental and jaw misalignments and improve the facial or dental aesthetics and masticatory functions, owing to the plasticity of the jaw [
1]. Improvements in the standard of living and social civilization have led to a progressive increase in the demand for aesthetics. The number of patients requesting orthodontic treatments and the proportion of adults among those undergoing orthodontic treatments are steadily increasing [
2,
3]. The complexity of the oral environment dictates that orthodontic treatments are bound to be riskier and more challenging in adults, particularly due to the increase in the incidence of periodontal disease with age.According to the WHO Oral Health Database, approximately 90% of adults have some form of periodontal issue [
4], ranging from localized mild gingivitis to generalized severe periodontitis [
5]. Orthodontic treatments are considered susceptibility factors for periodontal disease because orthodontic appliances can hinder the daily cleaning of the mouth [
6]. The periodontium continues to remain in a slightly inflamed environment during orthodontic treatment. Hence, maintaining the efficiency of orthodontic tooth movement (OTM) within a mildly inflammatory environment and ensuring a balanced remodeling of the bone are of the utmost importance during orthodontic treatment.In recent years, scientists have become increasingly interested in the possibility of replacing damaged cells in living organisms [
7]. Researchers are trying to understand the regenerative capacity of these cell populations and the potential use of these cells for immunotherapy or the treatment of various diseases, hoping to improve the immune environment and cure diseases through certain cell populations [
8]. Macrophages are a strategically located, highly plastic, and heterogeneous cell population that can rapidly change their functions in response to signals in the local microenvironment [
9]. They play an important role in regulating inflammation and bone regeneration and in mediating innate immune responses [
10,
11,
12,
13]. Furthermore, as osteoclast precursor cells, macrophages play a crucial role in bone remodeling during tooth movement [
14]. Several studies have focused on the two extreme phenotypes of macrophages: M1 and M2 polarization [
15,
16]. An imbalance in the macrophage phenotype disturbs the bone remodeling process in vivo, which may lead to challenges in enhancing the efficiency of the orthodontic treatment under mildly inflammatory conditions. However, a recent single-cell RNA sequencing (ScRNAseq) study has shown that the typical M1 and M2 phenotypes in vitro are inconsistent with the heterogeneity of the macrophages in vivo [
17]. In this regard, we wanted to target a subpopulation of phenotypically and functionally defined macrophages for use in orthodontic models.We focused on a subpopulation of macrophages with tissue-regeneration-promoting functions and high expression levels of CD301b protein [
18]. These CD301b+ macrophages overlap with the M1/M2 polarized classification and perform significant immunomodulatory and regenerative functions [
19,
20]. Therefore, these cells may play a more comprehensive role than the traditional M2-like macrophages by being involved in both inflammatory and bone-regenerative repair processes [
21,
22]. Previous studies have demonstrated that CD301b+ macrophages are necessary not only for tissue regeneration [
20], but also for bone defect repair and regeneration [
23,
24]. Therefore, it is suggested that these cells may be considered as targets for orthodontic treatment in the inflammatory environment. However, the specific mechanism remains unclear.In this study, we established an orthodontic animal model in normal and periodontal inflammatory microenvironments to compare the efficiency, bone remodeling, and metabolic levels of orthodontic tooth movement (OTM) [
25,
26]. The results showed that the inflammatory conditions hindered the effectiveness of the orthodontic treatment. Among these, the macrophages appear to be involved in key regulatory roles. Our further experiments verified that the recruitment and activation of CD301b+ macrophage subsets in the microenvironment has benefits for bone remodeling and can alleviate the adverse effects of periodontitis. CD301b+ macrophages are a promising target in orthodontic therapy. 2. Materials and Methods 2.1. Data Collection and Processing of Single-Cell Transcriptome Sequencing
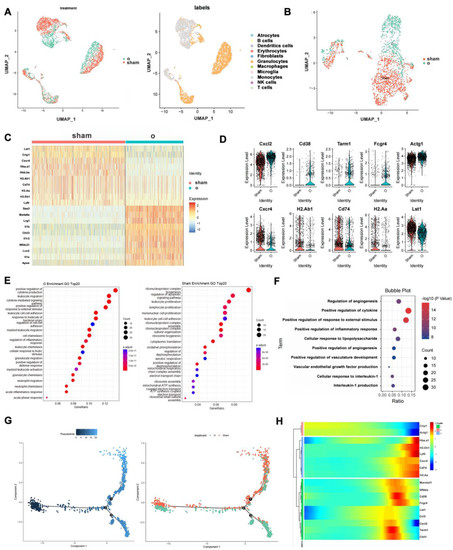
Publicly available scRNAseq datasets were obtained from the Gene Expression Omnibus DataSets (GSM5640072 and GSM5640073). The dimensionality reduction in the data was performed using the Seurat function. For quality control, cells with a percentage of mitochondrial genes below 10% and between 200 and 5000 genes detected were retained. The principal component analysis (PCA) was performed based on the 2000 top variable genes. For the FindClusters parameter, the resolution value was set to 0.5. Clusters were annotated based on the MouseRNAseqData dataset. We used the “FindAllMarkers()” function to obtain differentially expressed genes (DEGs).
2.2. Establishment of the Rat Model
The animal experiments were conducted in accordance with the policy of the Ethics Committee for Animal Research, School and Hospital of Stomatology, Wuhan University, China. The Ethics Committee for Animal Use approved the study under protocol number S0792203014. Male SD rats, weighing about 230–250 g, were used for the in vivo experiments after being acclimated to the SPF environment for one week. All animal experiments were approved by the Ethics Committee of Wuhan University. Establishment of the rat periodontitis model: After the rats were anesthetized with isoflurane, a groove of about 0.2 mm was ground on the palatal enamel of the maxillary first molar of the rat with a turbine. We used the needle holders to pass the 3-0 silk thread through the junction of the first molar and the second molar to the level of the gingival papilla, then wrapped it around the first molar and tied a knot to fix it. Establishment of the rat orthodontic model: After the rats were anesthetized with isoflurane, a groove with a depth of about 0.5 mm was ground in the distal part of the maxillary incisors of the rats with a turbine, and a 0.2 mm ligation wire was used to surround the incisors. We used a 0.2 mm ligature wire to pass under the abutment area between the first molar and the second molar and circle the first molar. We connected the ligature wire around the first molar to the ligature wire around the incisor with a tension spring and adjusted the tension to 50 g. After 12 h of postoperative fasting, food was taken and fed as usual.
2.3. Micro-CT Scans and Analysis
Bone tissue changes near the maxillary first molars were assessed using a micro-CT imaging system (Skyscan 1176). Scans were performed at 90 kV and 278 μA, the filter was Cu + Al, and the thickness of each layer was 9 μm in high-resolution mode. The tooth travel distance was measured using the DataViewer program. The CTAn program was used to calculate bone-tissue-related indicators, including the bone volume/total volume (BV/TV), trabecular bone number (Tb.N), trabecular bone thickness (Tb.Th), and trabecular bone separation (Tb.Sp). The circle around the root of the tooth was defined as the region of interest (ROI). The distance of the tooth movement was defined as the line between the distal most convex point of the first molar crown and the proximal most convex point of the first molar crown.
2.4. Histological Staining
The maxillary bone of each rat was taken as the specimen. The specimens after taking micro-CT images were placed in a decalcification solution containing 15% EDTA for 1 month, until the needle could penetrate the bone tissue without resistance. The specimens were dehydrated in a gradient manner, and the procedure was 70%, 80%, 90%, and 95% I and 95% II concentrations of alcohol for 2 h in sequence. The specimens were placed in n-butanol overnight and then dipped in wax and embedded the next day. The slice thickness range was chosen to be 5–8 μm. The specimen sections were placed in a 60 °C oven for 2 h before dewaxing. The sections were washed 3 times with PBS for 3 min each. For the H&E staining (Google Biotechnology, China), we used a hematoxylin staining solution for 10 s and then rinsed the sections with water for 1 min. Then, they were stained with eosin for 8 s and destained with 75% alcohol for 6 s. For the Masson staining (MXB Biotechnologies) and TRAP staining (MXB Biotechnologies), we followed the instructions in the manual.
For the immunohistochemical staining, the sections were first incubated with a drop of antigen retrieval solution at 37 °C for 30 min, then washed three times with PBS. Next, a drop of peroxidase blocking agent was added and they were incubated at 37 °C for 10 min and washed three times with PBS. Then, we added the serum and performed blocking at 37 °C for 1 h. We added the antibody solution (diluted 1:200 in PBS) and incubated the sections overnight at 4 °C. The next day, they were washed three times with PBS, then we added the biotin-labeled secondary antibody and them incubated at 37 °C for 1 h. We then washed them three times with PBS, added streptavidin–avidin peroxidase solution, and incubated them at 37 °C for 20 min. We then washed them three times with PBS, added a drop of freshly prepared DAB solution, and waited for 1 min. We then rinsed them with PBS and performed hematoxylin staining. For the IHC staining, the primary antibodies were IL-6 (Bio-Swamp, Shanghai, China), Col1a1 (Bio-Swamp, Shanghai, China), and TNF-α (Bio-Swamp, Shanghai, China).
For the immunofluorescence staining, the sections were first incubated with a drop of antigen retrieval solution at 37 °C for 30 min and then washed three times with PBS. Then, we added serum and blocked the sections at 37 °C for 1 h. Next, we added the antibody solution (diluted 1:200 in PBS) and incubated them overnight at 4 °C. The next day, we washed them three times with PBS, added the fluorescent secondary antibody (1:200 diluted with PBS), and incubated them at 37 °C for 1 h. They were then washed three times with PBS, mounted with DAPI-containing mounting medium, and stored at −20 °C.
2.5. Flow CytometryThe periodontal tissue samples on the buccal and lingual sides of the maxillary first molars of each rat were excised with a scalpel and collected in a 24-well plate. We cut the tissue samples into pieces with scissors, added 1 mL of digestion solution (RPMI medium containing 20% collagenase type II and 20% collagenase type IV), and incubated them at 37 °C for 2 h. The tissue fluid was ground on a 70 μm filter under PBS washing, and the filtrate was collected and centrifuged at 2500 r for 5 min. The cells were transferred to a round-bottom 96-well plate and washed once with PBS, then the supernatant was spin-dried. We then added 50 µL of antibody solution (see
Table 1), CD45 AP-cyanine7(Cy7) (Biolegend, San Diego, CA, USA), CD11b Pacific Blue (Biolegend, San Diego, CA, USA), F4/80 PE-cyanine7(Cy7) (Biolegend, San Diego, CA, USA), CD301b phycoerythrin (PE) (Biolegend, San Diego, CA, USA), and CD206 FITC (Biolegend, San Diego, CA, USA) and incubated them at 4 °C for 30 min. They were then centrifuged at 2500 r for 5 min and the supernatant was shaken off. After resuspending them in PBS and filtering them through a 70-micron filter, they were detected using a BD flow cytometer. The data analysis was performed using FlowJoc10.4 (Ashland, MA, USA) software. 2.6. Extraction and Culture of Primary Cells
Male SD rats of about 250 g were used and sacrificed after isoflurane anesthesia. The femur and tibia were cut off, and the attached muscle was stripped. After rinsing with PBS, we cut both ends of the backbone. The bone marrow was flushed out with a 20 mL syringe filled with the medium and collected into centrifuge tubes. We performed centrifugation at 1000 r for 5 min and discarded the supernatant. We added red blood cell lysate for 3 min, centrifuged the samples at 1000 r for 5 min, and discarded the supernatant. The cells were cultured in a 10 cm cell dish in DMEM high-glucose medium containing 100 U mL−1 penicillin, 100 μg mL−1 streptomycin, and 20% serum. Two days later, the supernatant in the cell dish was collected and the cells were taken after centrifugation to continue the culture. M-CSF (20 ng/mL) was added to obtain the BMDM. The adherent cells in the cell dish were further cultured to obtain BMSCs.
2.7. Real-Time Quantitative PCR
The P2 BMSCs were spread in a flexible six-well plate (FX-5000, Burlington, NC, USA), and after their cells were fused to 70%, the medium containing osteogenic induction solution (50 mL BMDM containing 10% FBS, 500 µL β-gp, 50 µL dexamethasone, 100 µL VC) was added and the cells were stretched using a device that stretches the cells (Flexcell, Burlington, NC, USA) for 48 h, then the culture was continued until the tenth day. The fluid was changed every three days.
We added 1 mL of TRIzol to each well of the six-well plate to extract the total cellular RNA. The corresponding cDNA was obtained using the Vazyme reverse transcription kit. The qRT-PCR system was loaded using Vazyme Taq Pro Universal SYBR qPCR Master Mix, and we detected the results using the CFX Connect system (Bio-Rad). Specific primers were purchased from Wuhan TianyiHuiyuan Biotechnology Co., Ltd. (Wuhan, China). All results were normalized based on the housekeeping gene glyceraldehyde-3-phosphate dehydrogenase (GAPDH). The primer sequences used in the qRT PCR process (5′ to 3′) are shown in
Table 2: 2.8. CD301b+ Macrophage Transfusion
Rat primary BMDM samples were extracted and cultured for seven days to make them mature macrophages. Subsequently, the cultured mature BMDM samples were sorted by flow cytometry using ARIA BD. The CD301b+ macrophages and CD301b- macrophages were collected in 15 mL centrifuge tubes and resuspended in 100 µL of serum after centrifugation. The two types of cells were injected into the subgingival areas of orthodontically mobile teeth on both sides with well-established periodontitis orthodontic models. For each group of 10 rats, 10 µL was injected into each side. Approximately 200,000 cells were counted. This operation was repeated on days 0, 3, and 7 of the orthodontics for different cell reinfusion results.
2.9. ALP and Alizarin Red S Staining
The P2 BMSCs were plated in flexible six-well plates, then after the cells were fused to 70%, the osteogenic induction solution was added and cells were subjected to 48 h tension and the culture process was continued with the medium being changed every three days. After ten days of culture, the PBS samples were washed three times and stained with alizarin red and ALP staining reagents for calcified nodules, respectively, as well as for their ALP activity assay. Microscopic observations were then performed.
2.10. Enzyme-Linked Immunosorbent Assay (ELISA)
Orbital blood samples were collected from the rats in the experimental group and the blank control group. The blood samples were collected in 1.5 mL centrifuge tubes, and after standing for 2 h at 4 °C, the upper layer of serum was taken into new 1 mL centrifuge tubes and stored in a −80 °C refrigerator. The serum was then shipped on dry ice to the reagent manufacturer. The bone metabolic parameters were measured in each group using an ELISA kit (Bioswamp, Shanghai, China) according to the kit manufacturer’s protocol.
2.11. CCK-8 Proliferation Assay and Cell Scratch Assay
In total, 3000 cells were added to each well of a 96-well plate, then 10 μL of CCK-8 reagent (Dojindo, Kumamoto, Japan) was added to the 96-well plate at 12 h, 48 h, and 72 h of incubation, respectively, and the OD value was measured at 450 nm using a microplate reader (Thermo, Waltham, MA, USA) for 1 h at 37 °C.
The P2 BMSCs were incubated in six-well plates for 24 h and then scratched with a sterile 200 µL pipette tip. The cells were washed with PBS to remove any debris. Photographs were taken at 0, 6, 12, and 24 h post-wounding. The gap distance was assessed quantitatively using software such as ImageJ (National Institutes of Health).
2.12. Data Statistics and Analysis
All data are presented as means ± standard deviations. The t-test was used for the analysis of significance between the two groups, and an analysis of variance was used for three or more groups. A data analysis and image rendering were performed using GraphPad Prism 8.4 (Boston, MA, USA) software.
2.13. Availability of Data and MaterialsAll data generated or analyzed during this study are included in this published article and its
Supplementary Information Files. All primary data supporting the results of this study can be obtained from the corresponding author upon reasonable request. 4. DiscussionAmong the many immune cells in the body, macrophages have received extensive attention in terms of the physiological and pathological processes that occur within the body owing to their complex functions. In this study, a single-cell sequencing analysis revealed the role of macrophages in regulating OTM and the microenvironment during orthodontic treatment. Subsequently, two models of OTM in periodontitis and normal settings were created for comparison; the macrophages were polarized toward the conventional classification M1, resulting in diminished OTM distances, as reported previously [
27]. Furthermore, in a mildly inflamed environment, the mechanical forces were found to slow down osteogenesis, osteoblast formation, and bone metabolism, which are detrimental to OTM.At present, many scientists want to change the environment of the disease through a certain cell population, so as to achieve the purpose of curing the disease [
7]. Macrophages have a wide range of functions such as innate defense, foreign body recognition, phagocytosis, inflammation regulation, and tissue repair [
28,
29,
30]. Unlike the traditional classification of macrophages (M1 and M2) [
31], a group of macrophages with high expression levels of CD301b focused on regulating the immune and regenerative functions has been recently identified [
18,
20]. In the present study, these cells were closely related to OTM. CD301b+ macrophages positively regulate the rate of OTM and the periodontal microenvironment; additionally, they promote osteogenesis in orthodontic environments, thereby altering bone metabolism and enhancing bone remodeling.Alveolar bone remodeling during OTM is a highly regulated process; it is a combination of local reversible damage to periodontal tissues and restoration under the influence of orthodontic forces [
32] Alveolar bone remodeling alters the periodontal microenvironment and coordinates bone resorption by osteoclasts and new bone formation by osteoblasts [
33]. First, a cavity is formed via bone resorption on the compressed side of the mobile tooth periodontium, followed by new bone formation within the cavity; on the tension side, mainly distraction osteogenesis is observed [
34]. Bone resorption and new bone formation around mobile teeth contribute to the movement of the tooth under orthodontic forces. Macrophages are a heterogeneous group of cells, and significant phenotypic and functional differences have been observed among macrophages within the same tissue and among those in different tissues [
35,
36,
37]. Activated macrophages produce various cytokines that can regulate or stimulate osteoclasts or osteoblasts to mediate the occurrence of associated bone loss or bone regeneration [
31].During orthodontic treatment, periodic orthodontic forces are applied to the teeth and transmitted to the periodontal tissues. The periodontal cells release mediators that alter the local bioenvironmental signals in the periodontium [
38,
39,
40], which can interact with the immune system to promote the polarization of the macrophages. Polarized macrophages are involved in the biological response to OTM, which ultimately prepares the tooth to move to a new position during periodontal restoration by remodeling the alveolar bone. In the present study, the effects of the two types of macrophages varied with the sites during OTM and the different stages during the treatment process. Type-M1-like macrophages in the traditional classification promote inflammation during tooth movement via the expression of TNF-α and inducible nitric oxide synthase (iNOS) [
41], whereas type-M2-like macrophages play an important role in angiogenesis, anti-inflammatory factor secretion, and the promotion of tissue repair regeneration and wound healing [
42,
43]. For orthodontic treatments in inflammatory environment, the traditional classification of macrophages, as M1-like or M2-like, has advantages and disadvantages for bone reconstruction during orthodontic treatment. This classification does not strictly represent a macrophage phenotype that can modulate the microenvironment and promote OTM in a mildly inflammatory setting. If a large number of macrophages of a certain phenotype are imported to regulate bone remodeling, promote tooth movement, and enhance orthodontic efficiency, they can cause an imbalance in bone metabolism, which may result in a series of adverse effects, such as root resorption. Therefore, it is difficult to be a new target for orthodontic treatment under this type of macrophage typing in mild inflammatory environments.In contrast, the new classification of macrophages, which is distinguished from the traditional classification, was used to describe the phenotype of macrophages from different perspectives in this study. To some extent, the obtained subsets overlapped rather than remained independent. The CD301b+ macrophages in the new classification contain a partial M1-like macrophage subset and a partial M2-like macrophage subset. Therefore, these macrophages possess the activities of both the M1-like (regulation of osteolysis and immunity) [
44,
45,
46] and M2-like (regenerative repair and osteogenesis) macrophages [
47,
48,
49]. In mildly inflammatory microenvironments, they respond positively to mechanical forces, enhance bone metabolism, and promote bone remodeling, thereby shifting the microenvironment towards a direction suitable for OTM. The results of the present study suggest that CD301b+ macrophages are tailored under the guidance of this goal.
The regulation of CD301b+ macrophages in bone remodeling under mechanical force during OTM has not been thoroughly studied. One of the limitations of this study is that the CD301b+ macrophages were obtained by sorting bone-marrow-derived macrophages. Thus, additional in-depth studies on the construction and functional validation of this fraction of macrophages and the corresponding condition-deficient rats with regenerated CD301b+ macrophages will have broader applications and extensive research values.
This study is an innovative exploration of the mechanism by which CD301b+ macrophages regulate OTM in an inflammatory environment. To the best of our knowledge, this is the first study to show that CD301b+ macrophages play an important role in OTM by promoting osteogenic differentiation. Macrophages with high expression levels of CD301b protein positively regulated the efficiency of OTM in a mildly inflammatory environment and the microenvironment during orthodontic treatment. This study provides a new idea for orthodontic treatment in inflammatory environments. However, more research is needed to explore the mechanism.



留言 (0)