The present study performed a detailed characterization of SO in clinical profiles, LV remodeling, and clinical outcomes in patients with HFrEF concomitant with DM. Our results supported the existence of a distinct SO phenotype with a poor prognosis within the spectrum of this entity. The main findings of this study are summarized as follows: (1) Despite having a similar NYHA functional class, compared to those with obesity but without sarcopenia, patients with SO had a greater level of NT-proBNP but a lower level of albumin. Moreover, patients with SO were more likely to have a more advanced disease progression of DM in comparison with those with sarcopenia alone. (2) Patients with SO displayed greater LV expansion and more profound LV dysfunction, together with an increase in LVM, resulting in eccentric cardiac remodeling. (3) Among HFrEF patients with DM, SO status was associated with a poor disease prognosis, indicated by an approximately 3-fold greater risk of experiencing adverse outcomes than those with neither sarcopenia nor obesity.
Clinical profiles of patients with SO
Obesity is highly prevalent in patients with HFrEF, with approximately 40–50% of patients having either overweight or obesity status [20]. Although obesity has been repeatedly shown to be a major independent risk factor for developing HF, the “obesity paradox” phenomenon seems to exist, as indicated by a better HF prognosis among patients with obesity, making the interaction between obesity and HF, especially HFrEF, more confusing [3, 21,22,23,24,25,26]. In recent years, the study of body composition changes may have helped to elucidate the survival benefit underlying the protective effect of a greater BMI on disease prognosis for HFrEF patients [4, 5].
DM and obesity often occur concomitantly, and both DM and obesity closely interact with each other. Since DM can reduce muscle protein synthesis, it is necessary to evaluate SO in the context of HFrEF with coexisting DM. HF patients with obesity display lower levels of natriuretic peptides than nonobese patients, which has been attributed to enhanced degradation of natriuretic peptides in adipose tissue [21]. In our study, only patients with obesity without sarcopenia had expectedly lower median levels of NT-proBNP than their nonsarcopenic/nonobese counterparts. In contrast, we observed remarkably elevated levels of NT-proBNP in patients with SO compared to those in patients with obesity without sarcopenia. The exact reasons for this observation remain unclear. The loss of lean muscle mass together with excess adipose tissue deposition may fail to prevent plasma volume expansion, resulting in increased wall stress and increased natriuretic peptide production. Moreover, we noticed that the serum albumin concentration was lower in patients with sarcopenia than in those without sarcopenia, regardless of BMI, which indicated that patients with sarcopenia were malnourished. However, this finding is partially reasonable for SO patients. In fact, for patients with SO, this abnormality may further suggest a metabolic imbalance in which obesity is involved. Current evidence shows that alterations in hormones, such as adiponectin and leptin, in the context of obesity may play a prominent role in anabolic–catabolic imbalance [27,28,29]. In clinical practice, the phenotype of SO, but not sarcopenia alone, could be easily ignored, since patients with SO present with a considerably increased BMI, which seems to indicate a relatively robust metabolic substrate. Therefore, recognizing the specific features of SO is necessary for clinicians to identify potential treatment targets.
LV remodeling in patients with SO
Obesity is considered to contribute to an increase in total blood volume in HF patients. The augmentation of blood volume and cardiac output thereby predisposes patients to LV enlargement and eccentric remodeling [30]. However, the alterations involved in LV remodeling in patients with SO are not entirely understood. In our study, elevated LV volumes were observed in patients with SO, accompanied by increased LVM and more prominently impaired LV contractile function across the study cohort. This observation was in keeping with our previous study, which demonstrated that a lower SMI was associated with ‘nonfunctional’ LV hypertrophy [9]. Moreover, despite the comparable LVH between patients with sarcopenia with and without obesity, we found that the former displayed a more exacerbated decline in LV contractile function. Our study further expanded upon these findings to identify more pernicious types of adverse cardiac remodeling and dysfunction. Perhaps the onset of sarcopenia among diabetic patients with HFrEF implies the progression of HF as well as DM, and obesity promotes this process through the release of proinflammatory adipokines, thereby leading to cardiac inflammation, myocardial ischemia and interstitial collagen deposition [21]. In this sense, regarding diabetic patients with HFrEF, thoracic muscle size assessment along with cardiac structure and function assessment are necessary, which is helpful for identifying patients with SO.
SO status and disease prognosis
The results of our study showed a worse prognosis in patients with SO than in patients with neither sarcopenia nor obesity. This finding was consistent with a previous study by Saito et al., who reported that SO status is a risk factor for adverse outcomes in the general elderly population with HF [31]. More importantly, since sarcopenic/non-obese individuals also had an increased risk compared to non-sarcopenic/non-obese individuals, while individuals with SO presented a more advanced disease progression of DM than individuals with sarcopenia alone, our study further provided evidence that SO phenotype may be more severe than that of sarcopenia alone in diabetic patients with HFrEF. Therefore, it could be just a reflection of SO as a specific phenotype beyond sarcopenia. In fact, SO patients with decreased skeletal muscle mass and increased fat mass have been reported to have impaired cardiorespiratory fitness, contributing to frailty and activity of daily living disability [20]. A sedentary lifestyle further aggravates DM and promotes insulin resistance, which in turn leads to a vicious cycle of skeletal muscle loss and adipose deposition [12]. It has been reported that reduced skeletal muscle mass may contribute to decreased total and central blood flow, which produces lower stroke volume and thereby cardiac output [20]. Furthermore, the paracrine and endocrine effects of adipose tissue on the muscle bed could result in impaired perfusion and inflammatory infiltration [32, 33]. Together, these pathological processes may induce myocardial ischemia and lethal arrhythmia and eventually cause adverse outcomes. Therefore, in patients with HFrEF and DM, skeletal muscle mass assessment should be performed routinely to identify risk and stratify patients with HFrEF and DM by obesity status. Additionally, our study also highlights the additional advantages of using MRI not only in cardiac structure and function but also in skeletal muscle mass assessment.
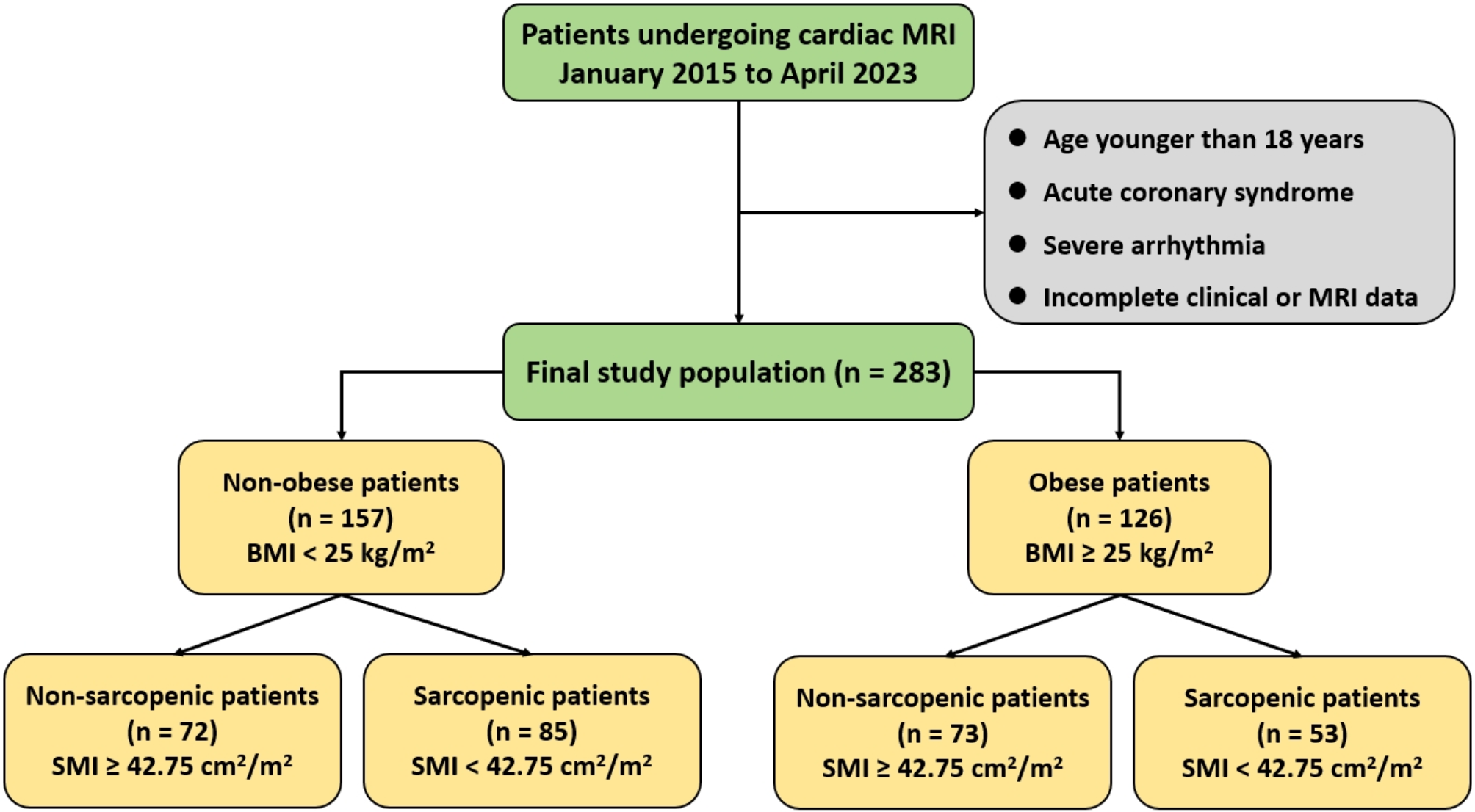
Study limitations
Our study also has several limitations. First, in the present study, we used a simple alternative index that has been confirmed by the above-mentioned studies to have prognostic value for detecting muscle mass reduction rather than traditionally used appendicular muscle mass [4, 9, 18]. Because this quantification assessment is readily available in subjects undergoing MRI scanning for cardiac structure and function assessment. Moreover, lower limbs skeletal muscle may be more subject to deconditioning [4]. Second, there are differences in the criteria for obesity between Westerners and Asians due to differences in ethnic background. We classified our patients using the criteria specified for use with Asian. However, regardless of the differences in the classification of obesity, we found that SO was related to adverse outcomes in patients with HFrEF and DM. The generalizability of this disease state to different populations needs to be further verified. Third, several new anthropometric measures, such as the waist-to-height ratio or waist-to-hip ratio, have also been used as biomarkers to reflect changes in body composition [34]. However, these measurements were unavailable in this study due to its retrospective nature. Forth, since this was a retrospective observational study, selecting bias was inevitable. Finally, we didn’t record the baseline data regarding other microvascular complications of DM in this study.





留言 (0)